-
-
LOGIN SCREEN
-
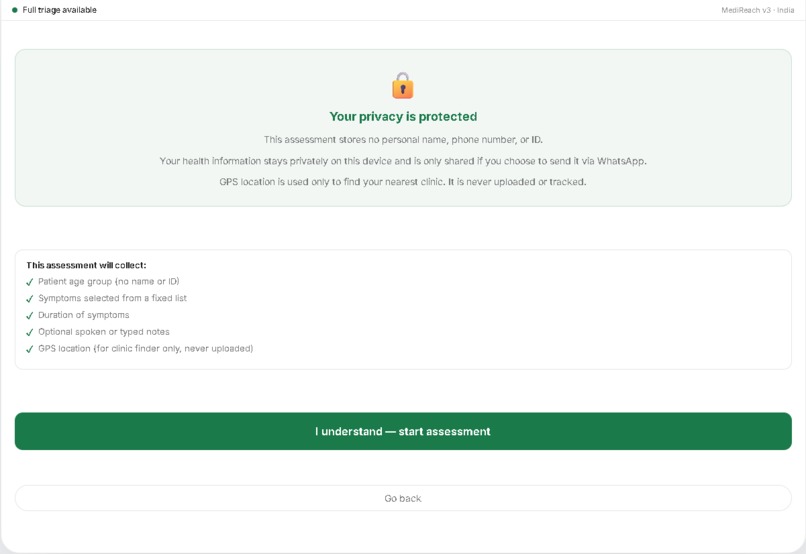
CONSENT SCREEN
-
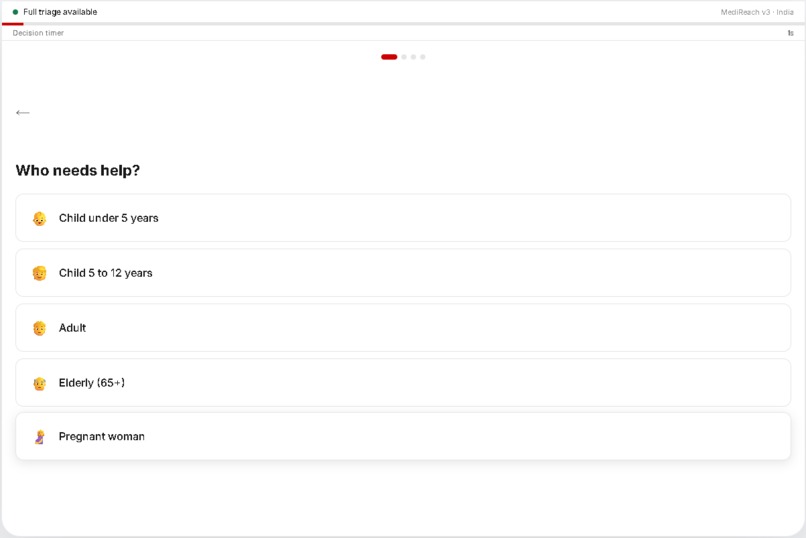
AGE SCREEN
-
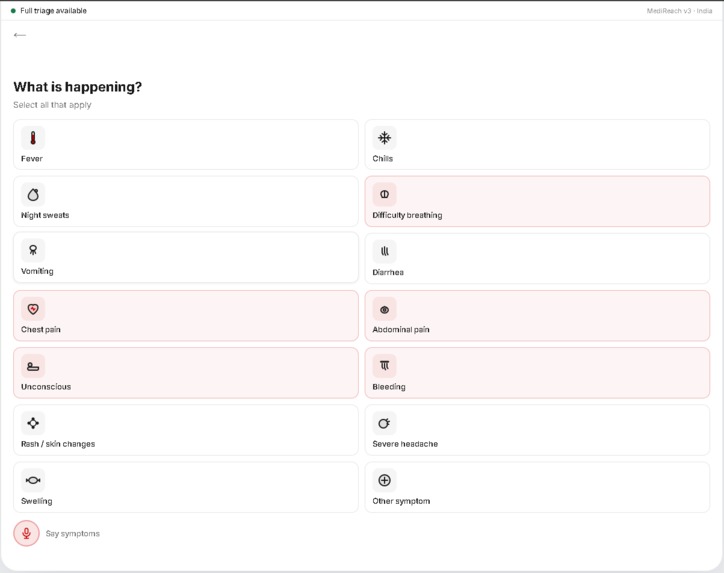
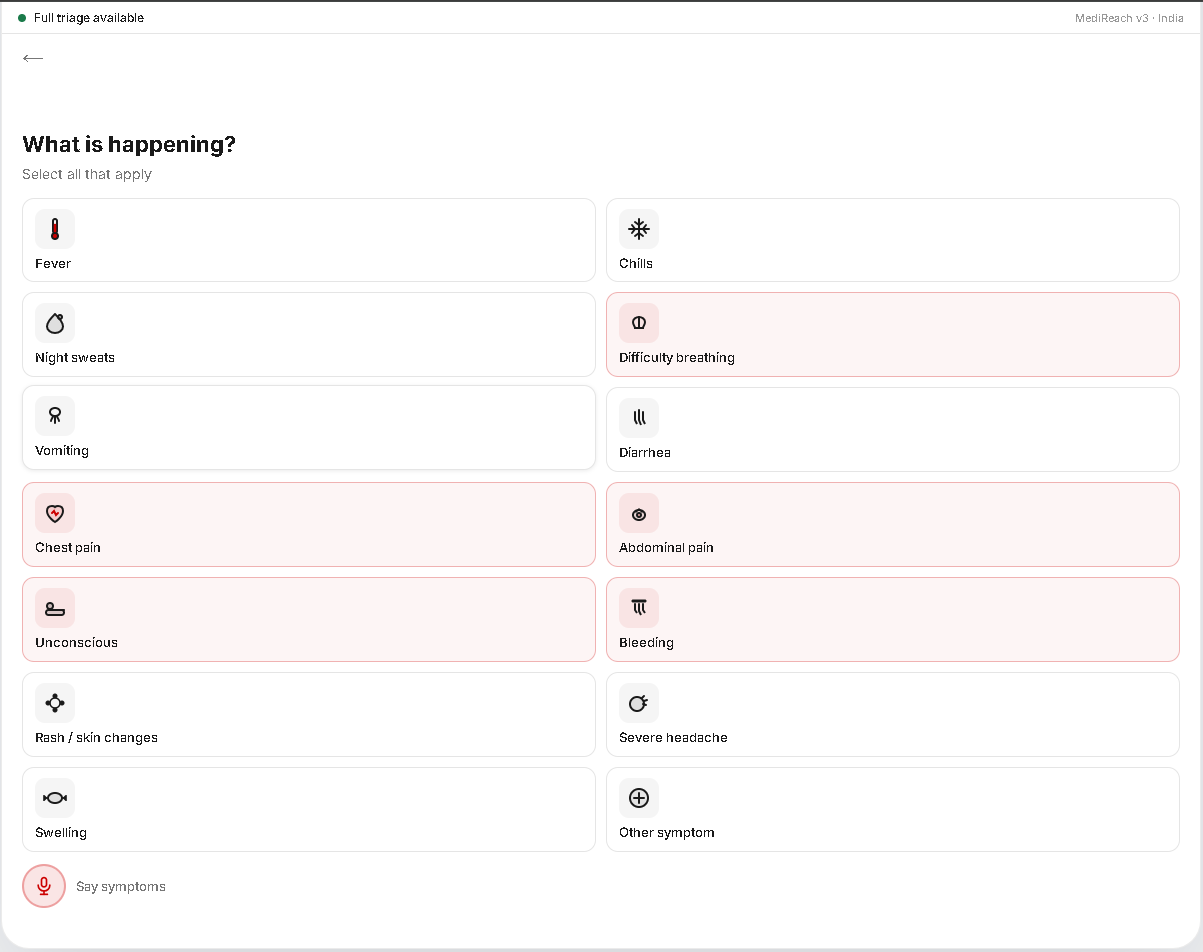
SYMPTOMS SCREEN
-
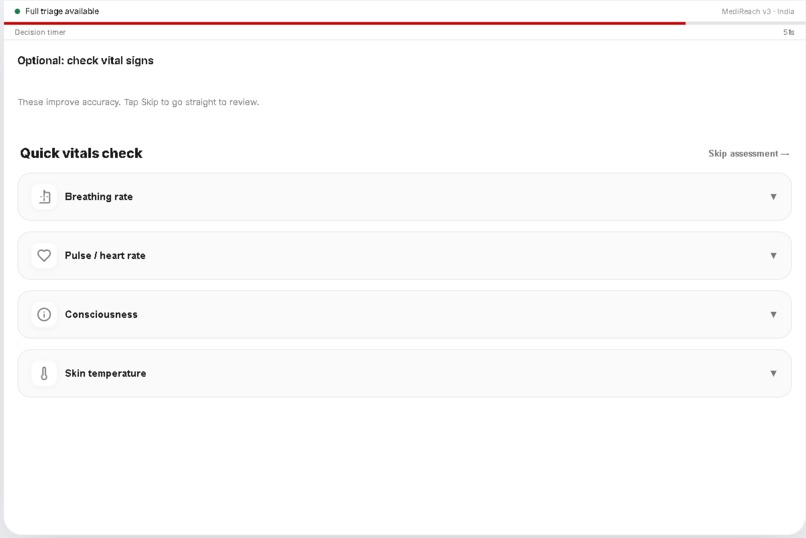
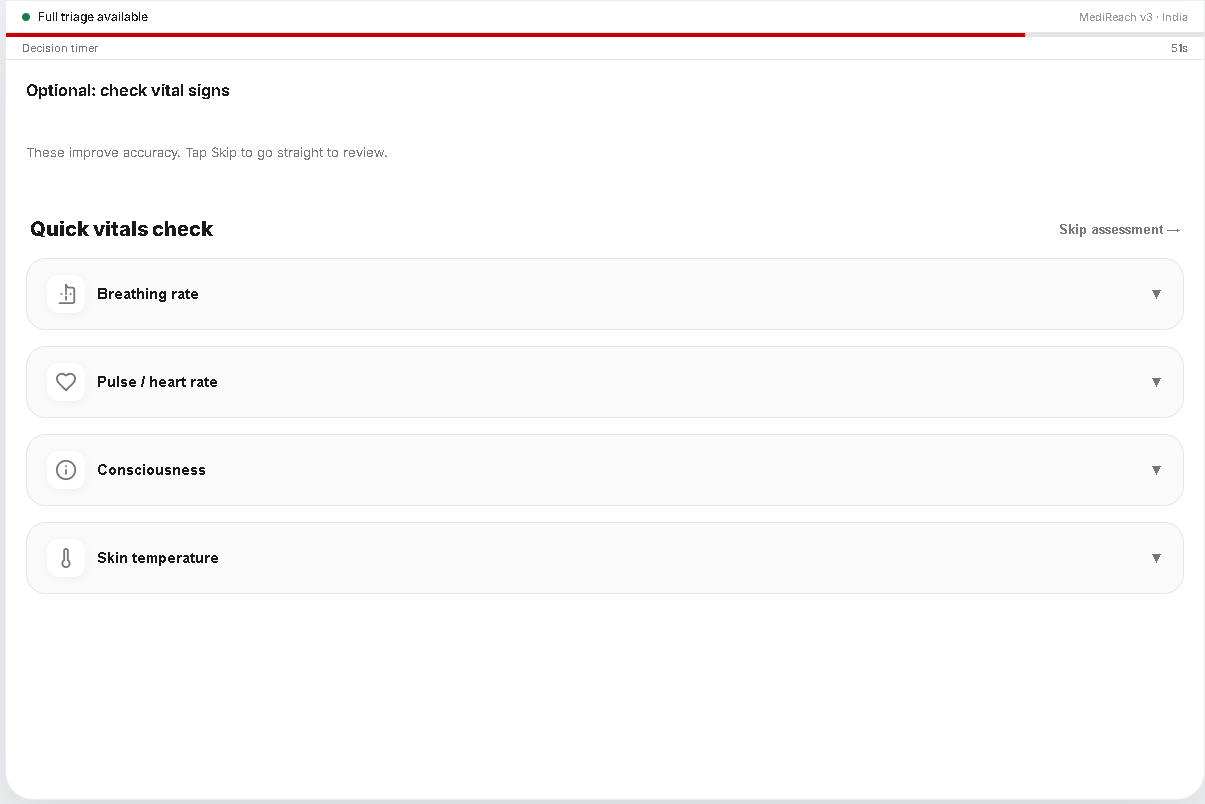
OPTIONAL VITALS SCREEN
-
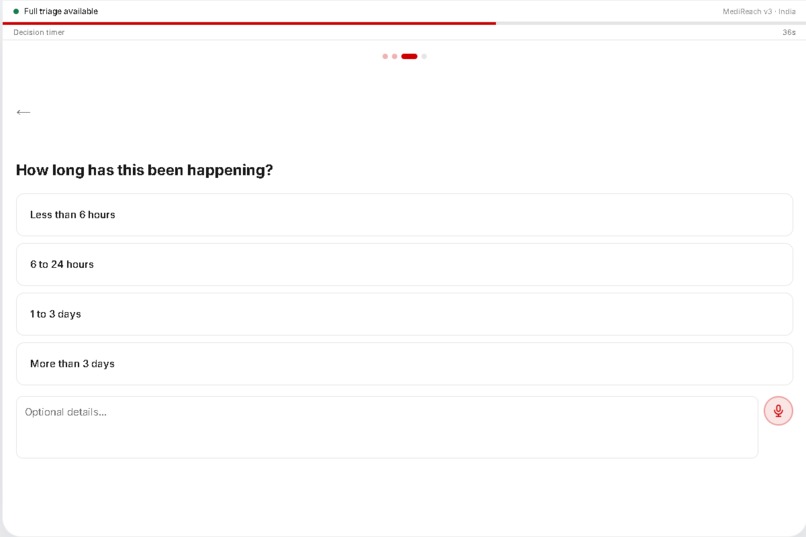
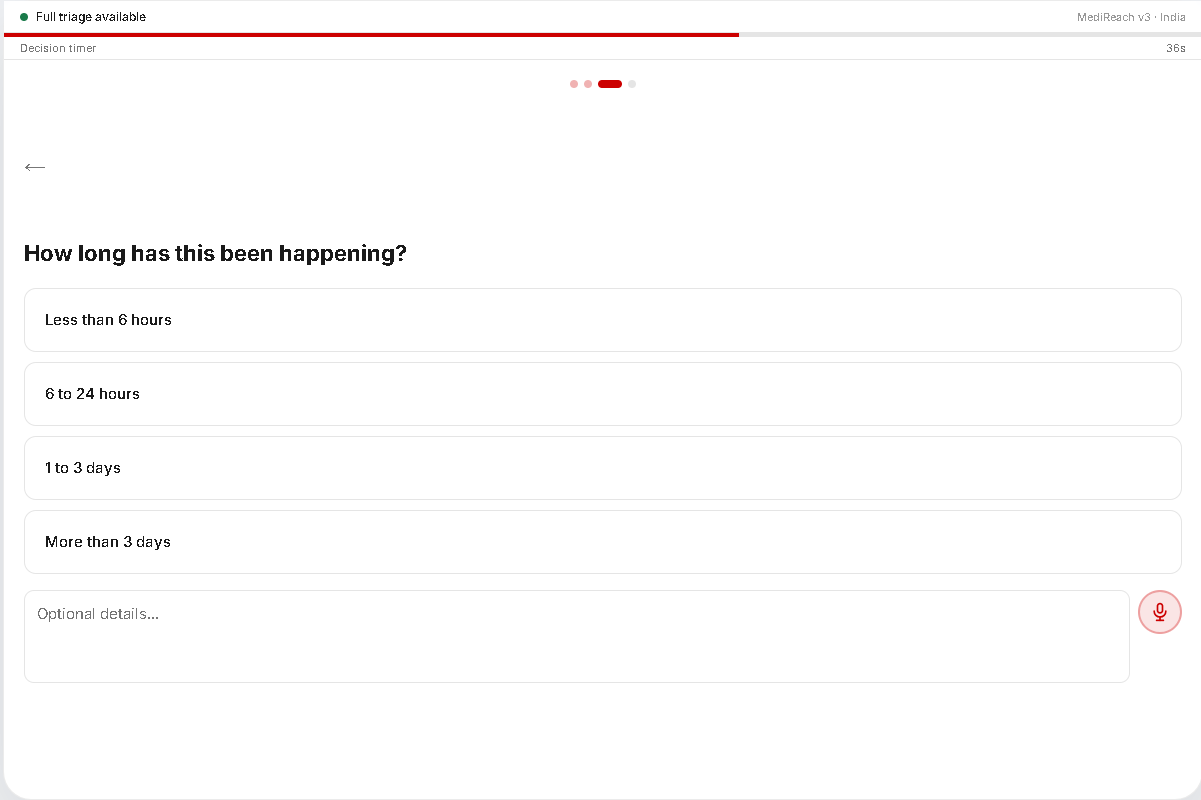
DURATION SCREEN
-
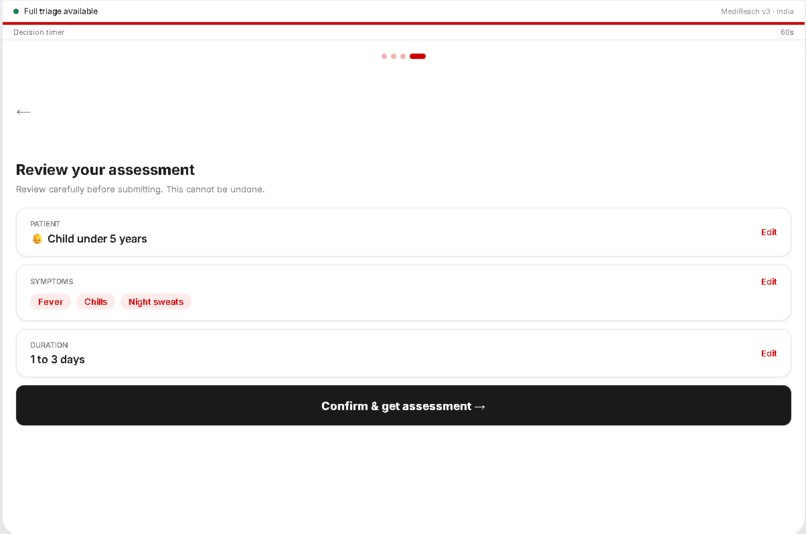
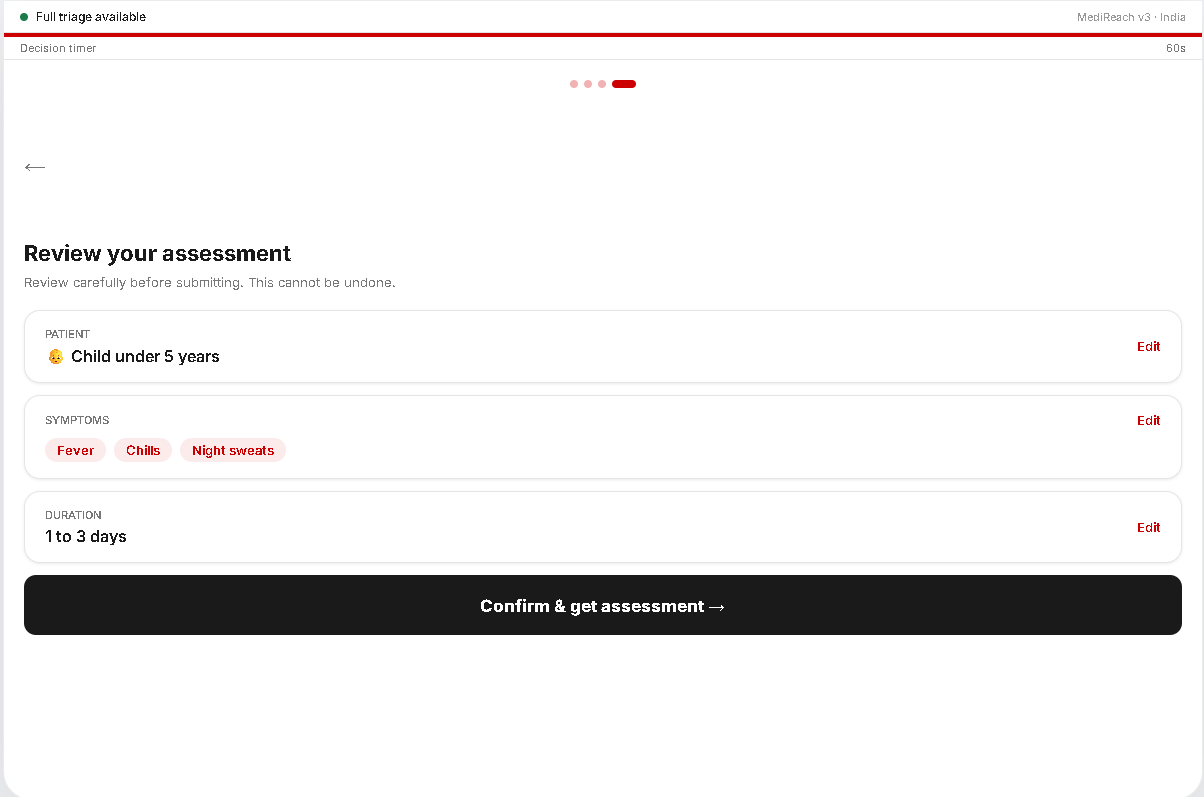
CONFIRMATION SCREEN
-
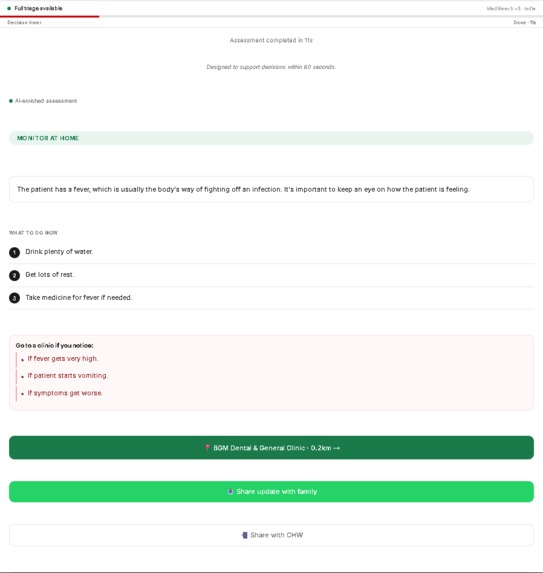
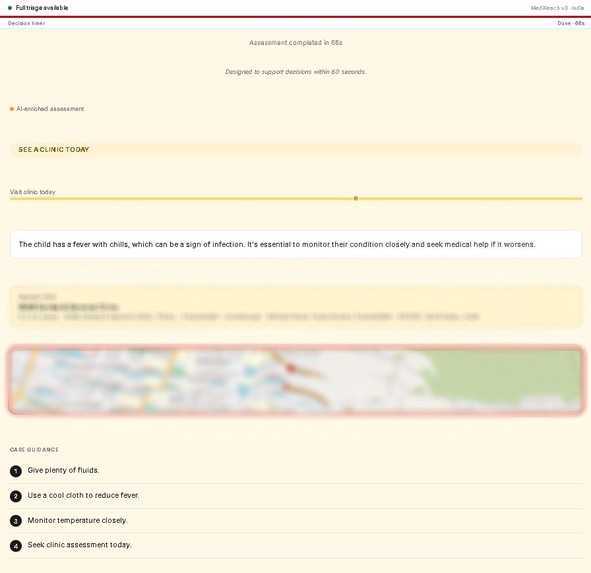
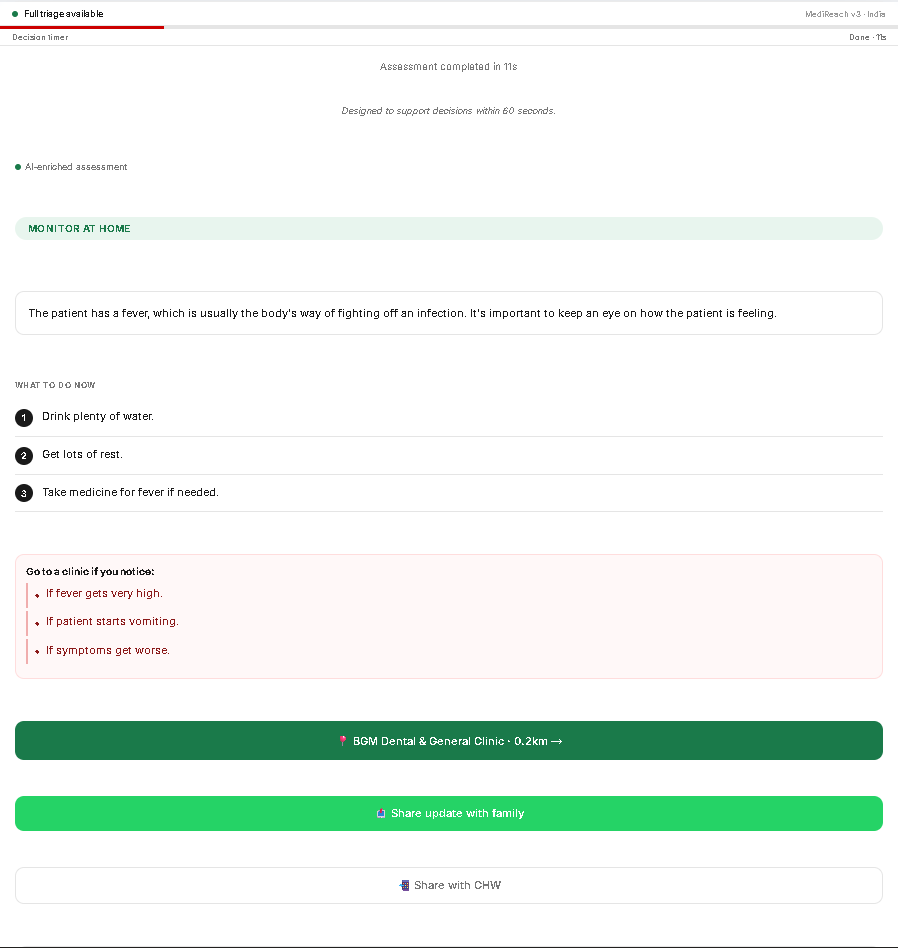
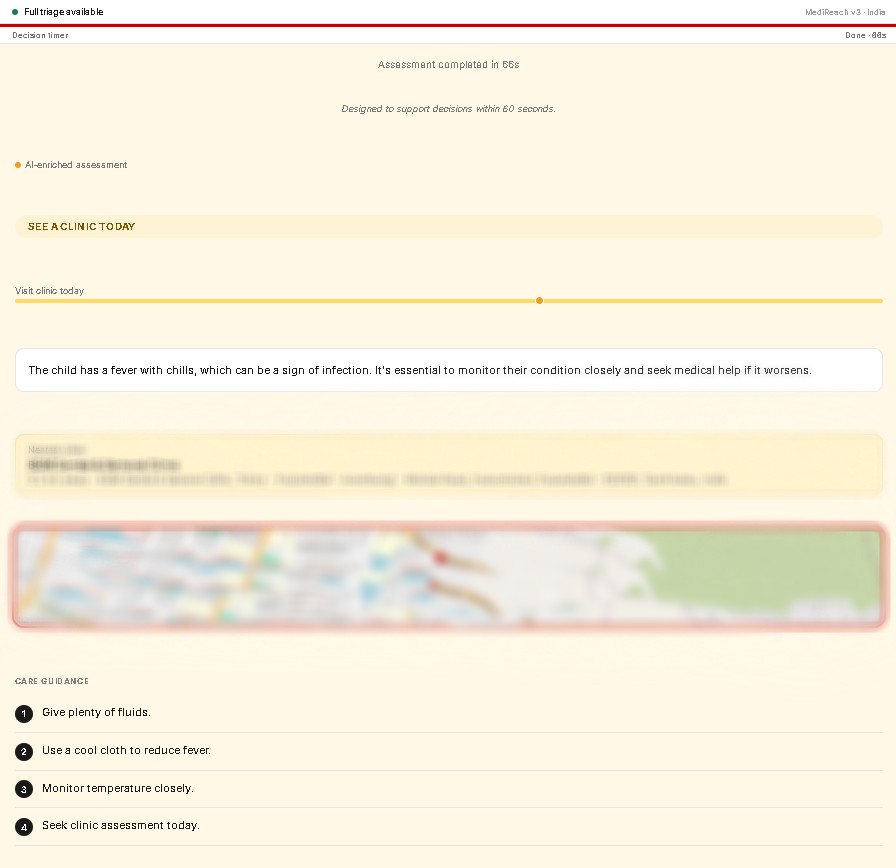
FINAL REPORT GREEN
-
FINAL REPORT AMBER
-
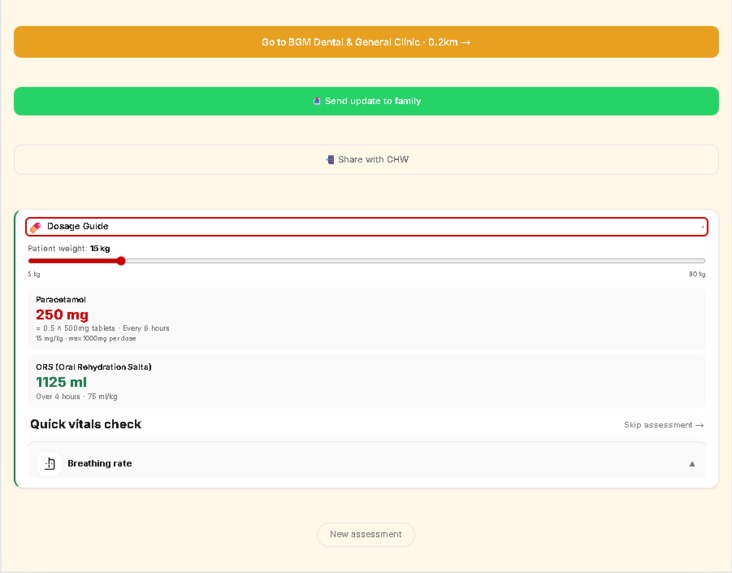
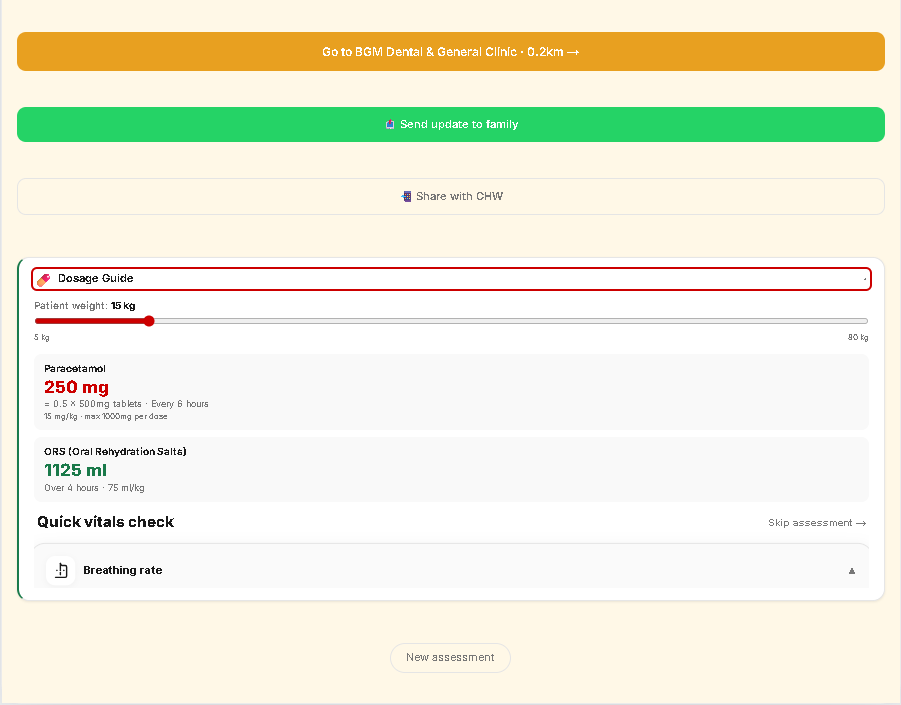
DOSAGE RECOMENDATION
-
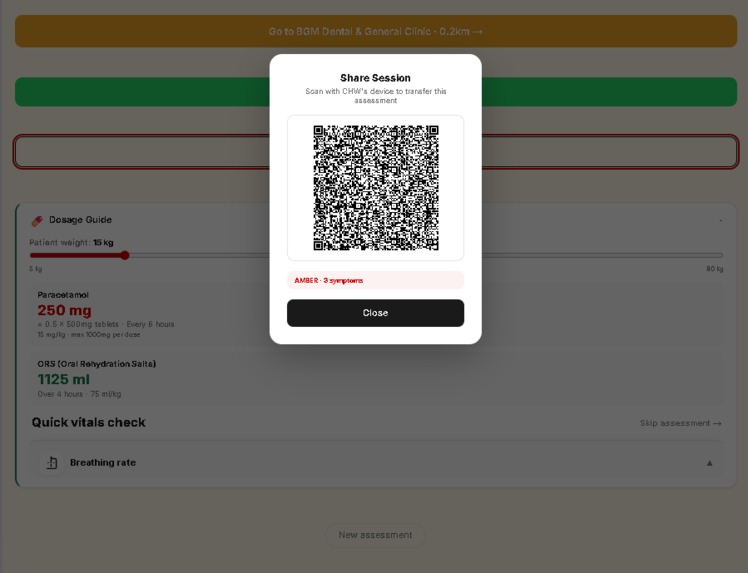
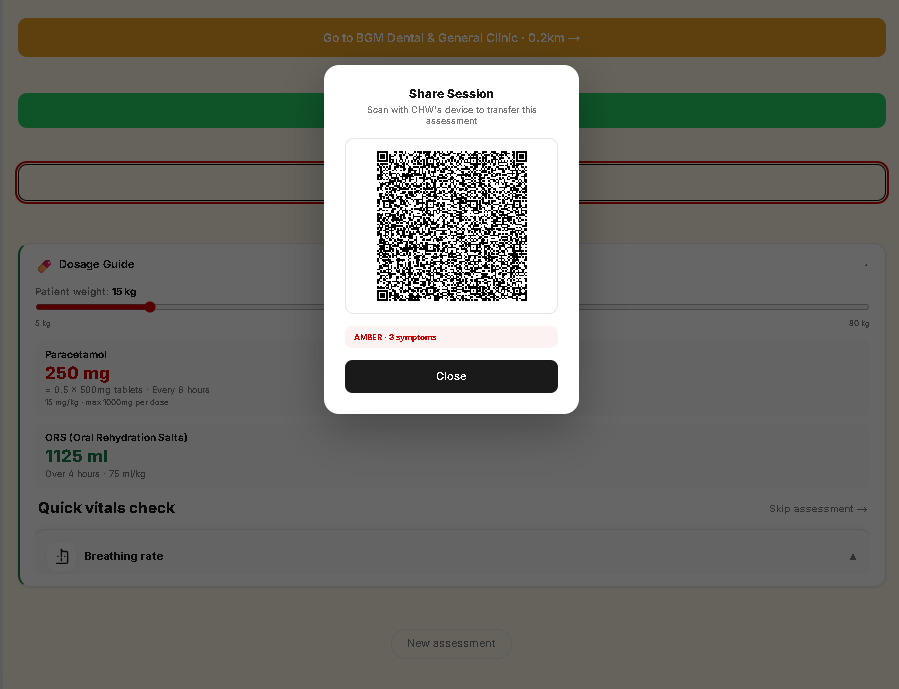
CHW QR CODE
-
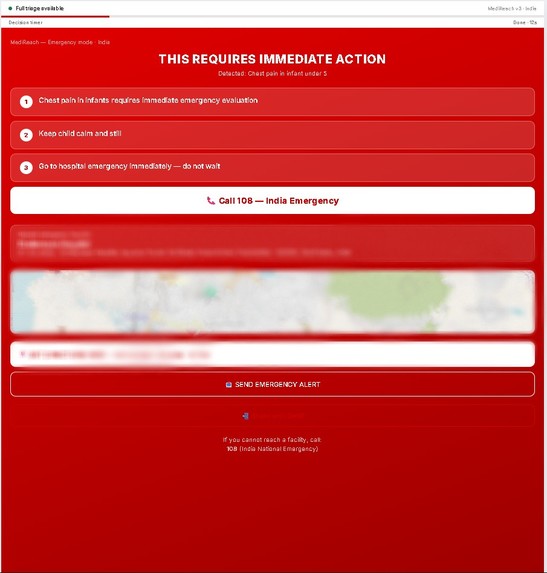
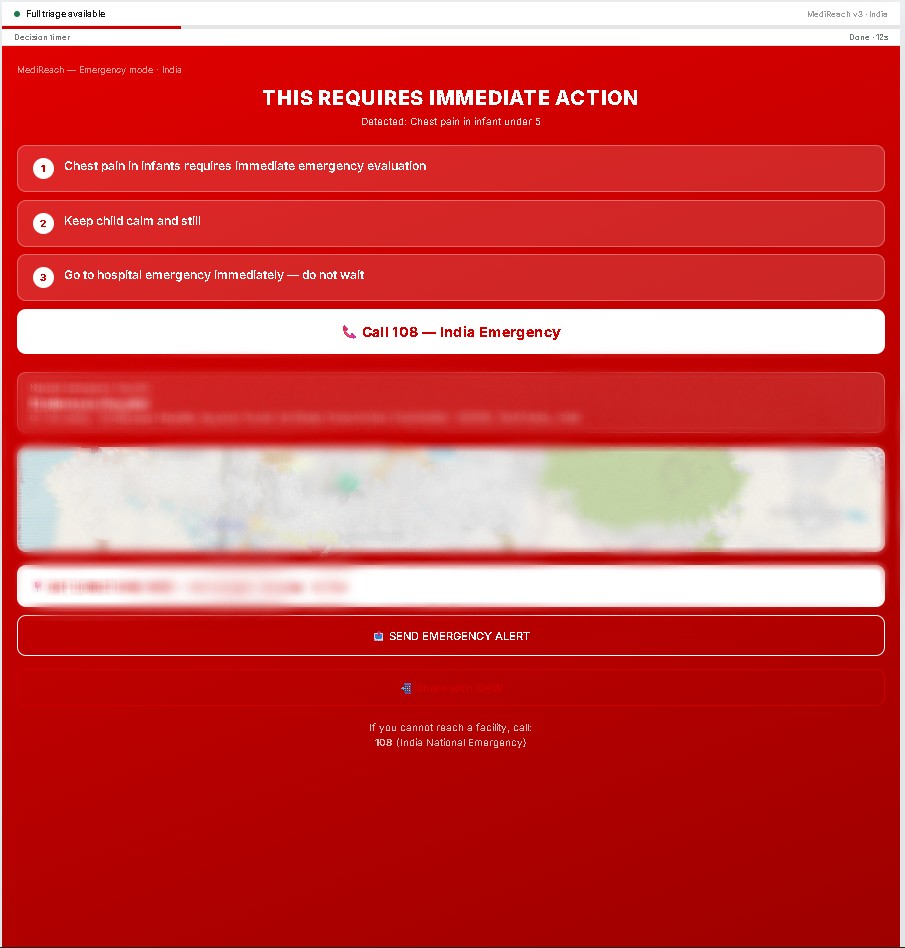
FINAL REPORT RED
-
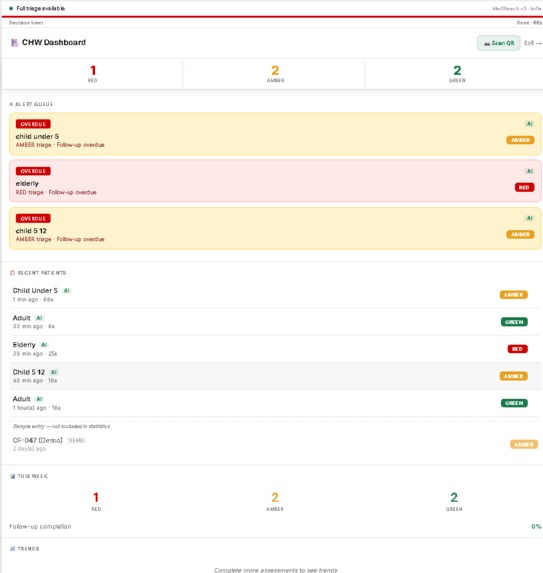
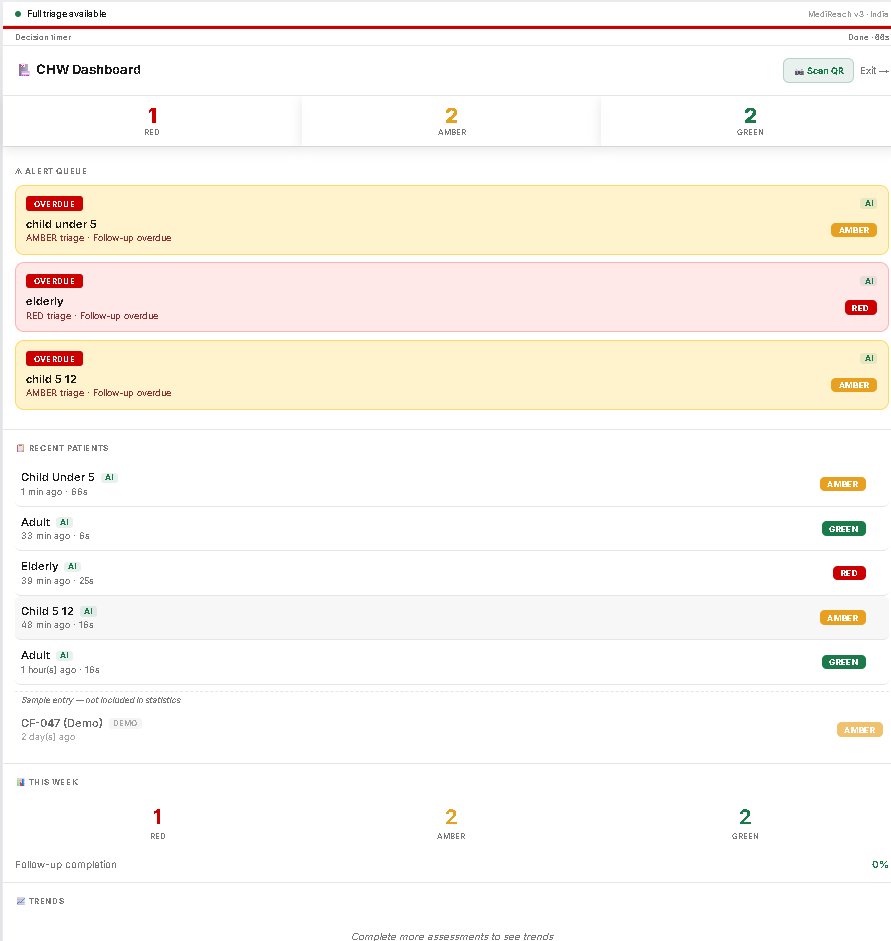
CHW DASHBOARD ABOVE
-
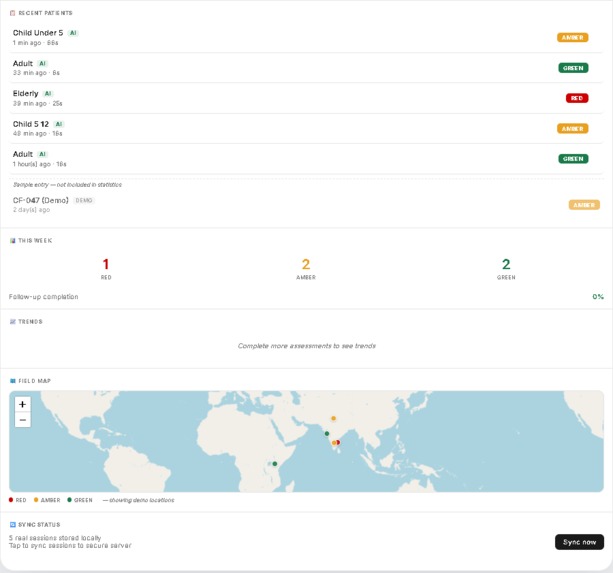
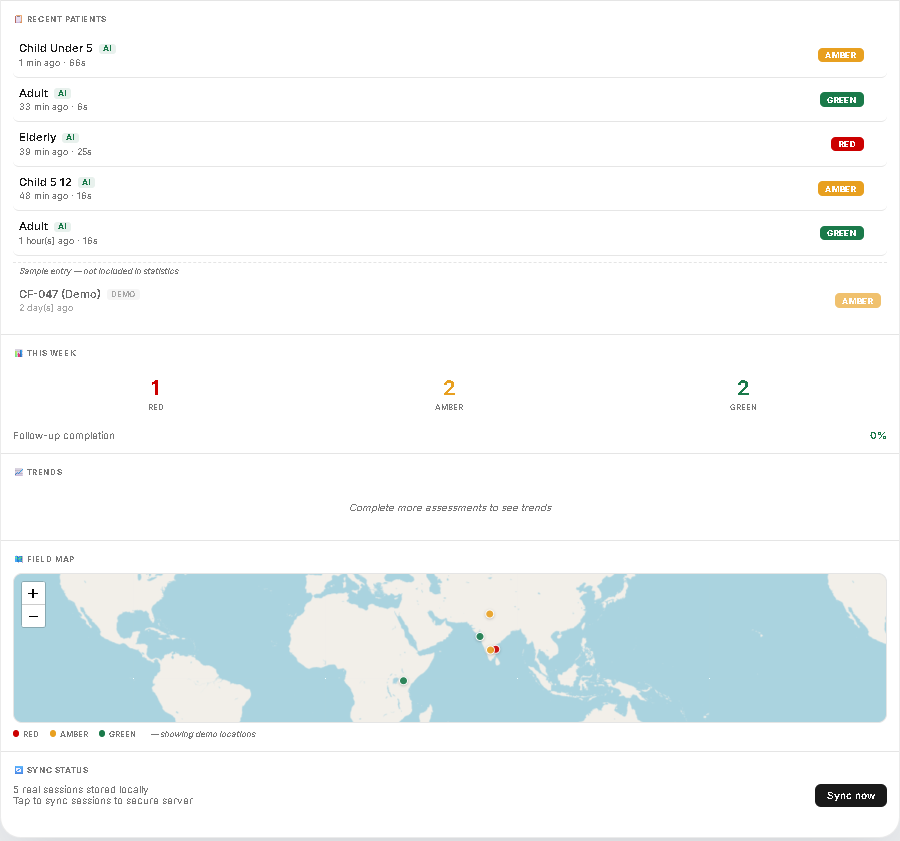
CHW DASHBOARD BELOW
-
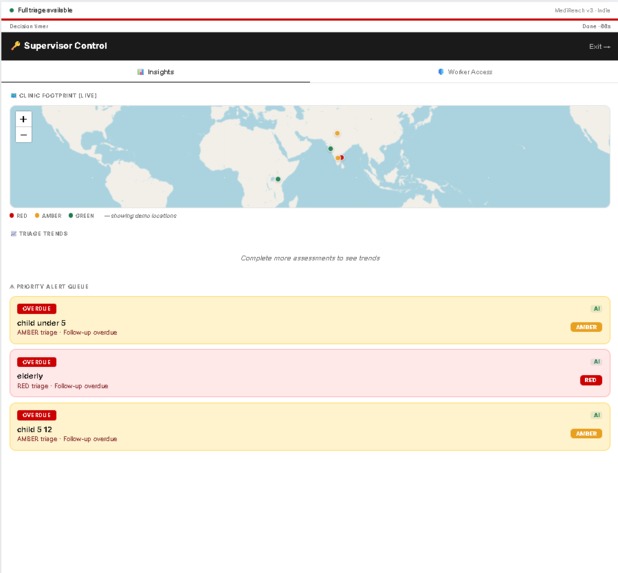
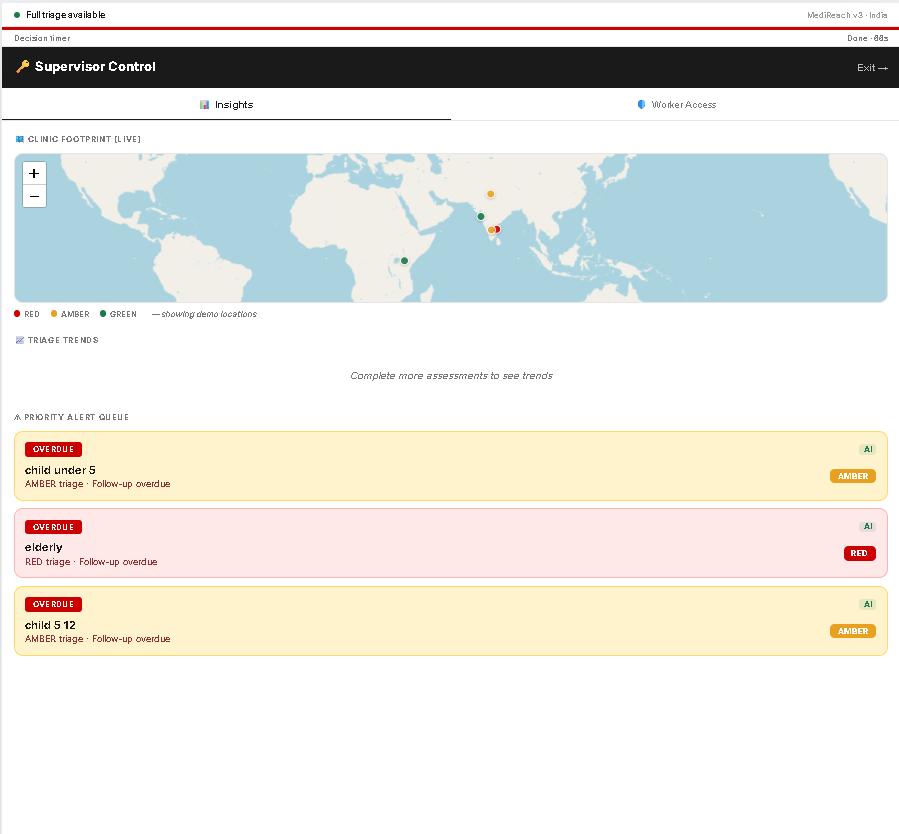
SUPERVISOR DASHBOARD
-
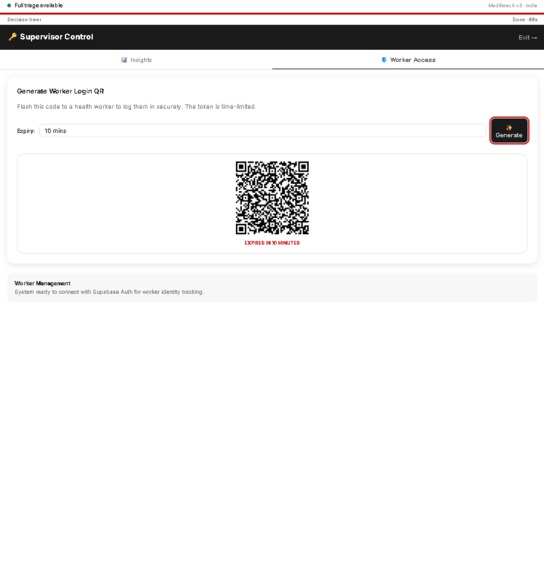
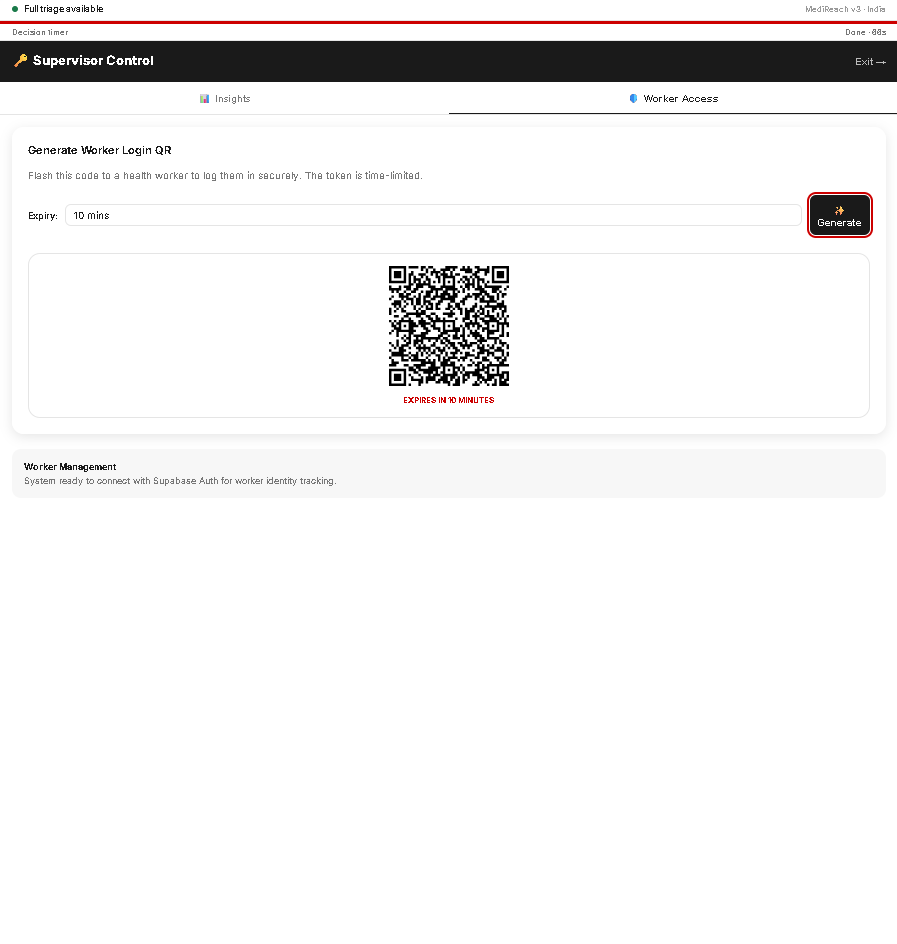
SUPERVISOR WORKER ACCESS
Inspiration
Every year, over 4.5 billion people lack access to essential health services (WHO, 2023). But in many low-resource settings, the primary failure is not infrastructure — it is delay in decision-making.
A Community Health Worker (CHW) often faces a critical question:
"Is this safe to manage at home, or is this an emergency?"
This hesitation — driven by uncertainty — leads to delayed care and preventable deaths.
We built MediReach v3 to eliminate this hesitation gap by giving frontline workers a fast, reliable, and explainable triage system that works anywhere, even offline.
What it does
MediReach v3 is an offline-first clinical triage system designed for Community Health Workers.
In under 60 seconds, it:
- Classifies patient condition into RED / AMBER / GREEN
- Calculates an urgency score (0–100)
- Provides plain-language care guidance
- Works offline on any smartphone
- Supports multilingual voice input (Tamil, Hindi, Swahili, English)
- Shows nearest clinics using GPS
- Feeds data into a real-time epidemiological heatmap
It does not replace doctors — it ensures patients reach them at the right time.
How we built it
We engineered a two-layer safety architecture:
1. Deterministic Clinical Engine
- Based on WHO IMCI protocols
- Runs fully on-device (IndexedDB + Service Worker)
- Executes in < 50 ms
- Produces severity + urgency score:
$$ U = U_{\text{base}}(S) + \Delta_{\text{duration}} + \Delta_{\text{category}} + \Delta_{\text{compound}} $$
This layer guarantees safety.
2. AI Enrichment Layer
- Uses Llama 3 70B via Groq
- Converts rule outputs into:
- Human-readable explanations
- Local-language instructions
- Family communication guidance
AI cannot override clinical severity.
Supporting Systems
- Offline-first storage: IndexedDB → Supabase sync → localStorage fallback
- Secure access: QR login + JWT (HttpOnly)
- Voice parser: multilingual symptom detection
- Responsive UI: mobile (CHW) + desktop (supervisor dashboard)
- Epi-Heatmap: real-time outbreak pattern detection
Challenges we ran into
1. Offline reliability vs real-time intelligence
Balancing a fully offline system with optional AI required strict separation between deterministic safety logic and AI enrichment.
2. Service Worker cache inconsistency
App updates caused stale UI crashes in offline mode.
We solved this using navigation fallback + cache revalidation strategy.
3. Multilingual voice ambiguity
Different languages describe symptoms differently.
We built a custom keyword-mapping parser instead of relying on generic speech models.
4. Security without friction
Traditional login systems fail in field environments.
We designed a QR-based access system that is both secure and fast.
Accomplishments that we're proud of
- Built a fully offline clinical triage engine
- Integrated WHO-aligned medical logic into code
- Achieved sub-60-second decision flow
- Developed multilingual voice triage
- Created a real-time epidemiological heatmap
- Designed a system that scales across countries without core changes
- Implemented automated testing for clinical rules
What we learned
- Safety > intelligence in healthcare systems
- AI is most powerful as a translator, not a decision-maker
- Offline-first design is not optional in global health — it is foundational
- Explainability increases trust and action
- Real-world constraints (language, connectivity, device limits) define success more than algorithms
What's next for MediReach
- Expand rule coverage beyond IMCI (maternal + chronic conditions)
- Integrate real-world pilot testing with CHWs
- Add predictive outbreak alerts using aggregated data
- Expand language support to more regions
- Partner with NGOs and public health systems
- Deploy at scale across India and other LMICs
“MediReach does not replace the doctor. It ensures the patient reaches one in time.”
Built With
- bcrypt
- express.js
- git
- github
- helmet.js
- indexeddb
- jwt
- leaflet.js
- node.js
- openstreetmap
- pwa
- react
- render
- supabase
- vannilacss
- webspeechapi


Log in or sign up for Devpost to join the conversation.