-
-
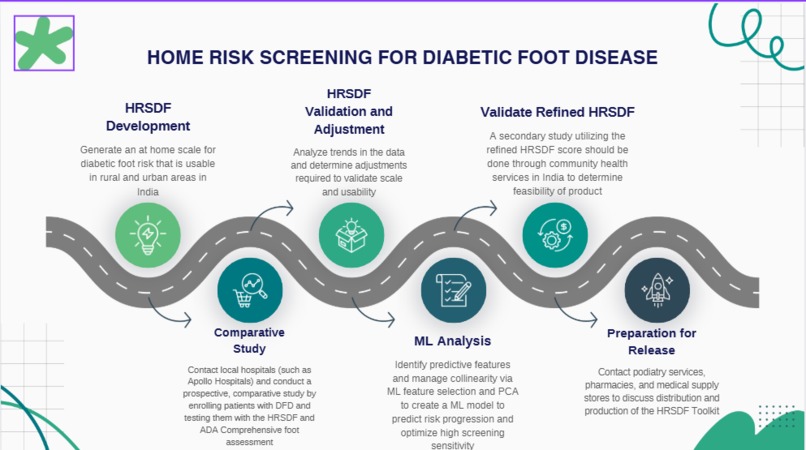
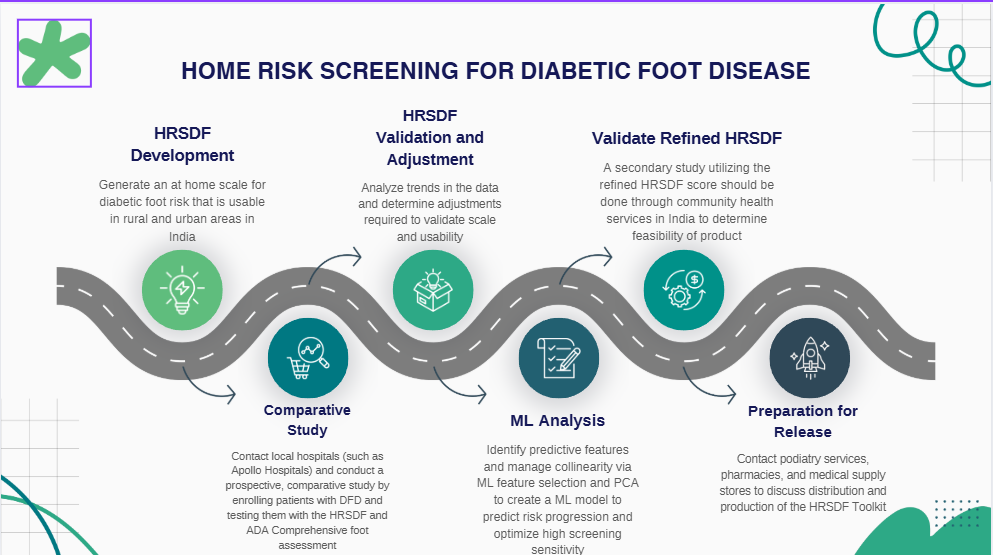
Roadmap for development of the HRSDF Assessment
Inspiration
While working as a clinical researcher specialized in diabetic foot disease, I have seen countless individuals struggle with maintenance of their condition. Many patients often feel ashamed or scared, and it discourages them from seeking help early on. The issue of poor-compliance goes beyond the fear of seeking help, but, cost, time, and education. Many patients around the world are given various clinical tests without truly knowing what they are being tested for or how the results will affect their lives. That inspired us to create the HRSDF Assessment.
What it does
The HRSDF Assessment utilizes materials that are of low cost, with tools that can be reutilized from patient to patient. Due to India being one of the most diverse countries in terms of language variety, the instructions in this booklet are put into simple words for easy translation and paired with various images to assist in guiding this exam. Along with each test is a simple explanation on what is being tested, how it relates to diabetic foot disease, and instructions for each exam. This exam can be done by home-health workers, family, or clinicians, allowing for a risk assessment to take place in the privacy of one's home or a clinic. Along with this, the kit contains a year's supply of monthly tests, allowing us to utilize machine learning to generate a prognosis based on HRSDF data collected over a year. Our goal is affectively generate a prognosis of a patient's diabetic foot disease and empower them to seek further clinical care to prevent further progression.
How we built it
This test is a modified version of the ADA Comprehensive Diabetic Foot Risk Assessment. We modified this assessment so that it was simple enough for a family member to do, detects and categorizes patients based on what stage of diabetic foot disease they are in, and provides us with longitudinal data that can be integrated into a ML model to predict further progression. A great deal of research was done into potential factors that can increase diabetic foot ulceration risk and DFD progression. We looked for physiological and lifestyle factors, as well as clinical characteristics of neuropathy and peripheral artery disease. Based on how these conditions are detected, scaled, diagnosed, and treated, we generated a scale for PAD, neuropathy, visuals, and biometric considerations to create a comprehensive foot exam. Our main goal with this exam was making it accessible to anyone, overcoming the psychosocial stigma that often prevents patients from seeking help.
Challenges we ran into
A major challenge we ran into when developing this scale was the development of a PAD risk assessment. Peripheral artery disease is often diagnosed based on vascular studies, along with ABI and TBI data. These exams are not available at home and require a degree of skill that would not be easy to teach in a simple booklet. To compensate, we looked at clinical characteristics and findings of PAD, and generated our scale based on these scores. While it may not detect PAD, patients who score high in this portion of the assessment likely have vascular insufficiency or dysfunction in their lower limbs, which is a cause for concern.
Accomplishments that we're proud of
We are very proud of the machine learning model we proposed to predict prognosis and validate the HRSDF assessment. Not only does this model allow us to compare our scale to more well-known scales, such as the MNSI or ADA Comprehensive Diabetic Foot Risk Examination, it also allows us to determine how we can make this assessment more streamlined for the patient. Along with this, because the HRSDF assessment collects data over 12 months, we are able to generate a model that can predict how their DFD will progress given the trends in their scores. We have a limited background in programming and machine learning, so we are especially proud of this achievement.
What we learned
While many regions have the ability to detect and treat a variety of conditions, stigmas often prevent patients from seeking the help they need. By lowering the barrier of care, and letting patients determine themselves that something is wrong, and that they need to seek assistance, compliance and good outcomes can increase. Many in healthcare forget that most people do not live inside their world, and don't like being stuck in a hospital, exposed to the public asking for help. Many people do not want to hear they are unhealthy based on things they don't understand, but if we give the power of diagnosis and testing to the people, we can empower them to seek education and understanding of the conditions they are afflicted with.
What's next for The Home Risk Screening for Diabetic Foot (HRSDF) Assessment
We hope to first explore whether this system works in low-resource areas near us in a small, short-term study. This may be done through Grady Memorial Hospital or Emory Hospital, but this short-term study could act as our proof of concept to pursue further validation and implementation of this scale. In the future, we hope to contact hospitals such as Apollo Hospital in Chennai, or Breach Candy Hospital in Mumbai, to explore an implementation study in rural and urban areas of India to flush out and fully validate this study. If the HRSDF proves effective in India, not just on a clinical level but a social level as well, we then would hope to expand to other countries that face similar problems, such as Vietnam, Cambodia, China, and Mexico.

Log in or sign up for Devpost to join the conversation.