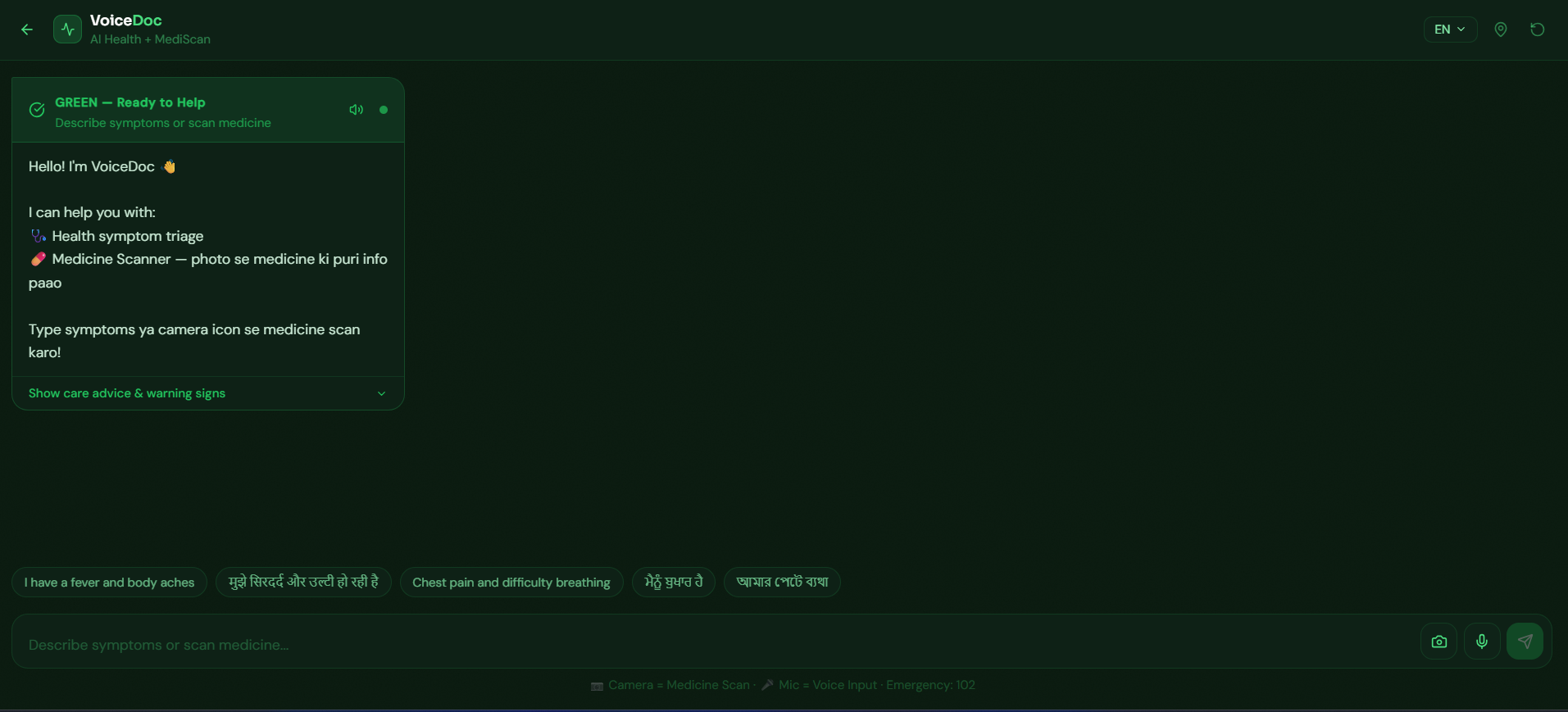
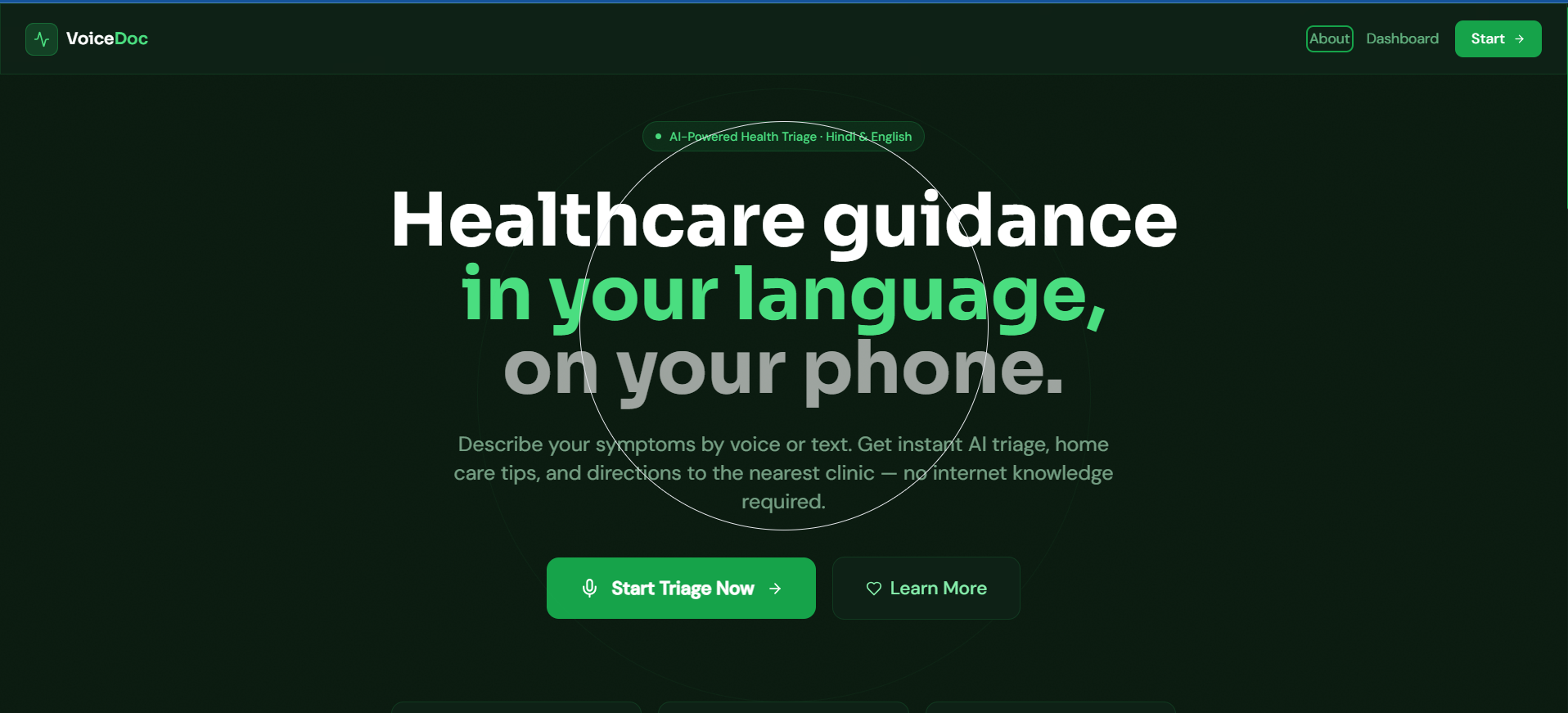
Inspiration Rural India faces a critical healthcare accessibility crisis—60% of the population lacks access to proper medical care. Doctor visits are expensive, travel is difficult, and language barriers compound the problem. We asked ourselves: What if we could make healthcare as simple as a WhatsApp call, powered by AI? That question led to VoiceDoc—a voice-based health assistant designed for those who need it most. What it does VoiceDoc is an AI-powered multilingual voice health triage system that:
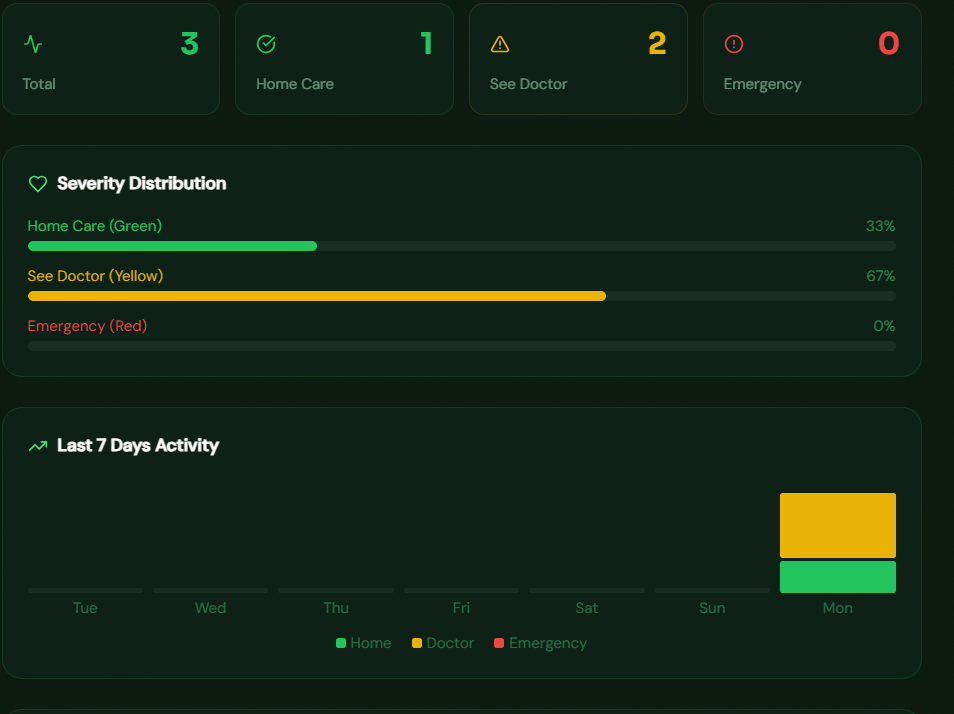
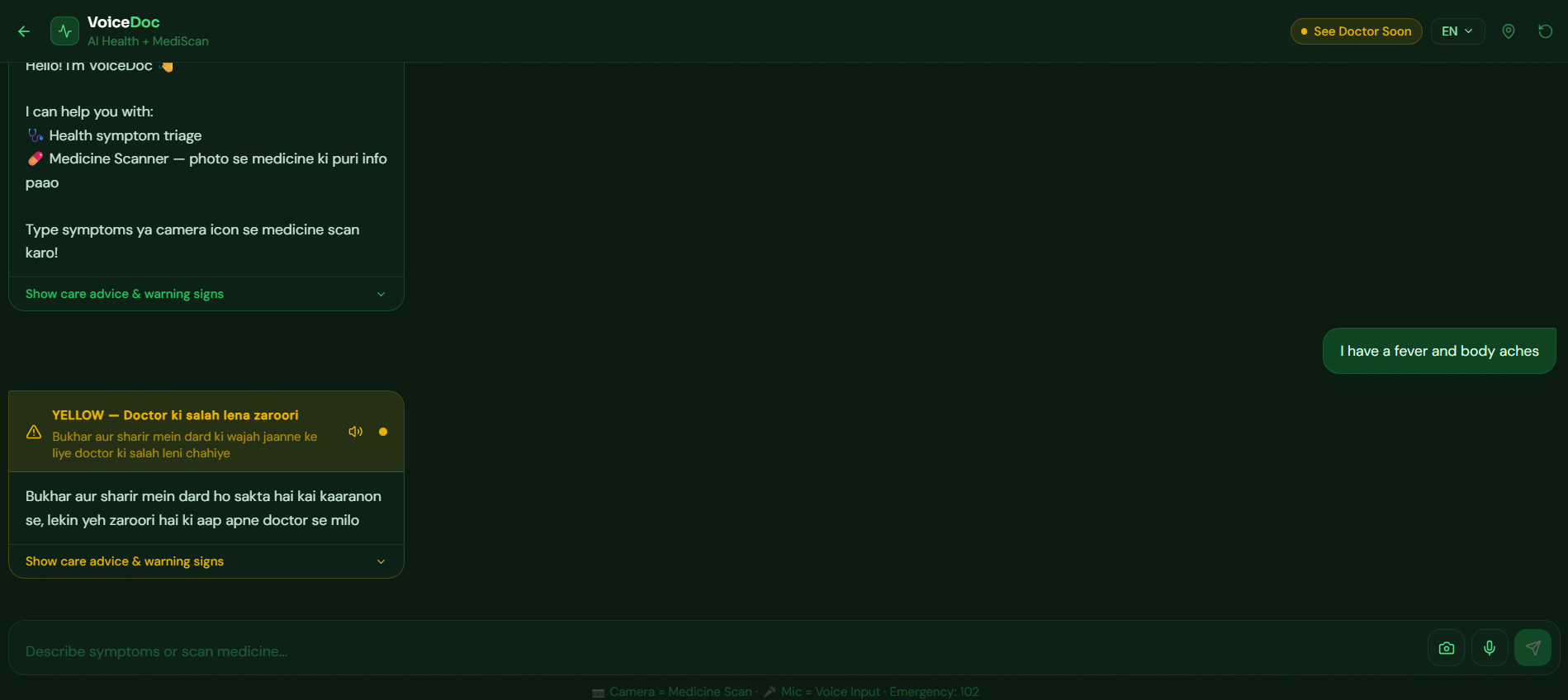
Listens to patient symptoms in Hindi or English via voice input Analyzes using cutting-edge LLaMA AI models (Groq-powered for speed) Diagnoses with preliminary health assessments and risk stratification Identifies medicines via visual AI (MediScan feature with text-to-speech) Alerts emergency cases with one-tap SOS functionality Tracks patient health history via an interactive analytics dashboard
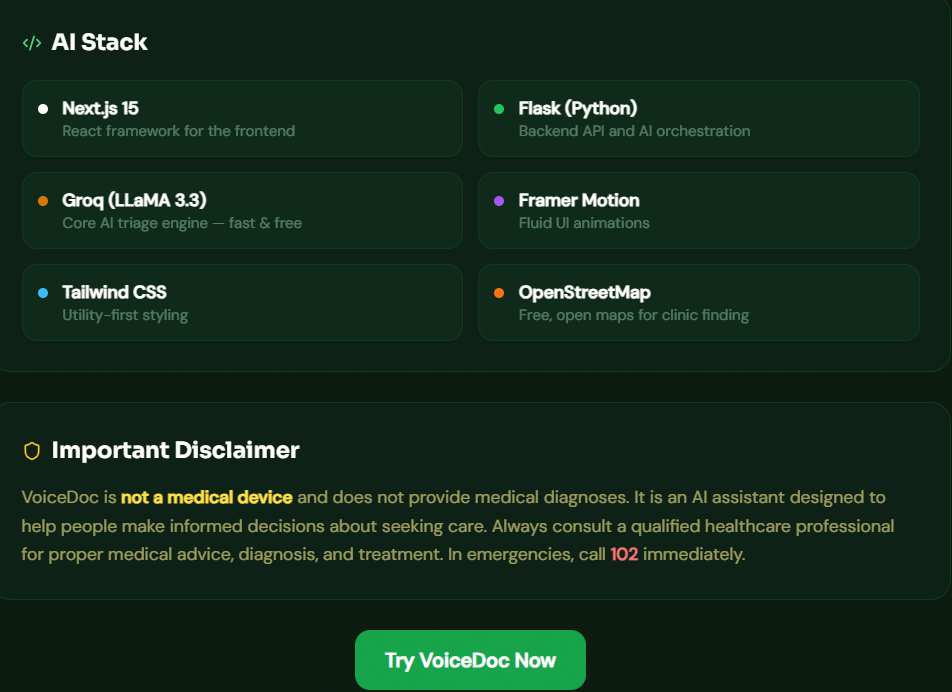
Essentially, VoiceDoc is a scalable, intelligent health companion for underserved populations. How we built it Production-Grade Tech Stack:
Frontend: Next.js 14 deployed on Vercel (responsive, optimized, fast) Backend: Flask deployed on Render (lightweight, scalable microservices) AI Engine: Groq API + LLaMA 2 (multilingual NLP, sub-second inference) Vision AI: Hugging Face models (medicine identification and verification) Database: MongoDB (secure patient data management) Architecture: Microservices optimized for low-bandwidth, rural connectivity
Key Technical Implementations:
Multilingual NLP pipeline with Hindi/English tokenization and code-mixing support Real-time voice processing using Web Speech API Text-to-speech accessibility in Hindi for non-literate users Inference optimization for edge devices and resource-constrained environments RESTful API with authentication and data validation Progressive loading and asset compression for slow networks
Challenges we ran into
Python 3.14 incompatibility — spaCy and sentence-transformers failed to install on modern Python versions. Solution: Downgraded to Python 3.11.9, replaced with lightweight scikit-learn alternatives and regex-based NLP. Render cold starts — Initial backend requests experienced 15+ second delays due to Render's free tier spin-down. Solution: Optimized Flask app startup, implemented health check endpoints, and added request caching. Environment variable management — Localhost URLs were hardcoded in .env.local, breaking production deployment on Vercel. Solution: Implemented environment-specific configuration via Vercel dashboard and dynamic URL generation. React-Leaflet dependency conflicts — Caused Vercel build failures and prevented deployment. Solution: Cleaned package-lock.json, removed unused dependencies, performed fresh npm installation. Multilingual voice processing latency — Voice input handling was too slow for real-time healthcare use. Solution: Implemented asynchronous processing, reduced model inference time, and added request queuing. Low-bandwidth optimization — Rural areas have 2G/3G connectivity; our initial build was too heavy. Solution: Implemented progressive loading, compressed assets (90% reduction), intelligent caching strategies, and API response optimization.
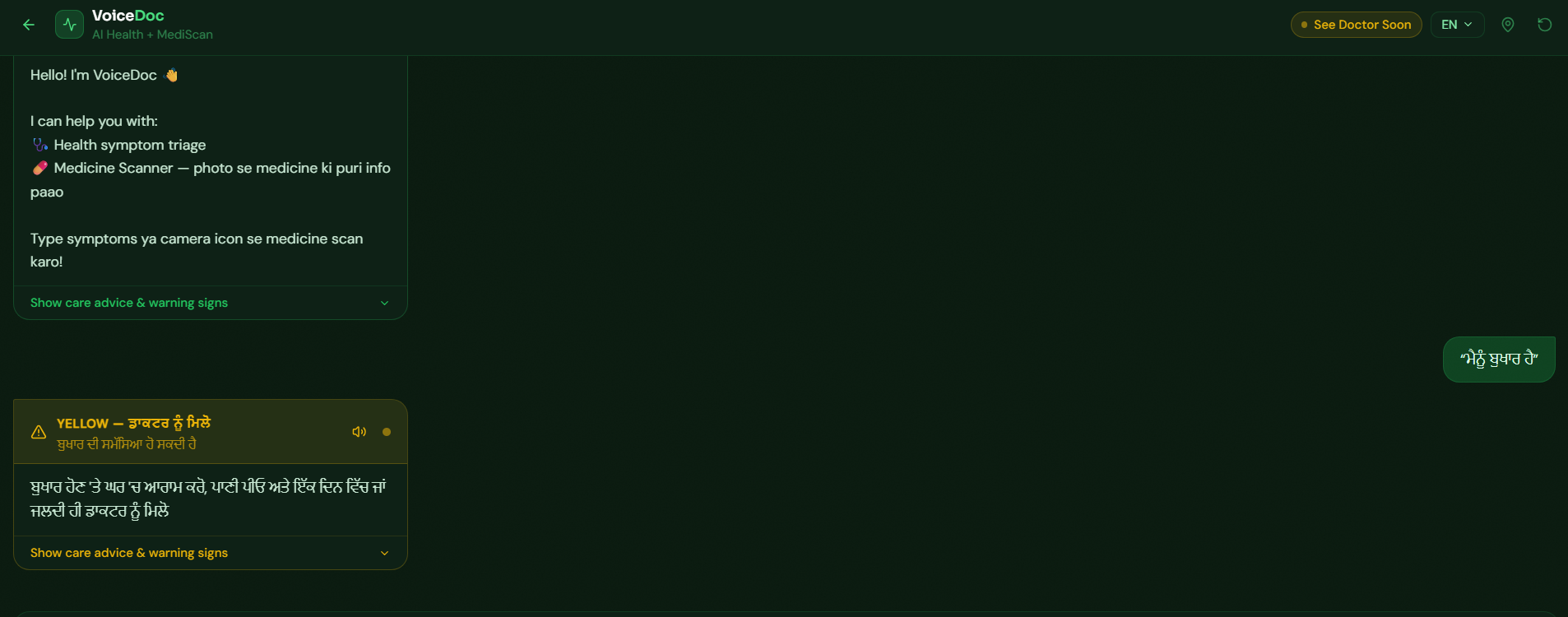
Accomplishments that we're proud of ✅ Fully deployed, production-ready system — Not a prototype; VoiceDoc is live, tested, and deployable ✅ Multilingual language support — Hindi and English with Hinglish code-mixing support for authentic rural communication ✅ Sub-3 second diagnosis delivery — Fast enough for real healthcare decision-making ✅ Medicine identification via vision AI — Unique feature enabling medication verification using phone camera ✅ Octoverse Hackathon submission — Already validated by GitHub and major open-source community ✅ Highly scalable architecture — Capable of handling thousands of concurrent users with minimal infrastructure costs ✅ Accessibility-first design — Voice input, TTS output, minimal UI complexity for non-digital-native users ✅ Cost-effective deployment — Zero external API costs; fully open-source tooling for rural scaling What we learned
Real-world constraints drive better design — Building for rural India forced us to optimize every aspect: bandwidth, latency, device compatibility, and user literacy levels became primary design constraints, not afterthoughts. Simplicity > Complexity — A voice interface beats elaborate dashboards for populations with varying digital literacy. UX must match user capability, not developer preference. MLOps is as important as ML — Model optimization, inference speed, cost management, and deployment pipelines consumed 80% of development time. Production readiness requires both software and infrastructure maturity. Multilingual AI is fundamentally harder — Language nuances, code-mixing (Hinglish), regional accents, and linguistic variation require specialized handling beyond standard NLP. One-size-fits-all models fail. Deployment complexity ≠ Development complexity — A simple Flask app can require extensive infrastructure work. Cloud platform quirks, dependency conflicts, and environment management are real challenges in production. In healthcare, user-centric design is life-critical — Every feature, every message, every delay has real consequences. We learned to prioritize accuracy, clarity, and fail-safes over feature richness.
What's next for VoiceDoc 🚀 Phase 2 (Next 6 months):
Regional language expansion — Add support for Tamil, Telugu, Bengali, Marathi, and Punjabi to reach 80% of Indian population Doctor network integration — Partner with verified medical professionals for complex case escalation and second opinions Offline-first capability — Enable core functionality without internet using cached AI models (critical for remote areas) NDHM integration — Connect to India's National Digital Health Mission for interoperability and official healthcare records Predictive analytics — Implement disease trend prediction at community level for public health insights SMS/IVR fallback — Support basic functionality via SMS and voice calls for feature phones (still majority of rural India)
🎯 Long-term Vision: Scale VoiceDoc beyond India to Southeast Asia and Africa. Make healthcare accessibility truly democratic—transforming healthcare from a privilege to a fundamental right. Our goal: be the first point of contact for populations currently underserved by traditional medical systems. Funding aspiration: Series A to build rural healthcare infrastructure Impact target: 1 million lives positively impacted by 2027 Success metric: Measurable improvement in early diagnosis rates and health outcomes in underserved communities

Log in or sign up for Devpost to join the conversation.