-
-
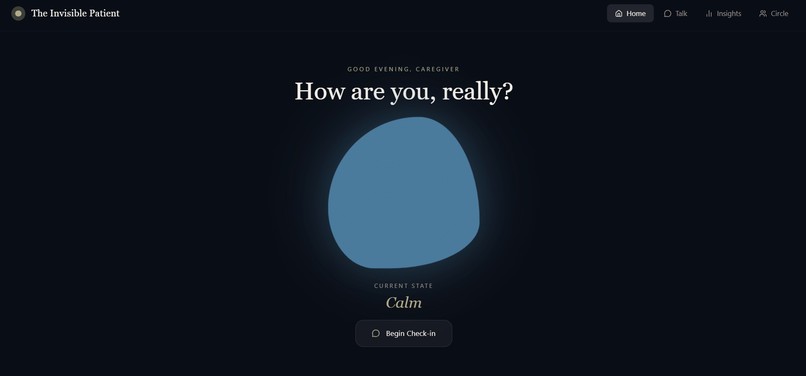
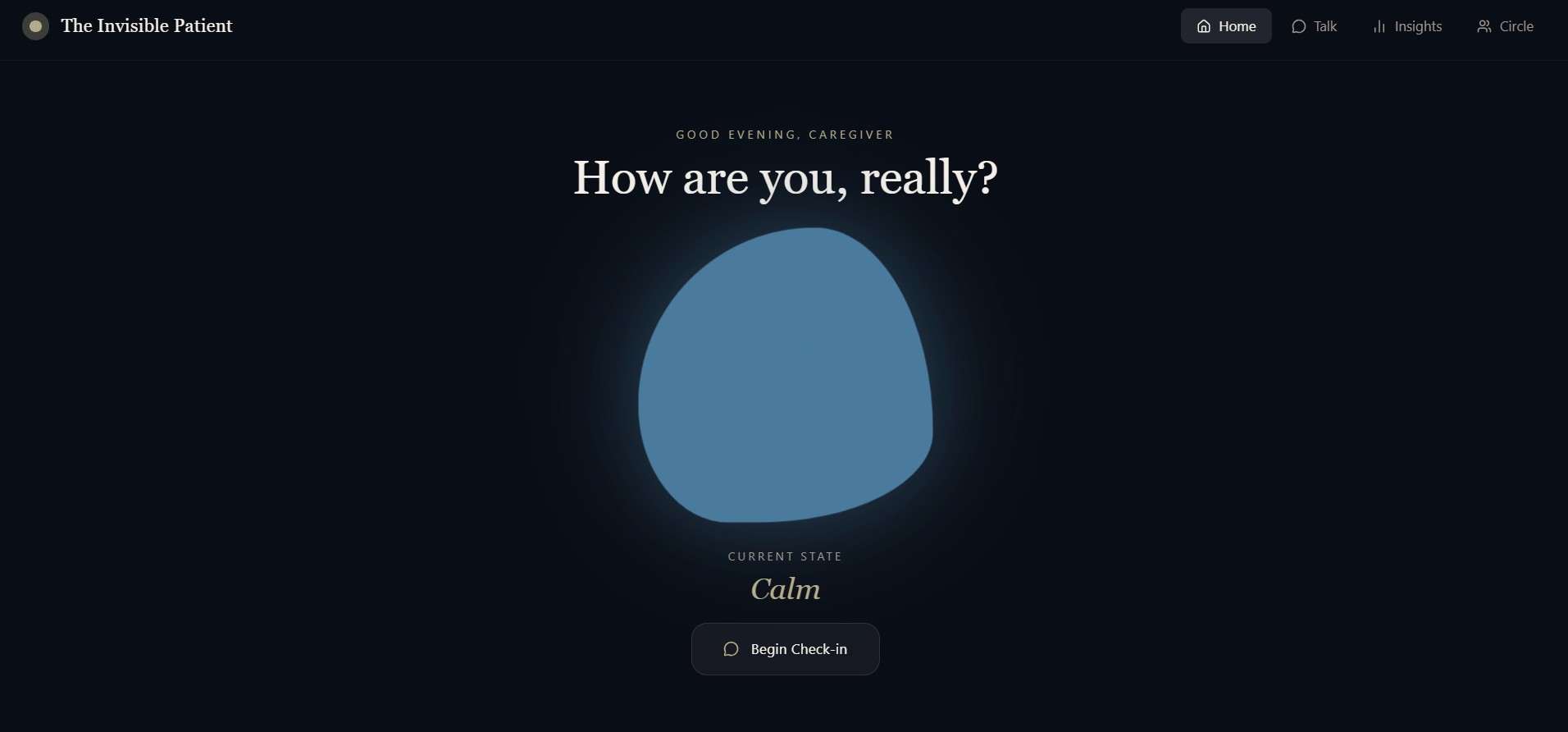
The Home Page
-
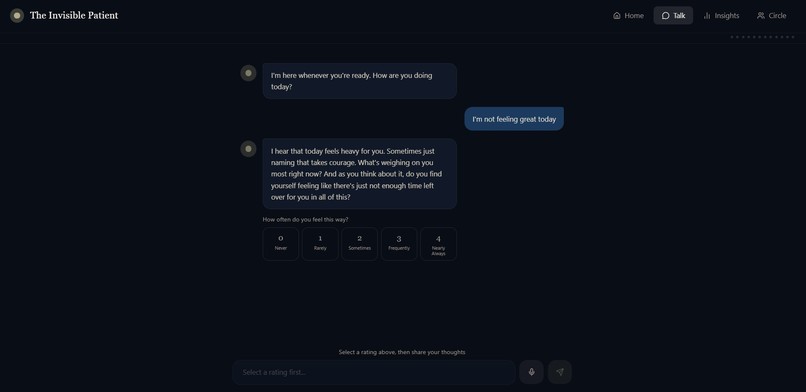
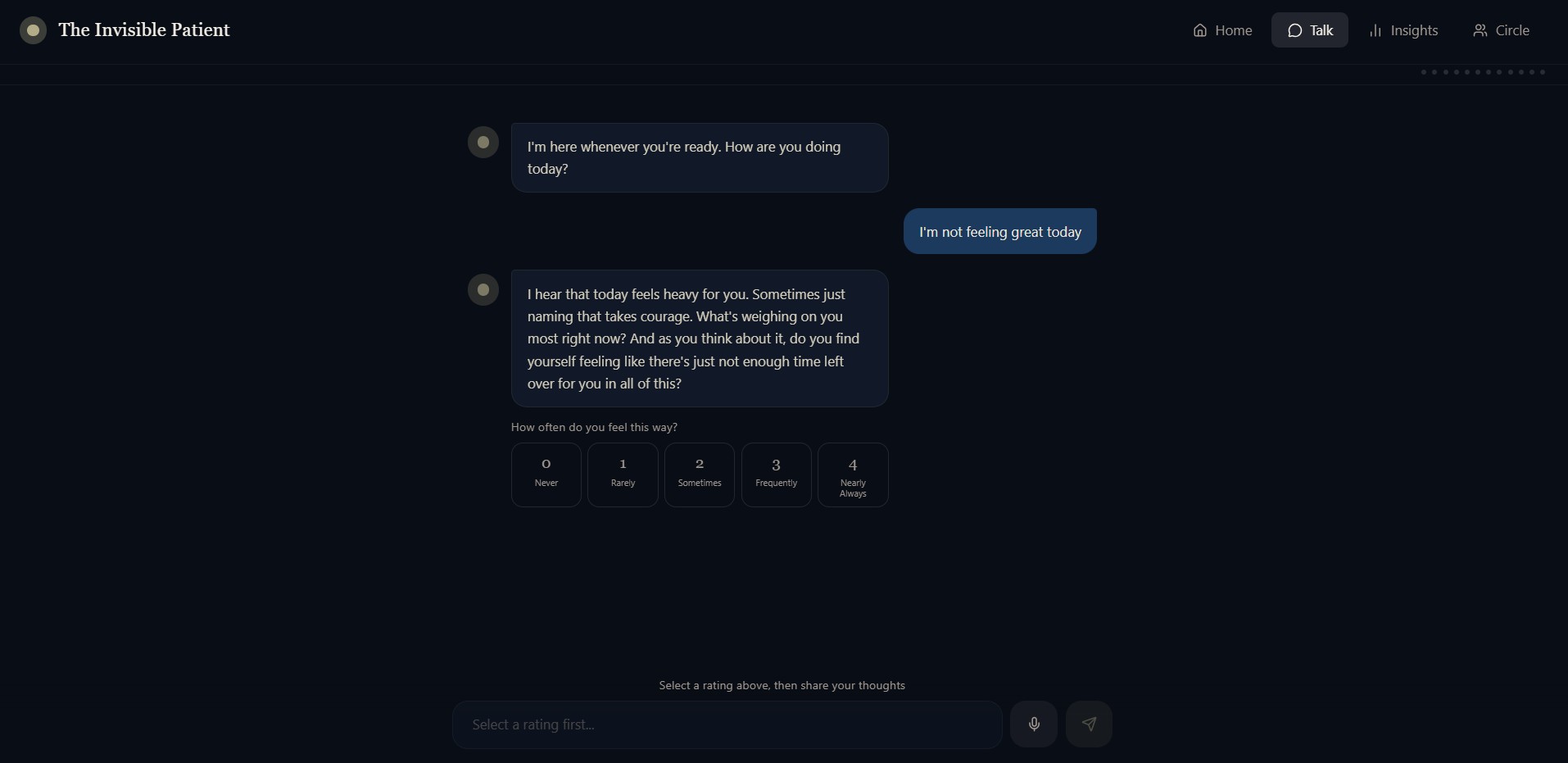
The Chat Page (Voice+Text)
-
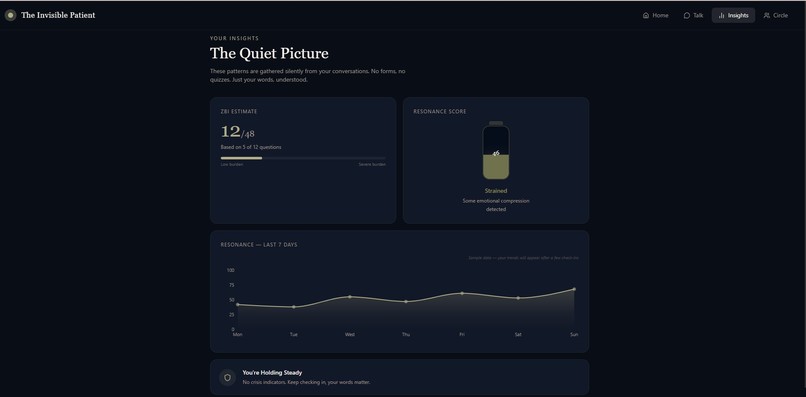
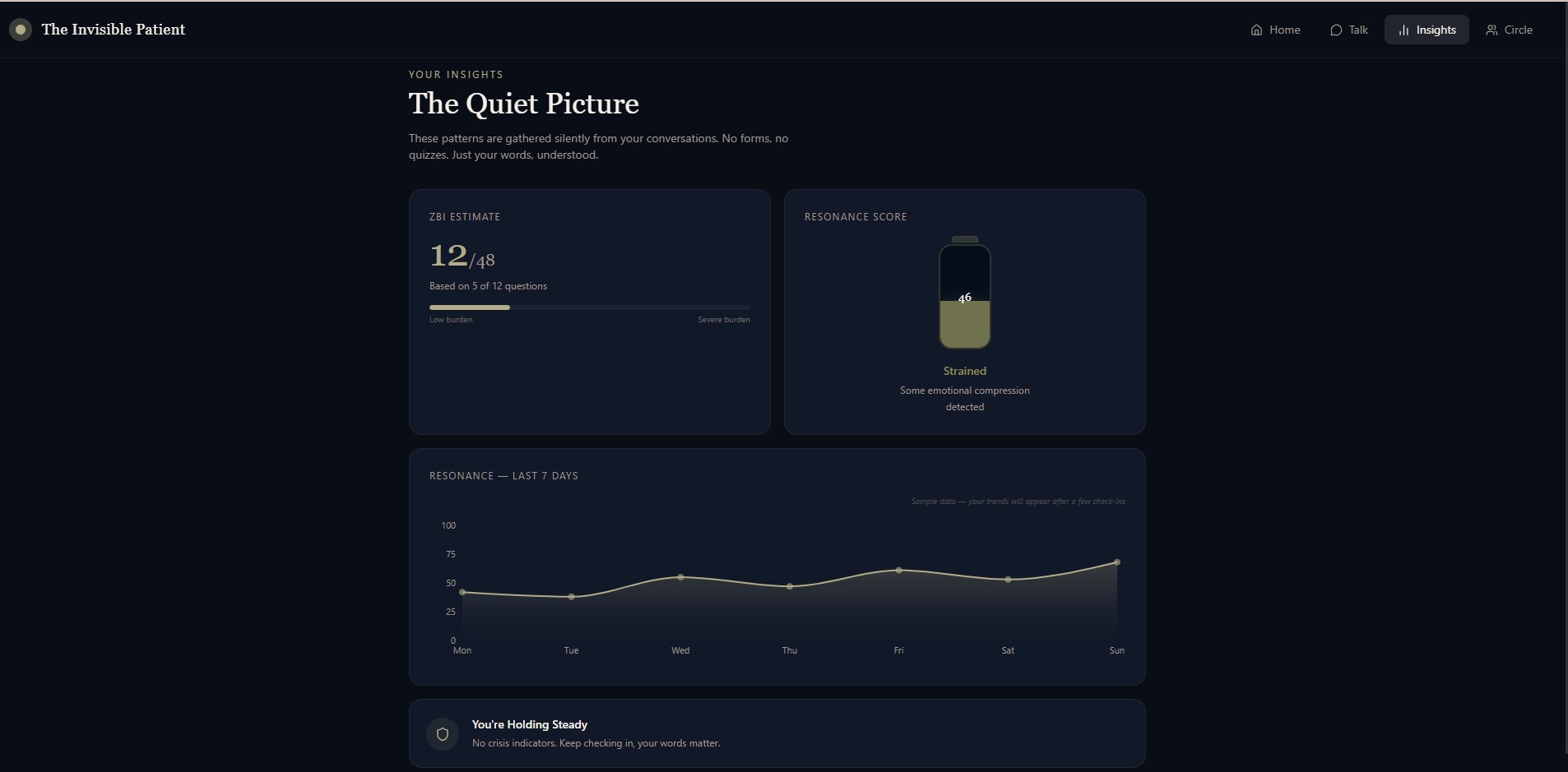
The Insights Page
-
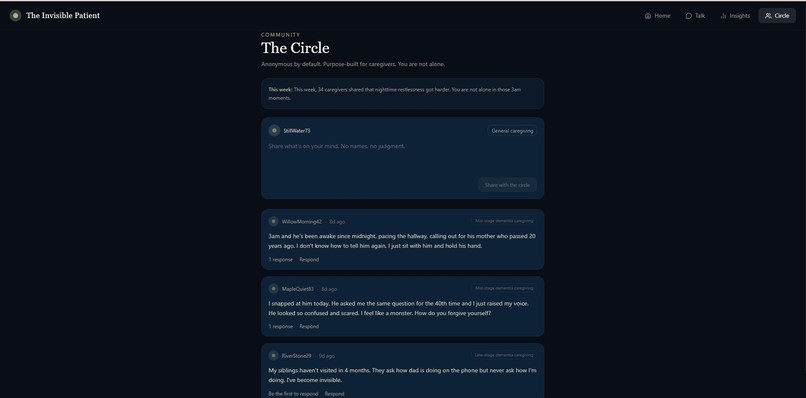
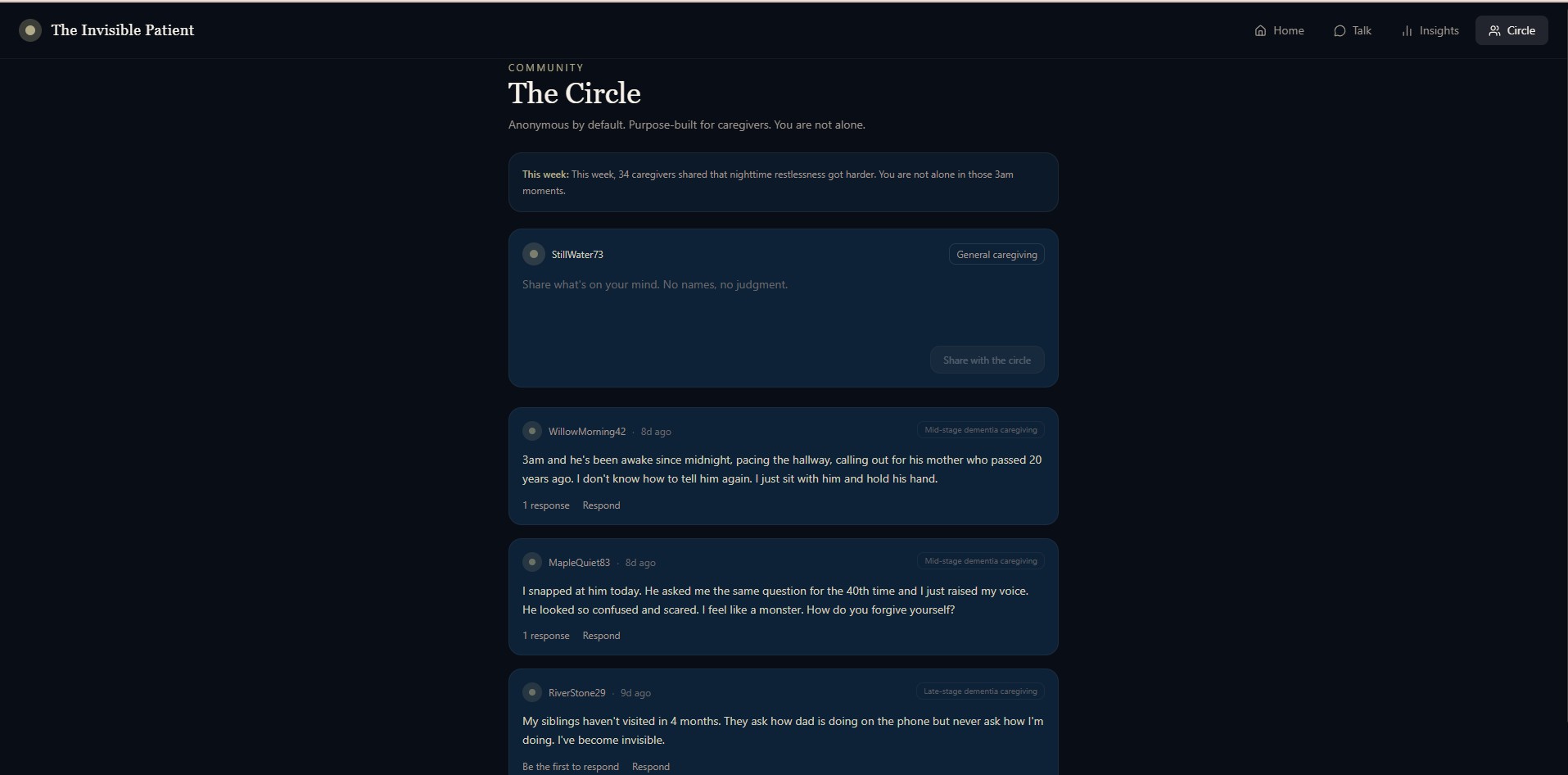
The Circle Community Page
INSPIRATION : WHERE THIS STARTED
It was not in a research lab. It was in our own home, at 3am, watching someone we love stand completely still in the middle of the room, not lost, exactly, but no longer quite findable. A family member who had been caring for a relative with Alzheimer's for two years. She had stopped sleeping in full nights. She had stopped finishing sentences about herself. She had started saying "I'm fine" the way people say it when they have forgotten what fine actually feels like.
We are a team with backgrounds in health-tech, data science, and AI. We know what burnout looks like in a dataset. But we had never felt it the way we felt it watching her disappear quietly, without anyone noticing, without a single system in the world designed to catch her.
She was not the diagnosed patient. Nobody was measuring her. Nobody had built anything for her.
And then we asked a harder question: how many people in the healthcare system are living the same version of this story not as family members, but as their profession?
The answer broke open the entire problem space.
WHAT IT DOES
We built The Invisible Patient for dementia caregivers. But the deeper we went, the more clearly we saw that the invisible patient is not just a family member at home at 3am. The invisible patient is also the ICU nurse who has watched six patients die this month and has not processed a single one of them. The invisible patient is the primary care physician burning out at a rate of 48–57% depending on specialty, quietly making more errors, seeing fewer patients, and considering leaving medicine entirely. The invisible patient is the social worker, the pharmacist, the oncology nurse, the medical student absorbing trauma they were never taught to metabolize.
The healthcare system is extraordinarily good at measuring the health of patients. It has built almost nothing to measure the health of the people delivering care.
The Invisible Patient is the infrastructure that changes that.
In 2022, 46% of health workers reported feeling burned out often or very often, compared to 32% in 2018. That is not a slow drift. That is a structural crisis that accelerated sharply and has not returned to baseline.
Primary care physicians consistently show the highest burnout of any occupation, ranging from 46.2% in 2018 to 57.6% in 2022. Several occupations saw burnout levels increase by 10% or more between 2018 and 2023.
When respondents were asked if they felt burned out in the past month, 50% answered yes in 2023. Pharmacy professionals experienced the most burnout at 62%. Burnout for nurses and physicians stood at 52% and 51% respectively.
From 2018 to 2022, health workers reported an increase of 1.2 additional days of poor mental health per month. The percentage reporting burnout very often rose from 11.6% to 19%.
And then there are the 11.5 million family caregivers alongside all of this, providing an estimated 18.4 billion hours of unpaid care annually, with 2 in 3 reporting difficulty finding resources and support for their own needs.
Every single one of these people, the ICU nurse, the burned-out physician, the family caregiver at 3am shares one thing: they are carrying someone else's pain for a living, and nobody is monitoring what that is doing to them.
The Invisible Patient monitors them. Passively. Continuously. Without adding a single thing to their to-do list.
HOW THE PRODUCT WORKS
The entry point is a conversation. Not a survey. Not a wellness check-in form. Not a mood slider. A conversation available at 2am, available in the car between shifts, available in the three quiet minutes before it starts again. The system simply asks: How are you doing today?
Underneath that question, a silent diagnostic architecture runs in real time. Every message is analyzed across four linguistic dimensions that together produce the Resonance Score, our proprietary 0–100 metric for psychological coherence: Lexical Diversity (Type-Token Ratio, 30% weight), Mean Sentence Length (15% weight) , Elaboration Ratio (15% weight), Contextually-Weighted Sentiment (40% weight).
Simultaneously and this is what separates us clinically, the Zarit Burden Interview (12-item version) for caregiver populations, and equivalent occupational stress frameworks for clinical professionals, are administered invisibly inside natural conversation. No forms. No surveys. The assessment happens while the person thinks they are just talking. We rephrase each validated clinical question as a moment of genuine human curiosity: "Between your shifts and everything you carry home from them, do you ever feel like there is nothing left for yourself at the end of the day?" The user can respond by tapping a 0–4 scale button or by typing freely. Both inputs are captured. Both are mapped.
The result is a Burden Weight, a longitudinal clinical estimate tracked across weeks paired with a Resonance Score that captures the psychological health of how someone communicates over time. Together these form a brain health portrait of the user, updated every session, stored longitudinally, and available for clinical review when thresholds are crossed.
When the Burden Weight climbs into the moderate-to-severe range, the system does not alarm. It says, gently: "You may be carrying more than one person can hold. Here is someone who can help." Real numbers. Real resources. Framed as care, not warning.
When crisis language appears, harm ideation, thoughts of quitting the profession, self-destructive ideation, the system responds immediately, with compassion first and crisis resources second, and it does not abandon the conversation. It stays.
The Circle is the community layer, a small, anonymous forum where users can post without identity, where an AI moderator monitors for crisis signals, and where a weekly AI digest tells the community: "This week, 63 healthcare workers here shared that the hardest part was not the clinical work, it was feeling invisible to the institution they gave everything to. You are not alone."
HOW WE BUILT IT: INNOVATION & TECHNICAL IMPLEMENTATION
The companion runs on Anthropic Claude Sonnet via the Messages API with a dual-track architecture: every user message simultaneously triggers a response generation call (empathetic, validating, clinically precise) and a silent analysis call (structured JSON output mapping the conversation to clinical indicators). The caregiver never sees the analysis. They only see the conversation.
The system prompt is built around Reflective Validation, a therapeutic communication framework that mirrors emotions back without judgment with warmth and precision. We rewrote this prompt many times. We debated individual words. We tested it against real emotional scenarios until every response felt worthy of the moment it would appear in.
Web Speech API — SpeechRecognition for input, SpeechSynthesis for output. Rate 0.88. The warmest available female voice. Because a nurse coming off a night shift who cannot hold a phone steady should still be able to talk to the system and hear something human come back.
ZBI-12 for caregiver populations. Occupational burnout frameworks (Maslach Burnout Inventory dimensions — emotional exhaustion, depersonalization, personal accomplishment) mapped conversationally for clinical professionals. PHQ-9 passively inferred from language patterns. All thresholds mapped to validated clinical scoring ranges. All resource referrals triggered by evidence-based cutoffs, not arbitrary scores.
IMPACT & USE CASE : WHO BUYS IT, HOW MUCH, AND WHY
The global mental health technology market was worth $15.22 billion in 2024 and is expected to reach $30.98 billion by 2030. Every major player in this market: Headspace, Calm, Lyra Health, Spring Health, BetterHelp, Woebot is competing for the same user: a working adult who is stressed but functional, who has time to open an app, and who can self-identify a problem and engage with a solution on the product's terms.
Not one of them was built for the healthcare worker who has been trained since medical school to suppress distress as a professional requirement. Not one of them does passive, longitudinal monitoring. Not one of them administers validated clinical assessments inside natural conversation without the user knowing. Not one of them has a clinical moat built from the only longitudinal mental health dataset on healthcare workers and caregivers at scale.
That is the white space. It is not a niche. It is the most mentally distressed, most underserved, most economically consequential population in the healthcare system.
Customer Segment 1 - Hospital Systems and Health Networks (highest contract value)
The problem they are already paying for: A burned-out physician costs a hospital system $500,000–$1,000,000 to replace when they leave, accounting for recruitment, onboarding, and lost revenue. Medical errors which increase measurably with clinician burnout cost the U.S. healthcare system an estimated $20 billion annually. When a family caregiver collapses, the patient they were supporting arrives in the ER. The average Alzheimer's-related hospitalization costs $30,000–$75,000. The hospital is already paying for burnout. They just call it something else on the balance sheet.
What we sell them: A per-user clinical monitoring dashboard. Burden Weight and Resonance Score tracked across weeks for every enrolled clinician and caregiver in their network. Early deterioration flagged before it becomes a leave of absence, a medical error, or a hospitalization. A social worker intervention triggered two weeks earlier than it would have been triggered without the system.
Example: UW Health has approximately 20,000 employees. Enroll 30% of clinical staff at $300/user/year: $1.8M ARR from one health system. The ROI justification writes itself prevent two physician departures and the contract pays for itself five times over.
Example: A memory care network with 3,000 active patient families. Enroll the caregiver alongside the patient at $200/caregiver/year: $600K ARR per network. The value proposition is reduced patient hospitalizations from caregiver collapse events which the network is already absorbing.
Customer Segment 2 - Medicare Advantage Plans and Insurers (massive TAM)
CMS added caregiver support as a covered supplemental benefit for Medicare Advantage plans. Insurers are now financially incentivized to prevent caregiver collapse because caregiver collapse drives patient hospitalizations that they pay for. We sell them population-level risk scores, a Resonance Score and Burden Weight for every covered caregiver at $15–$30 per member per month. Across a mid-size MA plan covering 50,000 caregivers, that is $9–$18M ARR from one insurance contract.
Customer Segment 3 - Employers with Healthcare Workforces (fastest to close)
Harassment at work was associated with increased odds of burnout of 5.83x among health workers. Hospital systems are employers. They are buying Headspace for Work and Lyra Health right now paying $8–$20/employee/month for general mental health benefits that were not built for the specific stressors of clinical work, do not passively monitor, and generate no longitudinal data. We are the replacement. Purpose-built for the profession. Clinically grounded. Passively monitoring. A premium product at a premium price point.
Customer Segment 4 - Direct to Consumer (acquisition engine)
$9.99–$19.99/month subscription. Family caregivers, healthcare workers between employer contracts, medical students. This is not the core revenue engine. This is the data flywheel, every session generates longitudinal mental health data that makes the clinical models sharper, the risk scores more accurate, and the product more defensible against every competitor who tries to follow us in.
The Data Moat: This is the asset that compounds. Every conversation, anonymized, aggregated, longitudinal becomes part of the only dataset of its kind in existence: real-time mental health trajectories of caregivers and healthcare workers, tracked across weeks and months, mapped to validated clinical frameworks. That dataset answers questions nobody has answered:
- At what point in disease progression do family caregivers show the steepest Resonance Score decline?
- Which linguistic markers predict a physician taking leave within 60 days?
- Which intervention, surfaced at which moment, produces a measurable improvement in Burden Weight within two weeks?
Pharma companies will pay for this data. Health systems will pay for this data. Academic medical centers will co-publish with us using this data. The product is the acquisition engine. The data is the moat.
UI/UX & DESIGN: CALM TECH FOR A CLINICAL TOOL
The design language is Midnight Serenity: Deep Navy (#0A192F), Soft Sage Green (#B2AC88), Warm Ivory text. No harsh reds. No alarming oranges. No clinical white. The aesthetic is deliberately premium and calm, it should feel like the most thoughtful room you have ever sat in, not a hospital waiting area.
Home screen: A single breathing aura, a liquid-motion blob that shifts color based on the user's current detected mental state. Calm shifts to sage. Stressed shifts to muted amber. Crisis signals appear as a deepening of the navy, never a harsh alert. One button: Begin Check-in.
Talk screen: Clean, dark chat interface. Large, friendly typography. The AI's messages arrive with the cadence of a thoughtful human response never instant, never robotic. Voice mode is a single microphone button. The AI responds in audio. The conversation feels like a call with someone who is genuinely unhurried.
Insights screen: A bento-grid dashboard two stat cards (Burden Weight /88, Resonance Score /100), a Neural Battery visualization, and the Your Journey chart showing both metrics across weeks with explicit directional notes: Burden Weight lower is better. Resonance Score higher is better. No jargon. No interpretation required.
The Circle: Card-based anonymous forum. Clean, minimal, with a candle icon for support reactions not a like, not a heart, something that acknowledges weight without reducing it to engagement metrics.
Every crisis resource is surfaced in muted sage, not red. The design principle throughout: care that does not feel clinical. Infrastructure that does not feel institutional.
CHALLENGES WE FACED
The hardest part was not technical. We know how to build the technical parts. The hardest part was calibration, understanding the difference between a system that processes distress and a system that is worthy of it. The second challenge was clinical restraint. The temptation when you have a system this sensitive is to overclaim to say the Resonance Score predicts burnout, to say the ZBI estimate diagnoses burden. We refused. The system offers patterns, not verdicts. It surfaces insights, not diagnoses. That restraint required active discipline against the pull of the product's own capability.
The third was scope management. Once we saw that the invisible patient is not just the family caregiver but also the clinical workforce , the nurse, the physician, the pharmacist, the social worker, the product had to expand without losing its soul. The core insight passive, longitudinal, conversational monitoring of the people nobody is monitoring had to hold at every scale. We believe it does.
ACCOMPLISHMENTS WE ARE PROUD OF
We are proud that the app never asks anyone to fill out a form. The entire clinical assessment happens inside a conversation that feels like being heard. That is not a feature. That is the design philosophy, held consistently across every screen, every prompt, every AI response.
We are proud of the Resonance Score. It is not borrowed from another domain or adapted from a general-purpose sentiment tool. It was designed from first principles for people who have been trained to suppress emotional distress because their language of distress is not "I am struggling." It is narrowing. It is fragmentation. It is the slow disappearance of elaboration. The score measures the shape of that disappearance.
We are proud that The Circle exists. There was no purpose-built anonymous forum for healthcare workers and caregivers. There should have been for decades. We built it in five days.
WHAT'S NEXT: THE ROADMAP
Immediate (0–6 months): A six-week clinical pilot with one hospital system or memory care network. The infrastructure is HIPAA-ready. The clinical framework is validated. We need a cohort, a control group, and a dataset that validates the Resonance Score against gold-standard clinical assessment administered by licensed professionals.
Near term (6–18 months): Hospital system SaaS contracts. Insurance partnerships. Medicare Advantage channel. Expansion of clinical framework to cover occupational burnout dimensions, Maslach Burnout Inventory mapping alongside the ZBI, to serve clinical workforces alongside family caregivers under a single platform.
Medium term (18–36 months): A clinical decision-support dashboard for care coordinators and HR administrators showing, alongside a patient's chart, the mental health trajectory of their family caregiver. Showing, alongside a hospital floor's staffing data, the aggregate Resonance Score trend for nurses on that unit. Population-level insight that makes the invisible visible at institutional scale.
Long term: The dataset. The longitudinal mental health data generated at scale becomes an academic and commercial research asset that no competitor can replicate because they do not have the head start, the clinical grounding, or the user trust.
The caregiver has been the invisible patient for decades. The burned-out nurse has been invisible for decades. The physician quietly considering leaving medicine has been invisible for decades.
We built the system that finally sees all of them. We are not finished. 🌿
Built With
- date-fns
- framer
- linguistic-wellbeing-analysis
- lucide-react
- next.js
- react
- recharts
- speech-recognition
- speech-synthesis
- tailwind
- typescript
- zarit-burden-interview

Log in or sign up for Devpost to join the conversation.