-
-

Log in page
-
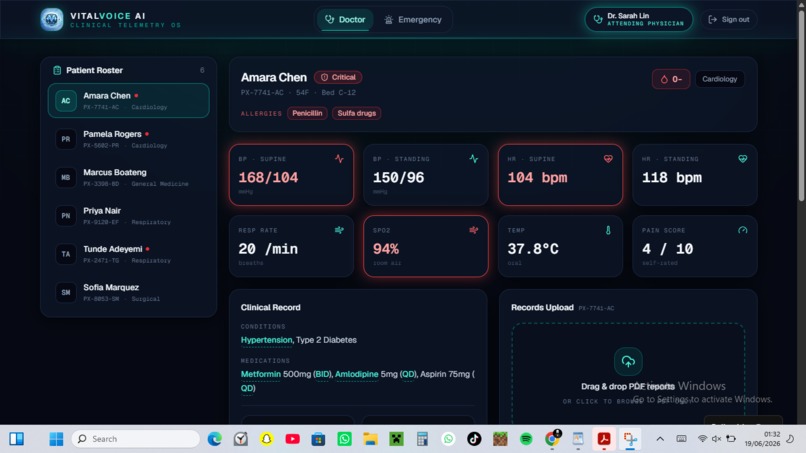
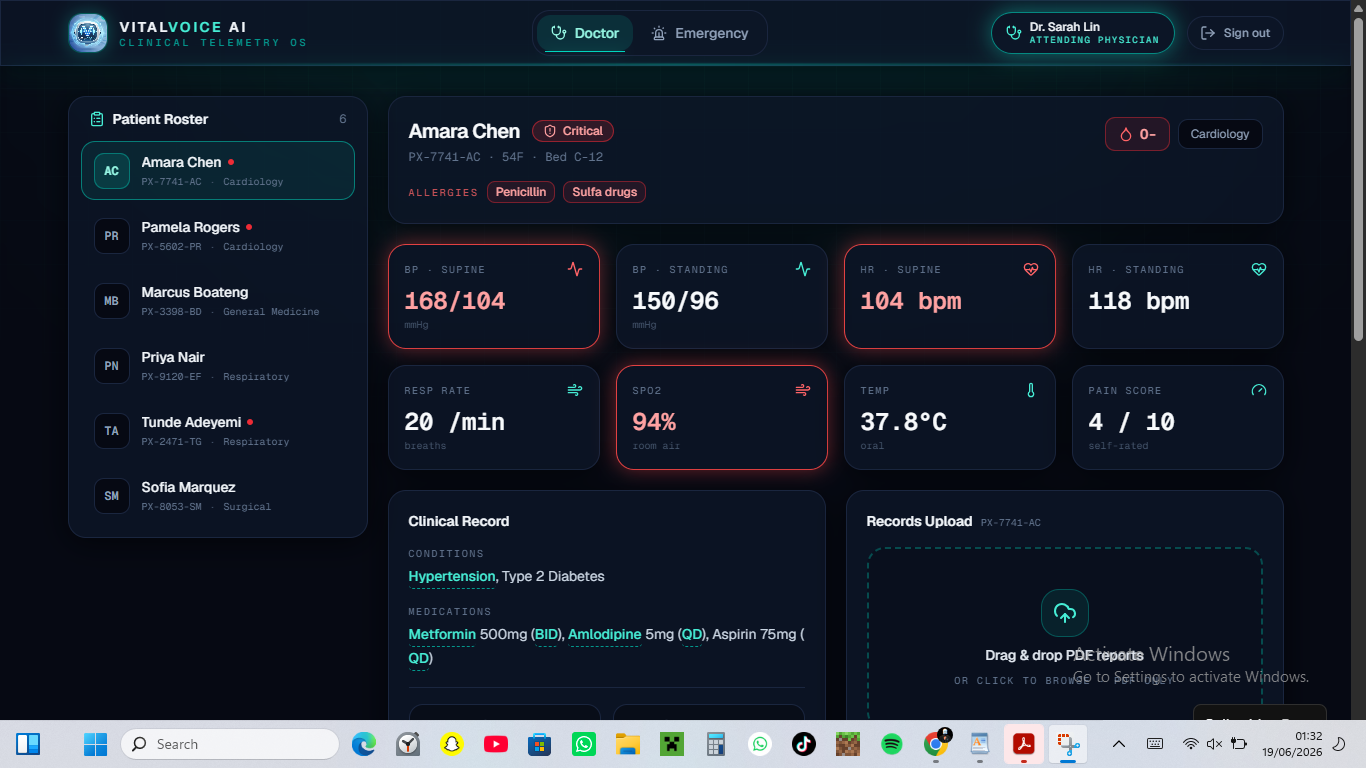
Doctor's portal
-
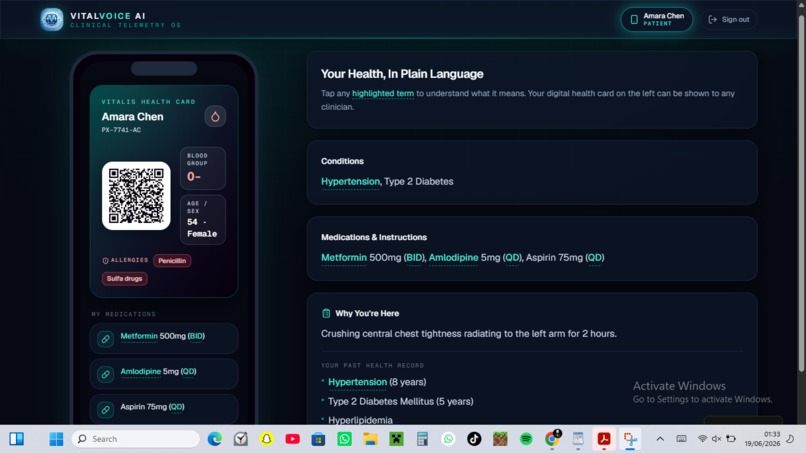
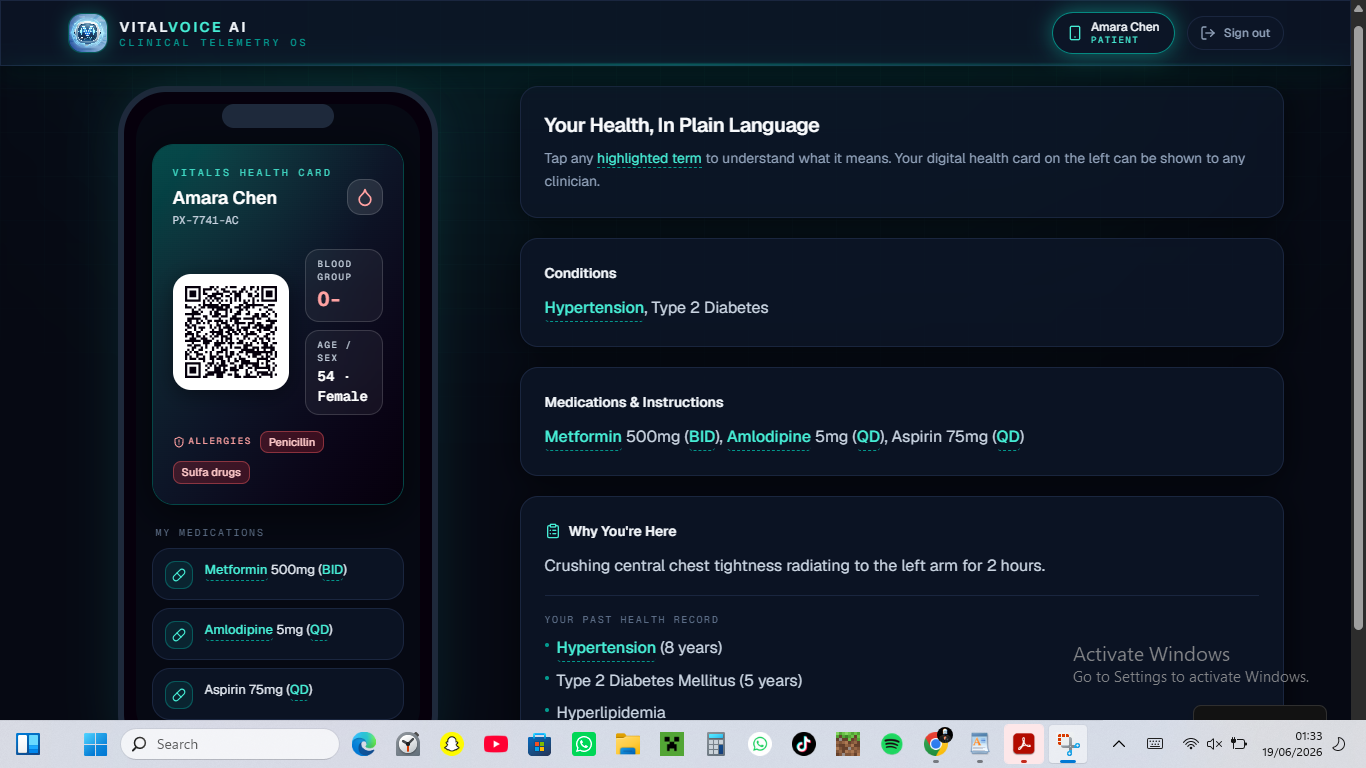
Patients mobile app
-
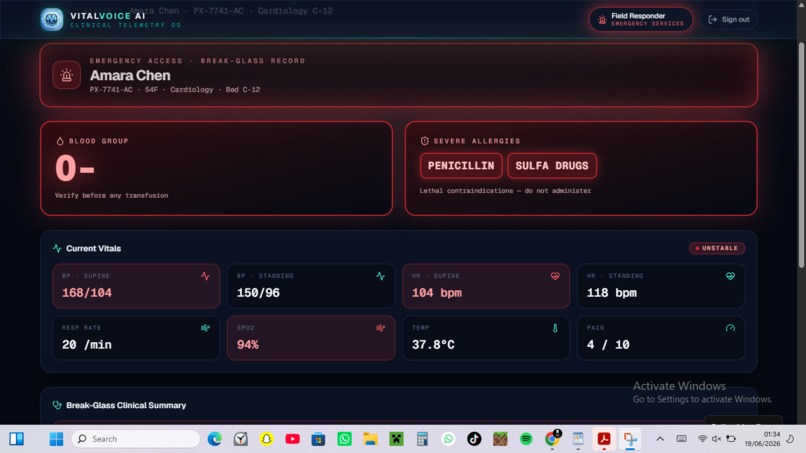
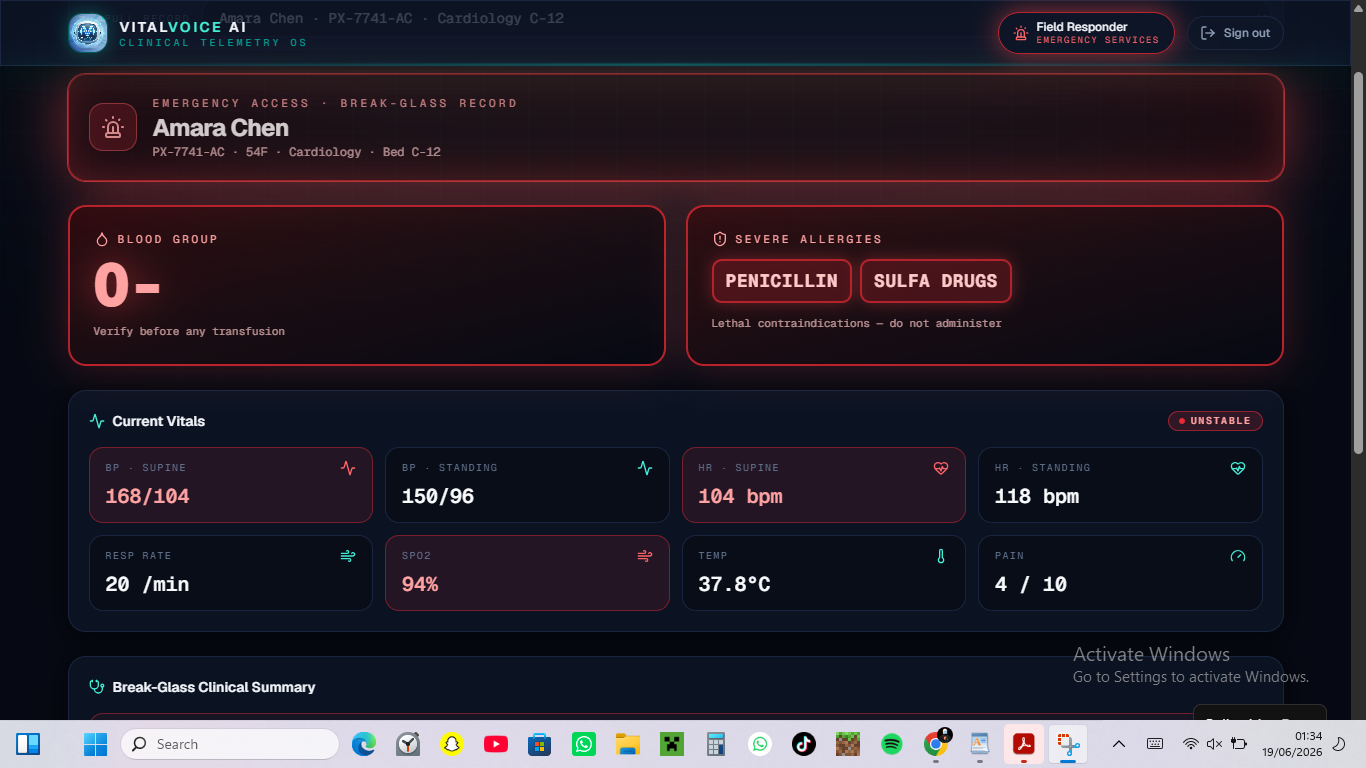
What emergency services will see if they scan the QR code

🚨 VITALVOICE: Redefining Clinical Data Highways in Emergency Care
💡 The Genesis & Inspiration (The "Why")
Every single day, emergency rooms and first responders are forced to make split-second, life-or-death choices completely blind. Consider a paramedic arriving at a chaotic trauma scene or treating an unresponsive individual collapsed on a public transit platform. The patient is entirely comatose—unable to vocalize their identity, let alone articulate that they suffer from unstable cardiovascular physiology, are bound to complex drug regimens, or harbor a lethal anaphylactic allergy to standard critical-care medications.
In an era where we automate complex global supply chains with zero-latency cloud infrastructure, a patient’s life-saving medical history remains locked inside fragmented, incompatible, and heavily gate-kept Electronic Health Record (EHR) databases. During the "Golden Hour"—the critical sixty-minute window post-trauma where morbidity and mortality curves are sharply decided—pre-hospital clinicians waste precious minutes conducting manual wallet searches, attempting to unlock biometric smartphones, or waiting on delayed hospital registration desks to patch through an archived profile.
This profound systemic vulnerability is what inspired VitalVoice. We recognized that a patient's medical identity should never be a passive, unreadable variable—it needs an immediate, definitive voice when they are physically incapacitated. We set out to engineer a continuous, zero-friction clinical data highway that bridges the dangerous information asymmetry between field emergencies, frontline nursing shifts, and institutional physician workflows. VitalVoice ensures that vital patient telemetry is decentralized, immediately deployable, and universally readable within two seconds of a crisis.
🌊 Systemic Depth: The Clinical and Psychological Weight of the Problem
To understand why VitalVoice is revolutionary, one must look beyond simple "user interface friction" and examine the severe clinical penalties, cognitive overloads, and psychological stress points that plague modern medicine. Healthcare environments are high-stakes pressure cookers; bad software architecture doesn't just cause operational delays—it actively breeds sentinel events and clinical burnout.
1. Eliminating the Pre-Hospital "Blind Spot" (First Responders)
- The Clinical Emergency Context: Paramedics operating in the field face profound psychological terror when administering emergency interventions without a diagnostic baseline. Administering a standard paralytic or antibiotic to an unconscious patient with an unknown anaphylactic history or a severe drug-to-drug cross-reaction can trigger immediate, catastrophic physiological collapse.
- The Structural Failure: Current systems rely on the patient being conscious, or carrying physical medical alert jewelry which is easily overlooked or lost in high-impact trauma.
- The VitalVoice Solution: The Emergency Triage Interface acts as a definitive visual shield. By executing aggressive content filtering, it suppresses 95% of non-essential administrative data (billing codes, provider phone numbers, registration dates) and pushes the absolute core physiological constraints—Blood Group and Severe Allergies—into massive, heavy typography at the absolute apex of the viewport. A first responder can scan a patient's locked-screen QR vector or physical proximity token and isolate lethal contraindications from several feet away in a dark, unstable environment. No credentials required, no firewall authentication latencies, no hesitation.
2. Mitigating the "Cognitive Switching Penalty" (Frontline Physicians)
- The Clinical Emergency Context: Modern physicians do not suffer from a lack of data; they suffer from an unorganized avalanche of it. When inheriting a critical patient, a doctor is forced to piece together unstructured text from external laboratory sheets, dense legacy PDFs, and cryptic handwritten charts. Forcing a human brain to manually scan, synthesize, and contextualize hundreds of rows of unformatted history while a patient's hemodynamic state actively fluctuates creates immense cognitive fatigue.
- The Structural Failure: Traditional medical software presents data in dense, spreadsheet-style configurations. Furthermore, the persistent use of Latin medical shorthand (abbreviations like BID, PO, QD, PRN) across different teams introduces massive communication vulnerabilities during handoffs.
- The VitalVoice Solution: The Physician Suite introduces an intelligent local ingestion matrix and a dedicated shorthand compiling engine. By integrating a simulated document-parsing drop zone, unstructured clinical paperwork is instantly processed, extracting key diagnostic profiles directly into the active state. Concurrently, the built-in Clinical Translator allows a physician to drop raw shorthand lines into the system and instantly generates a highly clean, structured plain-English treatment roadmap. This completely eradicates manual transcription stress and drastically reduces the doctor's semantic processing time, allowing them to focus entirely on advanced clinical reasoning.
3. Arresting "Silent Deterioration" (Ward Nursing Ecosystem)
- The Clinical Emergency Context: Ward rounds are a relentless, high-velocity race against the clock. A single nurse is frequently tasked with monitoring dozens of acute care beds across a 12-hour shift. As vital signs are manually checked and logged, numbers inevitably begin to blur. The primary driver of unexpected cardio-respiratory failure in hospital wards is "silent deterioration"—subtle, compounding changes across multiple vital signs (a creeping systolic pressure coupled with a marginal drop in oxygen saturation) that go completely unnoticed until the patient experiences a sudden, catastrophic code blue.
- The Structural Failure: Traditional charting systems display vitals as isolated historic columns. If a number is slightly elevated, it is viewed as an isolated variance rather than a compounding systemic risk factor.
- The VitalVoice Solution: The Ward Nurse Portal fundamentally updates the rounding paradigm by organizing the patient directory into a dynamic, interactive telemetry grid. Patient profiles are maintained as modular telemetry nodes. The moment a nurse logs a fresh set of metrics, the client-side state machine computes the collective deviation from a healthy baseline. If an overshoot is detected, the card component style reacts instantly, triggering a pulsing visual warning contour around that specific patient. This allows frontline nurses to visually prioritize high-risk rooms blocks ahead of schedule, capturing physiological decay long before a crisis peaks.
4. Resolving Post-Discharge Medical Alienation (Patients & Families)
- The Clinical Emergency Context: The transition from hospital discharge to home care is a period of intense vulnerability and psychological anxiety. Patients are handed complex care plans filled with confusing clinical terms and precise medication schedules. When a patient or an elderly family member feels unqualified to decode their own prescription, they experience severe post-discharge stress, which directly leads to medication non-compliance and preventable ER readmissions.
- The Structural Failure: Healthcare systems treat patient-facing portals as a secondary afterthought, offering rigid, unreadable summaries that do nothing to demystify complex clinical language.
- The VitalVoice Solution: The Patient Health Vault packs a premium health infrastructure right into a responsive personal mobile smartphone wallet pass, engineered inside a realistic device mockup bezel. It introduces a deeply empathetic Medical Jargon Decoder Engine. The application dynamically parses the patient's personal history and medication blocks, mapping an internal dictionary against the text. If a patient encounters a intimidating term like Hypertension or a shorthand interval like Metformin 500mg PO BID PC, they simply tap the highlighted node. The interface immediately renders a clear, conversational, plain-English breakdown explaining exactly what that means for their body. It replaces post-clinical alienation with absolute understanding, control, and peace of mind.
🛠️ Deep-Dive Product Architecture: What It Does
To comprehensively demonstrate this unified, multi-role data highway, VitalVoice integrates five independent, highly specialized viewports driven by a centralized frontend memory web:
- View 1: The Access Gateway: A beautifully minimal, dark-glass authentication core. To facilitate completely frictionless hackathon and investor evaluation, it features horizontal "Sandbox Nodes" for Doctor, Nurse, and Patient roles, executing single-click bypass routing that completely eliminates login fatigue for judges.
- View 2: The Physician Suite: Implements a responsive, multi-column patient directory with a real-time search index. Selecting a patient unlocks a deep-profile dashboard broken into highly detailed tab components: an Overview pane for chronic diagnostics, the active Ingestion Core with built-in PDF loading state animations, and the interactive Shorthand Compiler.
- View 3: The Ward Nurse Portal: Features a clean, high-speed monitoring panel visualizing active biometric parameters across the entire active registry. Selecting a node triggers an optimized, gesture-friendly vital signs input form allowing instantaneous logging of updated metrics.
- View 4: The Patient Mobile Vault: Explicitly rendered inside an ultra-polished smartphone frame with clean bezel tracking. It presents personal care timelines and medication matrices alongside a beautifully styled digital health card pass. This card pass houses an active, vector-drawn QR code block that serves as the secure vector directly into the emergency interface.
- View 5: The Public Emergency View: An unauthenticated, read-only field triage interface optimized explicitly for mobile extraction by public responders. Pinned to the top is an intense, flashing crimson warning banner. The screen drops all administrative noise to isolate the primary triage blocks, finishing with locked, tap-to-call communication anchors for the primary care doctor and next-of-kin at the absolute base of the layout.
🏗️ Engineering & Implementation Framework
VitalVoice was engineered as a self-contained single-file React web application optimized for zero-latency, client-side simulation.
- The Frontend Stack: Developed using functional React hooks (
useState,useEffect,useRef,useCallback) to create an unbroken data-binding loop. When a nurse modifies a vital sign or a doctor updates a medication array, that mutation instantly bubbles up, recalculating metrics across all views simultaneously. - The Visual Design System: Designed around a strict "cyberpunk luxury" and professional clinical design language. We explicitly bypassed standard, muted browser colors to enforce a highly premium color token canvas: an ultra-deep space canvas (
#060913), elevated frosted glass component cards (#0d1527/80with a sharp#1a263ftechnical border), and radiant telemetry cyan accents (#14b8a6). - Typography Treatment: To prevent visual cognitive fatigue under intense pressure, all standard interface controls, operational descriptions, and navigation links use a clean, professional sans-serif typeface, while all raw physiological measurements, numeric values, blood pressures, and unique patient tracking numbers are forced to render in highly legible monospace paths.
- State Persistence: Data structures are synchronized dynamically with browser
localStoragehooks, ensuring complete persistence across role swaps without requiring heavy server infrastructure or introducing network latency during live demonstrations.
📊 Mathematical Modeling of Physiological Volatility
To validate the platform's ability to act as an early-warning telemetry system rather than a passive ledger, the nurse rounding portal implements automated risk scoring metrics based on compounded physiological variances. Rather than treating heart rate, blood pressure, and oxygen saturation as isolated data silos, VitalVoice acknowledges that these vectors interact dynamically.
To mathematically model the compounding probability of an imminent clinical triage event $P(T)$ during a shift, we evaluate the vital overshoot threshold index ($\lambda$) across active intervals ($t$) through a non-linear decay function:
$$P(T) = 1 - e^{-\lambda t}$$
Where the clinical volatility index $\lambda$ is automatically compounded based on critical deviations within our application state parameters:
$$\lambda = \alpha \cdot \text{Variance}(\text{Systolic BP}) + \beta \cdot \left(100\% - \text{SpO2}\right)$$
In our client-side runtime logic, whenever a nurse inputs an abnormal blood pressure (e.g., a systolic reading $\ge 140\text{ mmHg}$) or an oxygen overshoot (e.g., SpO2 $\le 95\%$), the application instantly catches the tracking index $\lambda$. This shifts the component styling states reactively, triggering intense, pulsing color alerts around the patient's modular card to visually sound the alarm before a physiological crisis peaks.
🚧 Challenges we ran into
- Practicing Design Restraint in Crisis UI: The single hardest architectural challenge was enforcing extreme data suppression on the emergency viewport. As software engineers, our baseline instinct is to maximize data density—adding historical timelines, trend charts, and deep administrative logs. However, in a chaotic emergency environment, high density is an operational liability. We had to write strict, conditional filtering layout templates that completely strip away secondary information from the top half of the interface, ensuring that a paramedic's eyes are locked purely on allergies and blood groups within the first 500 milliseconds of a page load.
- Simulating Multi-Role Environments Client-Side: Building a prototype that flows seamlessly between four distinct real-world applications (a doctor’s desktop, a nurse’s tablet, a patient’s mobile wallet, and a first responder’s phone) usually requires a massive backend, complex session routing, and authentication handshakes. Introducing that overhead into a hackathon environment would create loading screens that ruin the pacing of a pitch video. We overcame this by writing a custom client-side state manager backed by a fixed horizontal navigation console, allowing a judge to instantly teleport between user roles without breaking state synchronization.
- Balancing Premium Aesthetics with High-Contrast Accessibility: Creating a dashboard that looks incredibly sleek and modern to venture capital investors while maintaining the rigid, extreme accessibility required for a medical environment was an intensive balancing act. We ran multiple style audits on our glassmorphism backdrop opacity values and technical border treatments to ensure that text lines remain blindingly sharp against our ultra-deep space background tokens.
🏆 Accomplishments that we're proud of
- The On-Demand Jargon Decoupling Engine: We engineered an interactive string parser that scans unstructured patient history blocks, programmatically flags matching keywords from an internal medical lexicon dictionary, and wraps them in custom interactive UI nodes. It successfully proves how deep technological empathy can be written directly into a codebase, transforming scary, gate-kept healthcare documentation into intuitive maps for everyday people.
- The Single-File Micro-Architecture: We succeeded in packing a comprehensive multi-role enterprise SaaS product blueprint—complete with localized databases, validation checks, upload animations, and complex device mockup frames—into a single, highly optimized React asset ready for instant production deployment.
- Frictionless Pitch Optimization: Building the top "Deployment Console" HUD ensures that anyone interacting with our live prototype can evaluate our core narrative and appreciate the full inter-connected value of the data highway with absolutely zero operational friction.
🧠 What we learned
This project completely upended our assumptions regarding healthcare product development and user experience design. We discovered that clinical interfaces do not have to look ancient or uninspired to be functional; in fact, an intentionally engineered, high-contrast dark system significantly reduces eye strain for frontline shift workers operating in low-light environments.
We also deepened our mastery of declarative state machines in React, learning how to leverage client-side storage structures to seamlessly mimic complex, distributed relational database systems entirely inside local runtime memory.
🔮 What's next for VitalVoice : AI-Powered Clinical Intelligence Platform
VitalVoice was architected from day one not as a disposable hackathon submission, but as a fully realized structural blueprint ready for scale. Our immediate technical roadmap includes:
- Production HL7 FHIR Infrastructure Integration: Upgrading our local data simulator arrays to hook directly into production-grade, open healthcare APIs, allowing VitalVoice to query real-time electronic health records straight from institutional medical networks like Epic Systems and Cerner.
- Biometric Security & WebAuthn Decoupling: Integrating FaceID and fingerprint biometric authentication natively through the browser’s WebAuthn API. This will keep the patient's private personal portal highly encrypted while ensuring the emergency QR triage link remains entirely unauthenticated and open for instantaneous paramedic scanning.
- Passive NFC Wearable Tokens: Transitioning the digital emergency QR indicator off smartphone screens and onto durable, waterproof, passive NFC-enabled medical wristbands, smart rings, and physical wallet cards—allowing first responders to simply tap a tablet against a patient's wrist to summon the VitalVoice interface instantly.
Built With
- html5
- javascript
- lucid
- react
- tailwind
- v0.dev

Log in or sign up for Devpost to join the conversation.