Inspiration
A fertility referral can be clinically justified and still fail operationally.
In fertility care, the breakdown rarely happens at the moment of decision. It happens in the silent space afterwards: the workup is incomplete, partner testing arrives weeks late, outside records sit unindexed in scanned PDFs, fertility preservation timing is measured in days, and nobody has translated the chart into a specialist-ready packet. The referral is medically appropriate, but operationally unready, and the patient absorbs the delay.
This is a large and time-sensitive problem.
- WHO estimates that 1 in 6 adults worldwide experience infertility during their lifetime.
- CDC reports that 13.4% of U.S. women ages 15 to 49 have impaired fecundity, and 8.5% of married women in that age range are infertile.
- ASRM highlights major access disparities and estimates that only 24% of U.S. ART need is currently met.
- NCI SEER estimates 88,120 new cancer cases among adolescents and young adults ages 15 to 39 in the United States in 2026, where gonadotoxic therapy can compromise future fertility within days of starting treatment.
The workflow failure is just as measurable as the clinical need.
- Specialists report receiving no prior information in 68% of outpatient referral visits.
- Only 34.8% of referral scheduling attempts result in a documented completed specialist appointment.
- Physicians spend 49.2% of office time on EHR and desk work, versus 27% in direct patient time.
The cost of that is concrete. Cycles of fertility lost to age. Fertility preservation windows missed before chemotherapy. Patients re-explaining their history at every visit. Specialists triaging from incomplete packets. Coordinators chasing labs that should already be in the chart. None of this is a knowledge problem. It is a coordination, timing, and handoff problem.
Fertility Referral Control Tower exists to close that gap.
How today's workflow really looks, and how ours changes it
Today, in most clinics:
- A clinician decides a patient needs fertility evaluation or fertility preservation.
- A nurse or coordinator manually scans years of notes, labs, imaging, and outside records.
- Partner information, if any, is incomplete or stored separately.
- The referral letter is short, generic, and frequently missing key fertility-relevant findings.
- The specialist receives the patient with little prior context and re-runs much of the workup.
- Fertility preservation cases compete in the same queue as routine evaluation, so urgency is not visible.
- Follow-up tasks (order missing labs, schedule imaging, request partner semen analysis) live in inboxes, sticky notes, and verbal handoffs.
- The patient gets a vague "we are referring you" message and often does not understand what comes next.
With Fertility Referral Control Tower:
- The MCP pulls fertility-relevant evidence from FHIR context and optional note text in seconds.
- Deterministic clinical rules classify the case as routine, expedited, or time-critical fertility preservation, with explicit reasons.
- Missing workup is surfaced as a structured gap matrix instead of buried in prose.
- A specialist-ready referral packet is generated with confirmed findings, urgency, outstanding workup, and rationale.
- A patient-friendly brief explains what is happening and why.
- Follow-up actions are prepared as a preview FHIR Bundle the clinician can inspect before anything is committed.
- "What is known" and "what is missing" are kept separate, so nothing is silently assumed.
The shift is not cosmetic. It changes who does the operational work, how visible it is, and how reviewable it is.
What it does
Fertility Referral Control Tower is a FHIR-aware MCP workflow for fertility referral readiness and fertility preservation coordination. It takes structured patient context plus optional clinical note text and converts them into an operationally useful next step for clinicians and coordinators.
Instead of behaving like a generic summarizer, it answers the questions that actually determine whether a referral can move forward:
- Is the patient ready for fertility referral now, or is the workup still incomplete?
- Is this an urgent fertility preservation case that should be expedited before gonadotoxic therapy?
- What evidence already supports the referral, and what is still missing?
- What should happen next, and is it safe to act on?
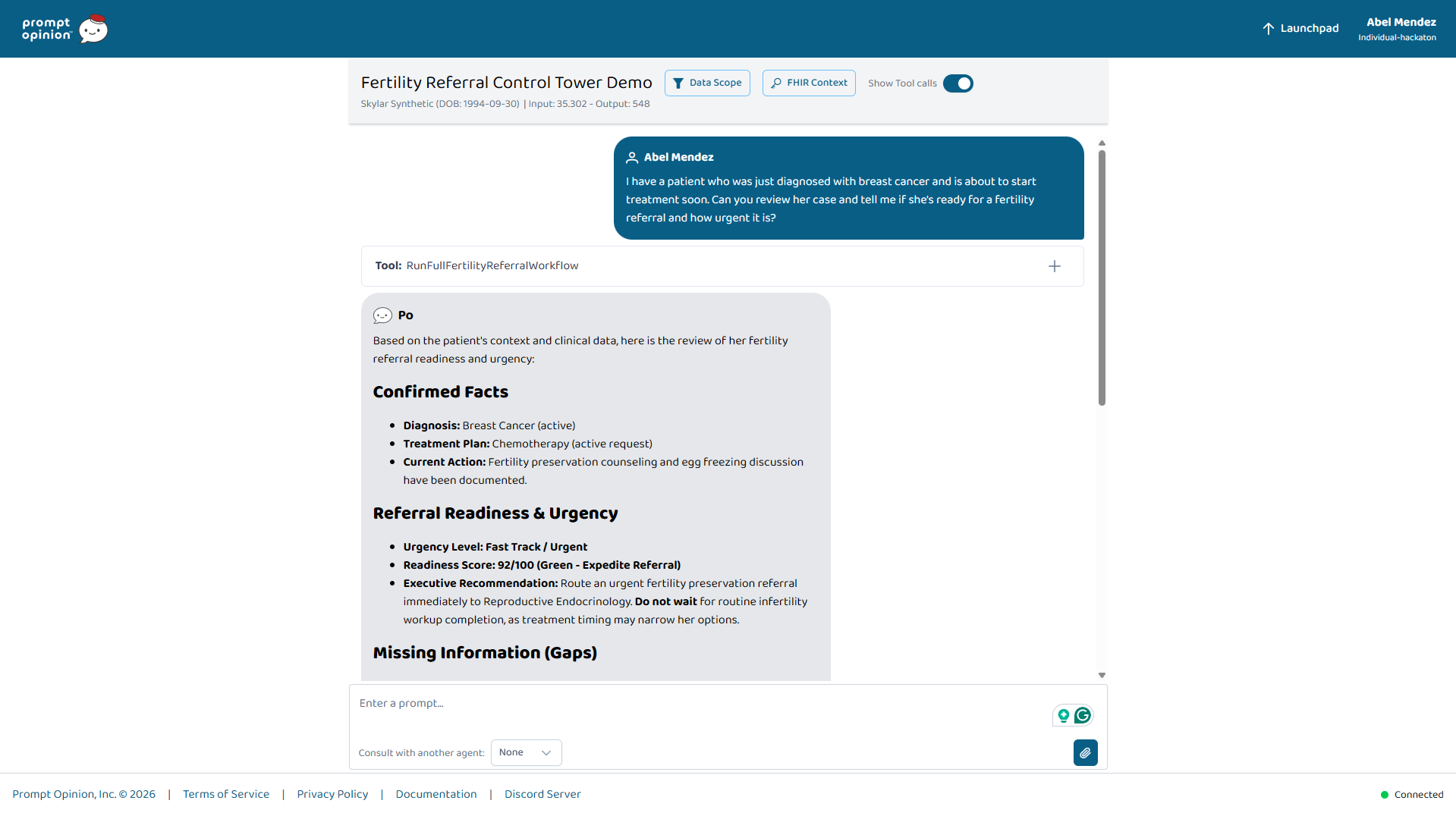
Every case ends in a structured, clinically legible view:
- Confirmed Facts
- Missing Information
- Referral Readiness and Urgency
- Recommended Next Step
- Previewed follow-up actions when appropriate
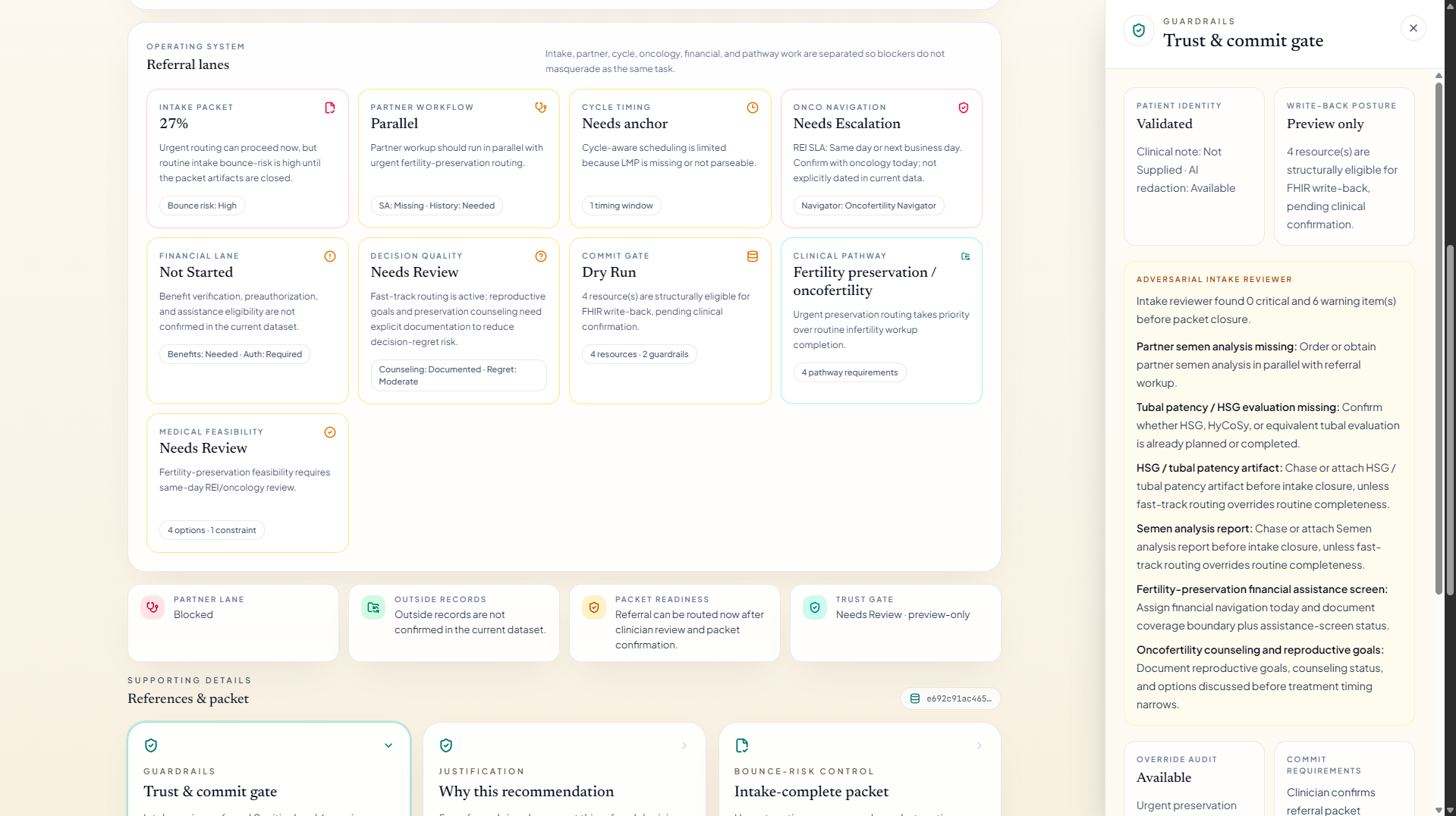
Clinical workflow and MCP tools
The MCP is a clinical workflow, not a single prompt. Each tool addresses a specific failure mode in fertility care.
Evidence and clinical baseline
GetFertilityEvidenceBundleconsolidates fertility-relevant context from the FHIR record and optional note text: reproductive and menstrual history, ovulatory and tubal factors, semen analysis when present, ovarian reserve indicators, prior workup, and oncologic context. Problem it solves: the fertility signal exists in the chart but is buried under unrelated encounters, so coordinators routinely miss it during manual review.
Readiness and urgency decisioning
EvaluateFertilityChecklistapplies deterministic referral rules to classify readiness and urgency. It distinguishes routine infertility evaluation (for example age plus duration of attempted conception per ASRM guidance), expedited evaluation for advanced maternal age or known reproductive risk, and time-critical fertility preservation before gonadotoxic therapy. Problem it solves: low-urgency and time-critical cases currently sit in the same queue. Here, urgency is explicit, justified, and visible.
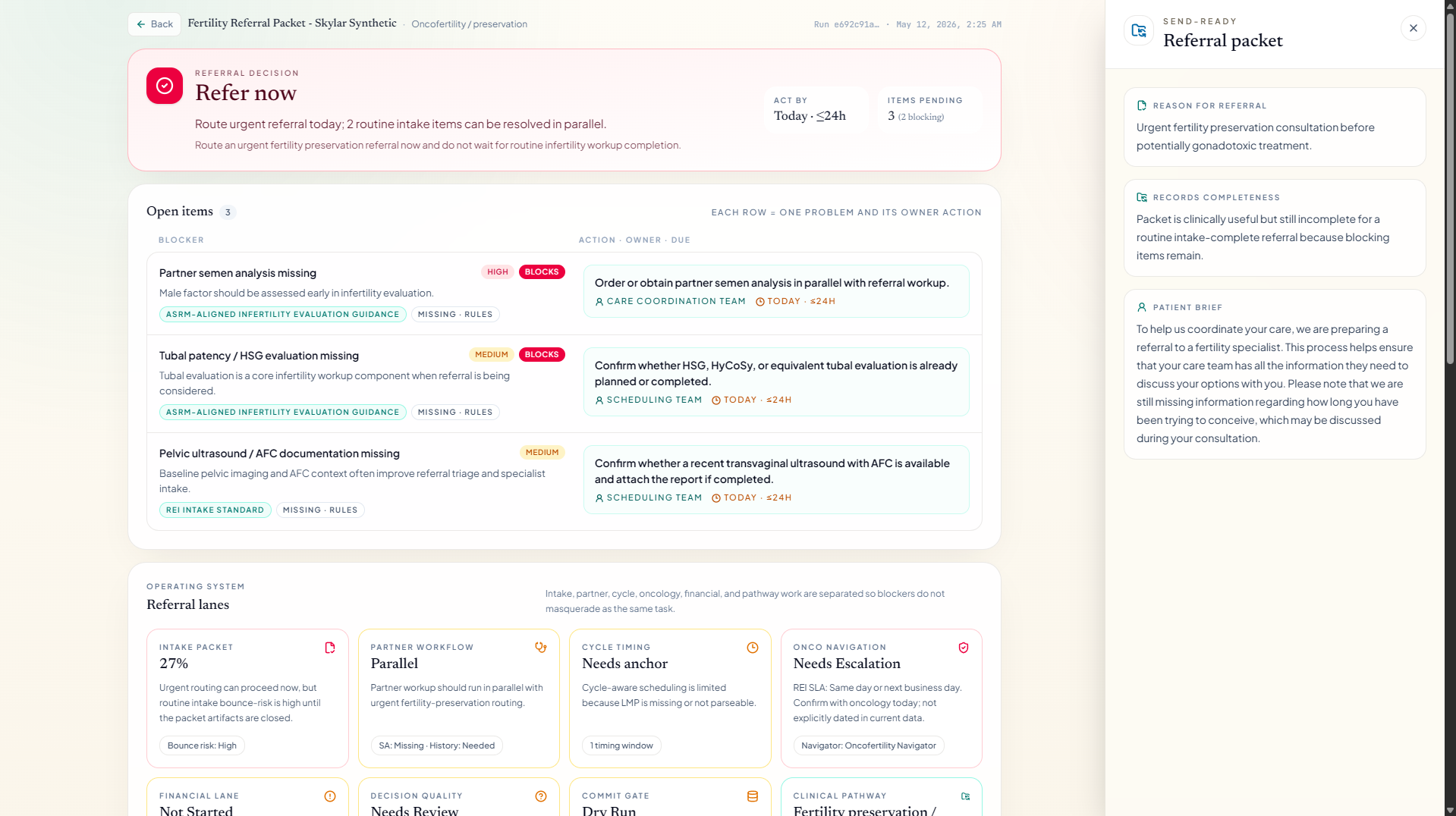
Operational gap detection
BuildGapMatrixturns the assessment into a concrete picture of what is still missing for a complete fertility workup, such as ovarian reserve testing, tubal patency assessment, partner semen analysis, hormonal evaluation, or imaging. Problem it solves: specialists routinely receive incomplete packets and bounce referrals; gaps are exposed before the referral is sent, not after.
Specialist-ready handoff
BuildReferralPacketDataassembles structured referral packet content for the receiving fertility specialist: reason for referral, urgency, confirmed findings, outstanding workup, relevant history, and rationale. Problem it solves: the "no prior information in 68% of visits" pattern. The specialist now starts from a real packet, not a one-liner.
Patient-side coordination
GeneratePatientEducationBriefproduces a brief, human-reviewable patient-facing explanation of the next fertility step and why it matters. Problem it solves: patients often leave the visit unclear about what was referred and what they have to do, which directly affects whether they complete the workup and attend the specialist visit.
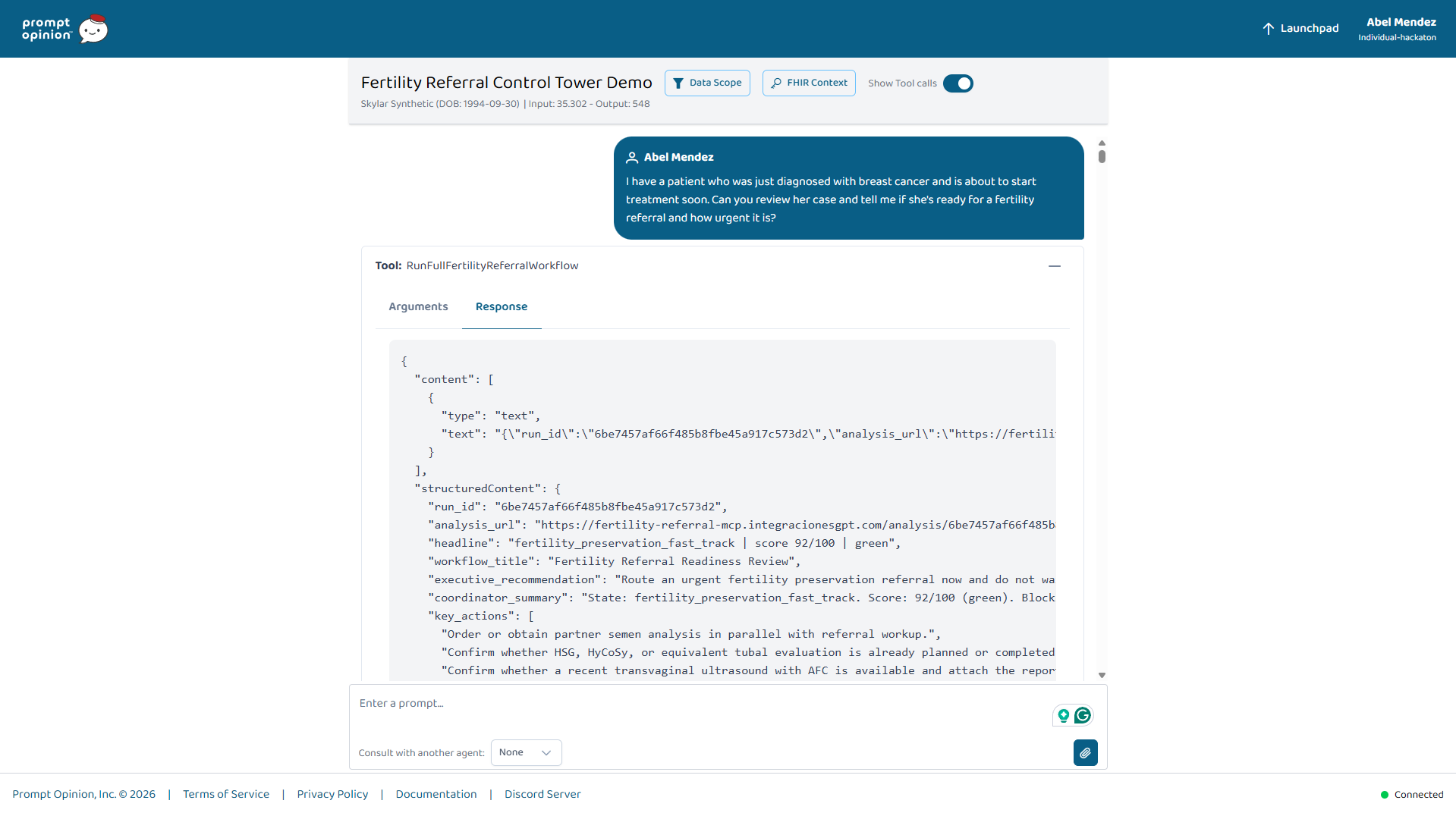
End-to-end orchestration
RunFullFertilityReferralWorkflowruns the full readiness pathway end-to-end and returns the assessment, packet, patient brief, and follow-up artifacts together. Problem it solves: value in fertility care comes from connecting the steps. This is the single entry point a clinician or another agent can call to get the full picture in one shot.
Safe follow-up and write-back
CreateFollowUpArtifactsPreviewproduces a preview FHIR Bundle with Tasks and a DocumentReference draft for follow-up actions, such as ordering missing workup, scheduling specialist evaluation, or initiating fertility preservation coordination. Problem it solves: follow-up tasks today live in inboxes and verbal handoffs; here they become explicit, reviewable artifacts before anything is committed.CommitFollowUpArtifactsToFhirperforms the actual write-back, but only when explicitly confirmed. It defaults to dry-run, requires clinician confirmation, and reports what succeeded and what was skipped. Problem it solves: preserves the safety boundary that fertility care, especially fertility preservation, requires, and matches how clinicians actually want to interact with automated follow-up.
Review surface and evaluation
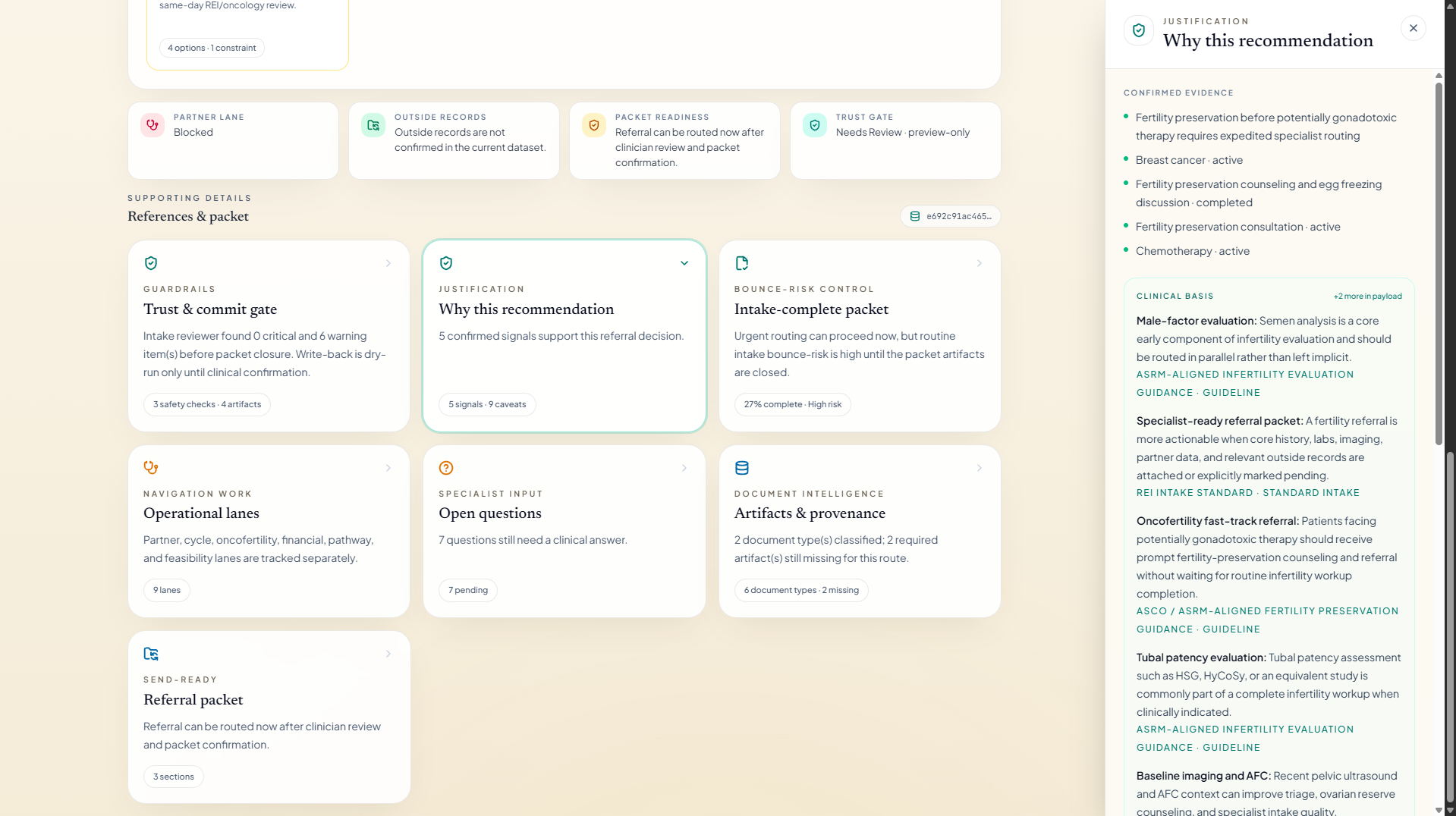
The MCP is paired with a dedicated review UI that renders the workflow output as a clinical operations picture instead of a raw JSON response. This is where the workflow becomes legible to the people who actually use it.
At a glance, the care team can see:
- the confirmed fertility evidence the workflow used, traced back to the underlying chart context
- readiness and urgency classification with the explicit reasons behind it
- the operational gap matrix of missing workup and documentation
- the proposed referral packet content for the specialist
- the patient-facing brief
- the previewed follow-up actions before any write-back
That makes the workflow auditable. A specialist, coordinator, or medical director can verify why the system classified a case as urgent fertility preservation, what evidence supported it, what is still missing, and what would happen if they approved the follow-up. It also makes the workflow evaluable: because each step is explicit and structured, it can be checked against expected clinical behavior on synthetic and deidentified fertility cases, rather than judged only on how the final narrative reads.
Why this changes the workflow
A clinically grounded summary alone does not fix fertility care. What changes the workflow is making the operational layer explicit:
- Visible urgency. Fertility preservation cases stop competing silently with routine evaluation.
- Visible gaps. Missing workup is structured and reviewable, so coordinators can act on it before the referral bounces.
- Visible handoff. The specialist receives a real packet, which shortens time to a productive first visit.
- Visible patient narrative. The patient receives a brief explanation that supports adherence and shared decision-making.
- Visible safety boundary. Follow-up actions are previewed first, confirmed second, and only then committed.
The net effect is that fertility referrals stop relying on heroic individual coordination and start behaving like a reviewable clinical workflow.
Challenges we ran into
The hardest challenge was being clinically useful without overclaiming. Fertility decisions are sensitive to missing context, partner data, oncologic timing, and patient preference, so the workflow had to clearly separate confirmed findings from missing information and avoid inventing labs, dates, or history.
A second challenge was reflecting how fertility referrals actually fail in practice: incomplete workups, late partner testing, fragmented outside records, and time pressure in fertility preservation before gonadotoxic therapy. Capturing those failure modes faithfully is harder than producing a polished narrative.
A third challenge was follow-up safety. Fertility care is time-sensitive, so follow-up actions stay in a preview-first posture, with explicit clinician confirmation before any write-back.
Accomplishments that we're proud of
We are proud that Fertility Referral Control Tower moves a case from "we should refer" to "the referral is actually ready," with explicit readiness, urgency, gaps, packet content, patient education, and previewed follow-up.
The output is clinically legible: a clinician or coordinator can quickly see what is confirmed, what is missing, how urgent the case is, and what the next step should be, instead of reconstructing that from a long narrative.
The workflow is also reusable. It is published as an interoperable clinical capability, so the workflow itself can travel into other fertility-aware care settings, not only the demo around it.
What we learned
Trust in clinical AI comes from structure, restraint, and legibility. A fertility workflow that explicitly shows what is known, what is missing, what is urgent, and what should happen next is far more useful than one that simply sounds confident.
Many high-value clinical AI problems live in the handoff layer. The opportunity in fertility care is not to replace specialist judgment. It is to reduce coordination failure, surface fertility preservation urgency early, and help teams close the referral loop faster and more safely.
Technical approach
The workflow is implemented as a Python MCP server with FHIR-aware context handling, deterministic referral logic, structured gap detection, packet generation, and preview-first follow-up actions. It is paired with a Next.js review surface that renders the output as an operational case view.
The core stack:
- Python for the MCP backend and workflow orchestration
- FHIR-aware context handling for structured fertility-relevant patient data
- Deterministic rules for readiness, urgency, and gap evaluation
- Selective generative AI for the patient-facing brief and clearer workflow packaging
- Next.js for the case review and analysis interface
The MCP is distributed as an interoperable clinical capability so the workflow can be evaluated and reused beyond a single demo.
What's next
We want to deepen the workflow in two clinical directions: broader fertility referral operations and stronger fertility preservation pathways, including tighter handling of oncologic timing.
We also want to measure concrete operational outcomes:
- fewer bounced or delayed fertility referrals
- shorter time to specialist-ready packet completion
- improved referral loop closure
- earlier identification of fertility preservation urgency
- less manual pre-referral chart review burden
On the technical side, the next step is to harden production deployment, expand safe follow-up support, and continue improving how interoperable tools and structured fertility context work together in a realistic clinical workflow.
Built With
- next.js
- python


Log in or sign up for Devpost to join the conversation.