-
-

Homepage of the strain website
-
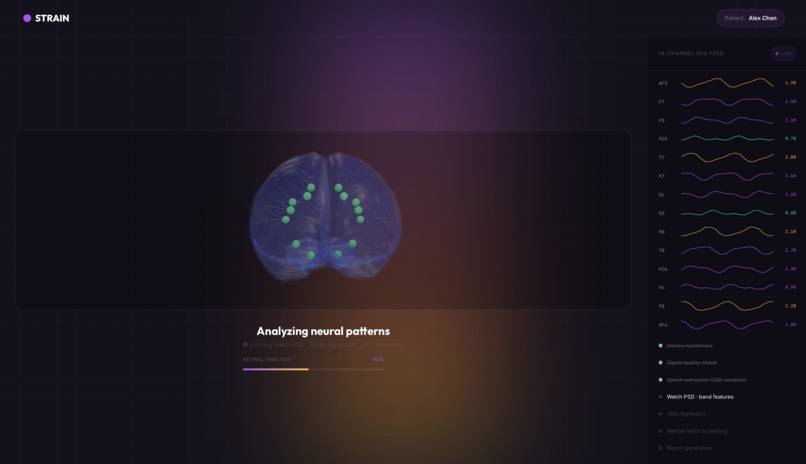
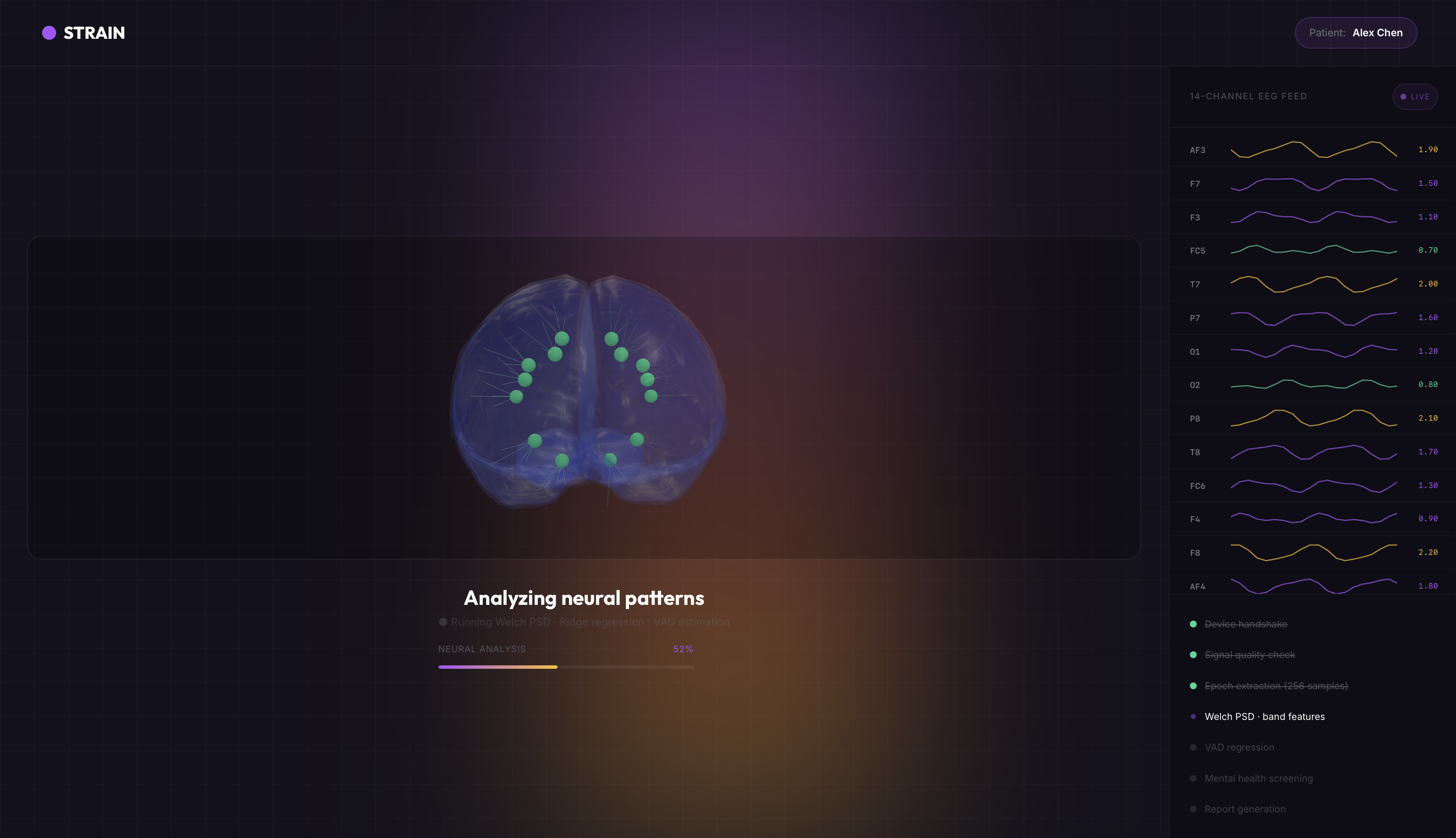
EEG scans being processed
-
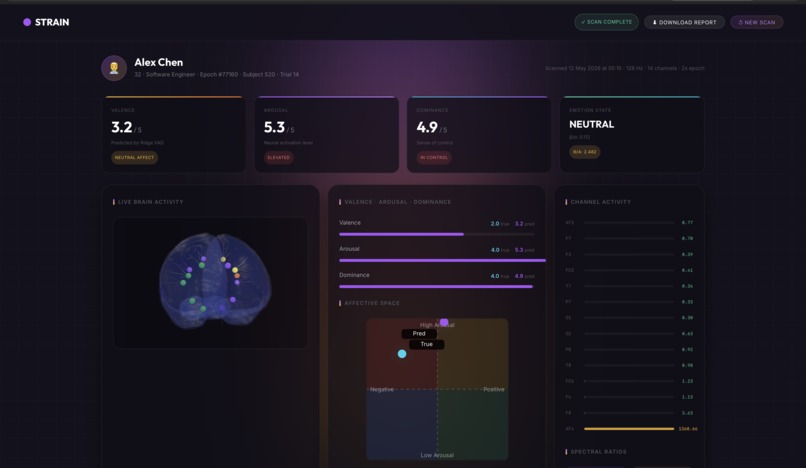
Results being generated after processing
-
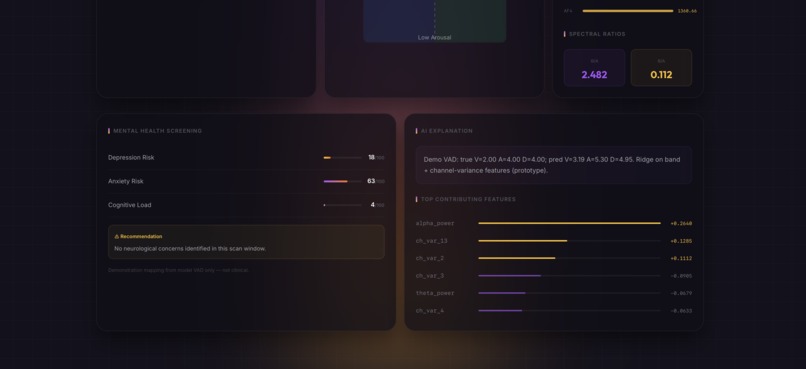
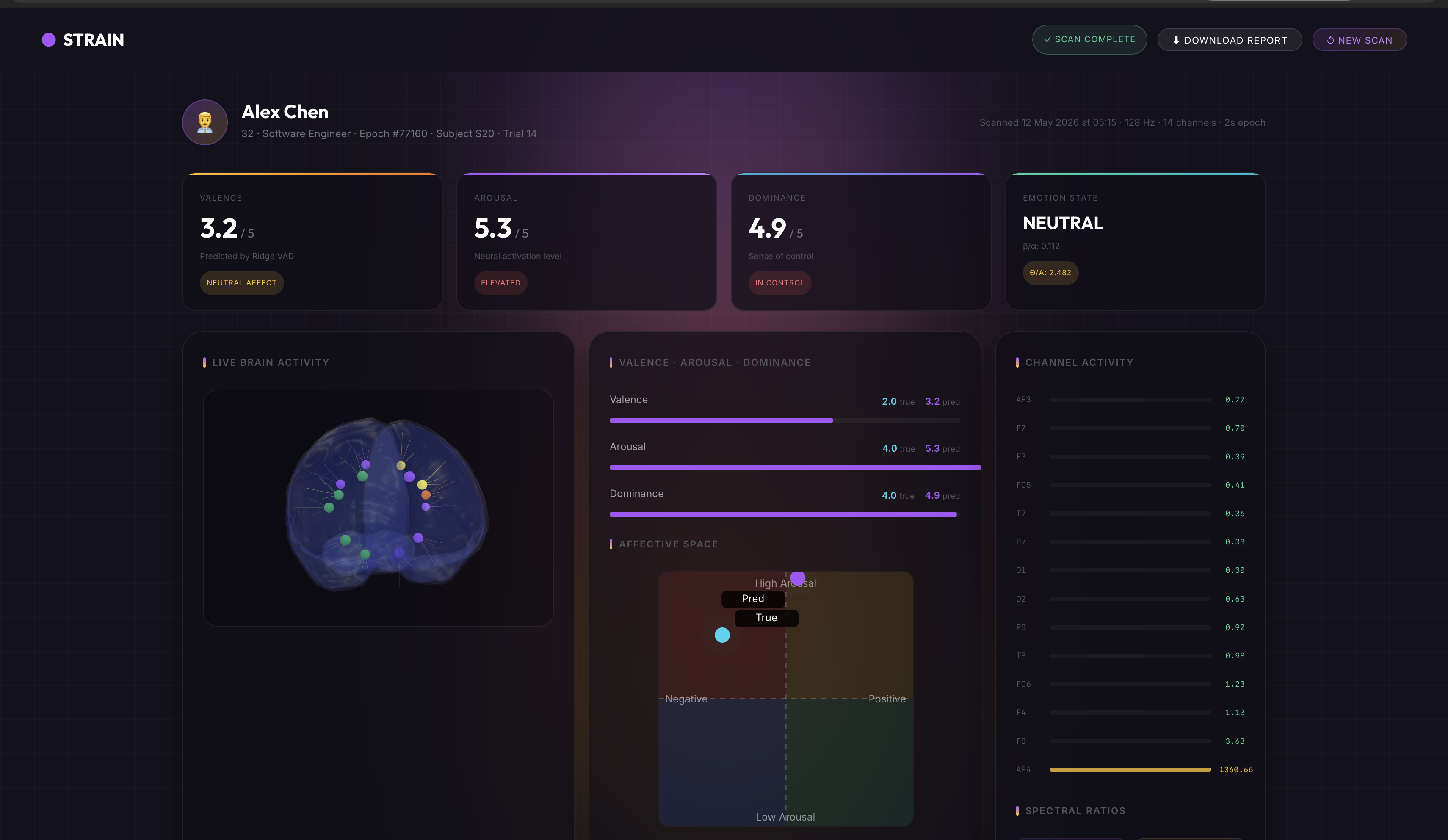
Statistics reported
-
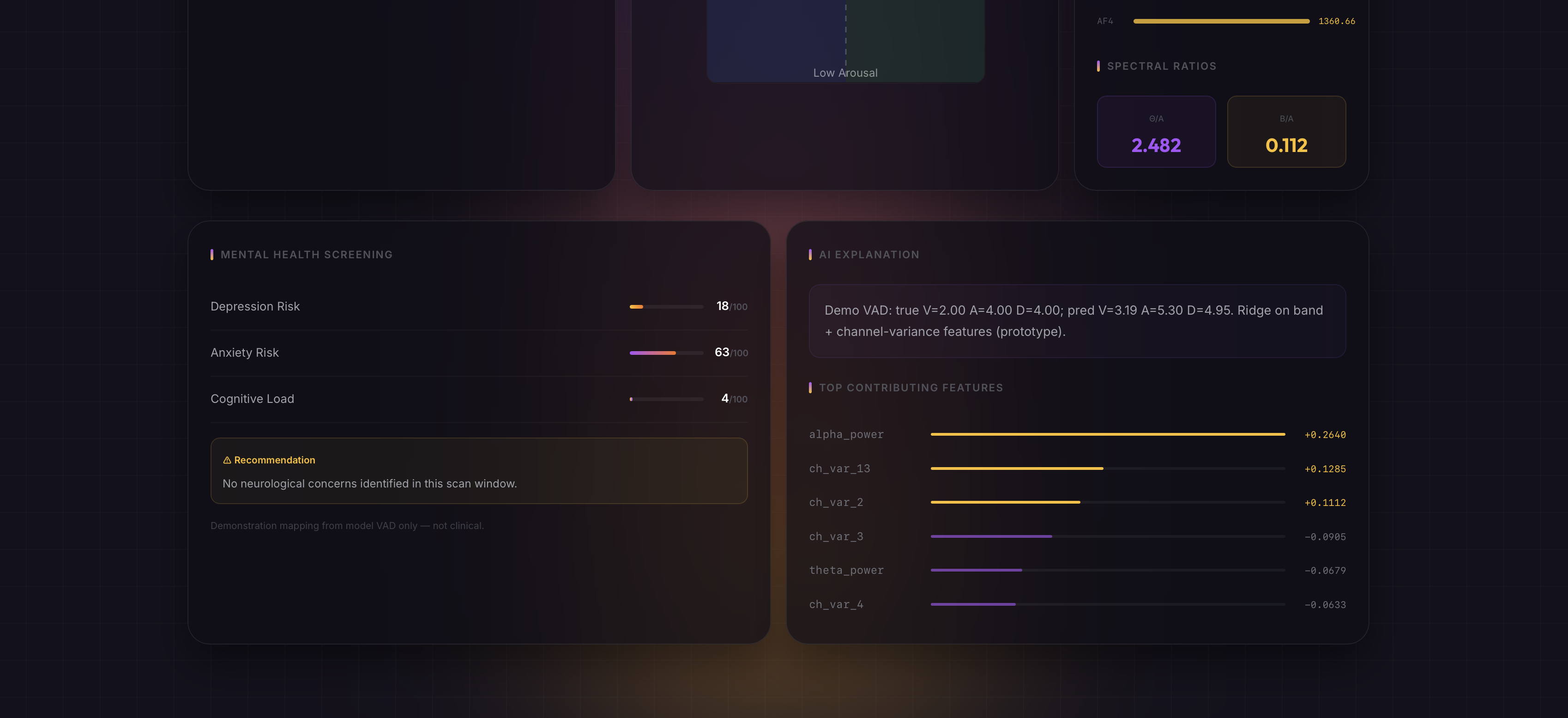
Report generated
-

Strain Logo
-
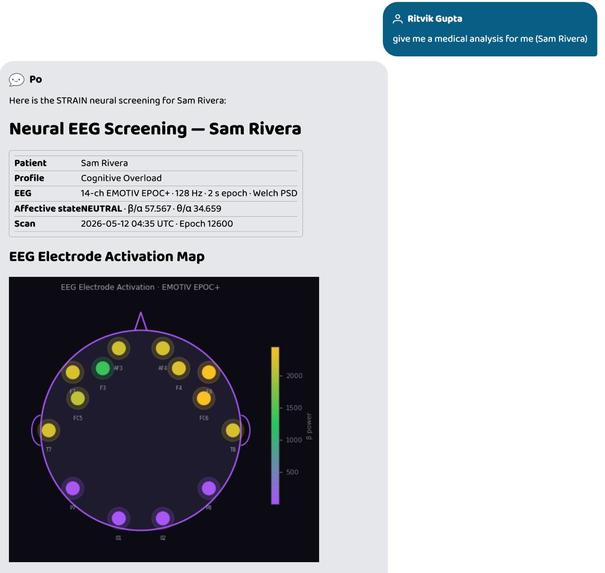
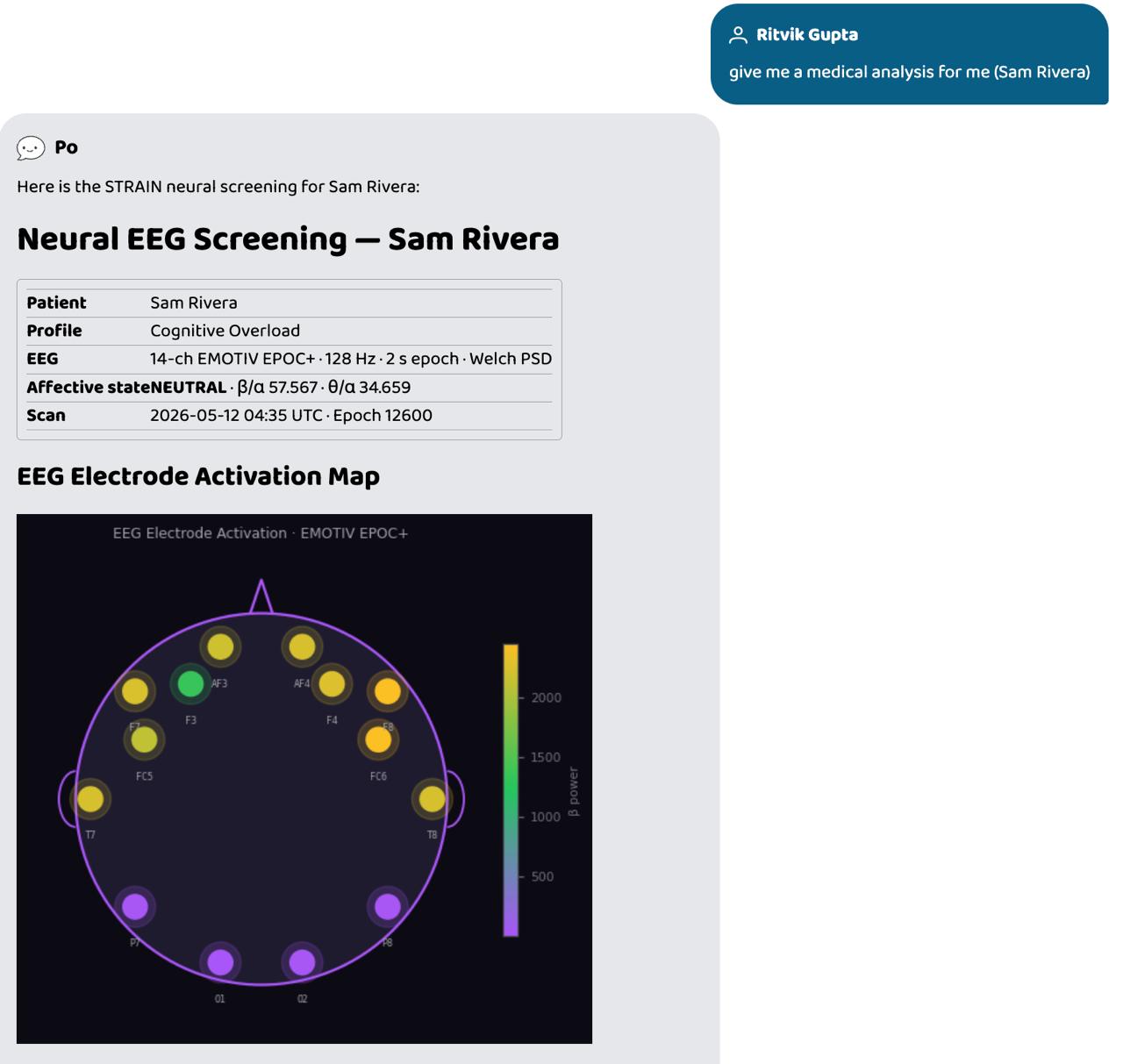
Output of strain agent by strain agent on Prompt Opinion platform
-
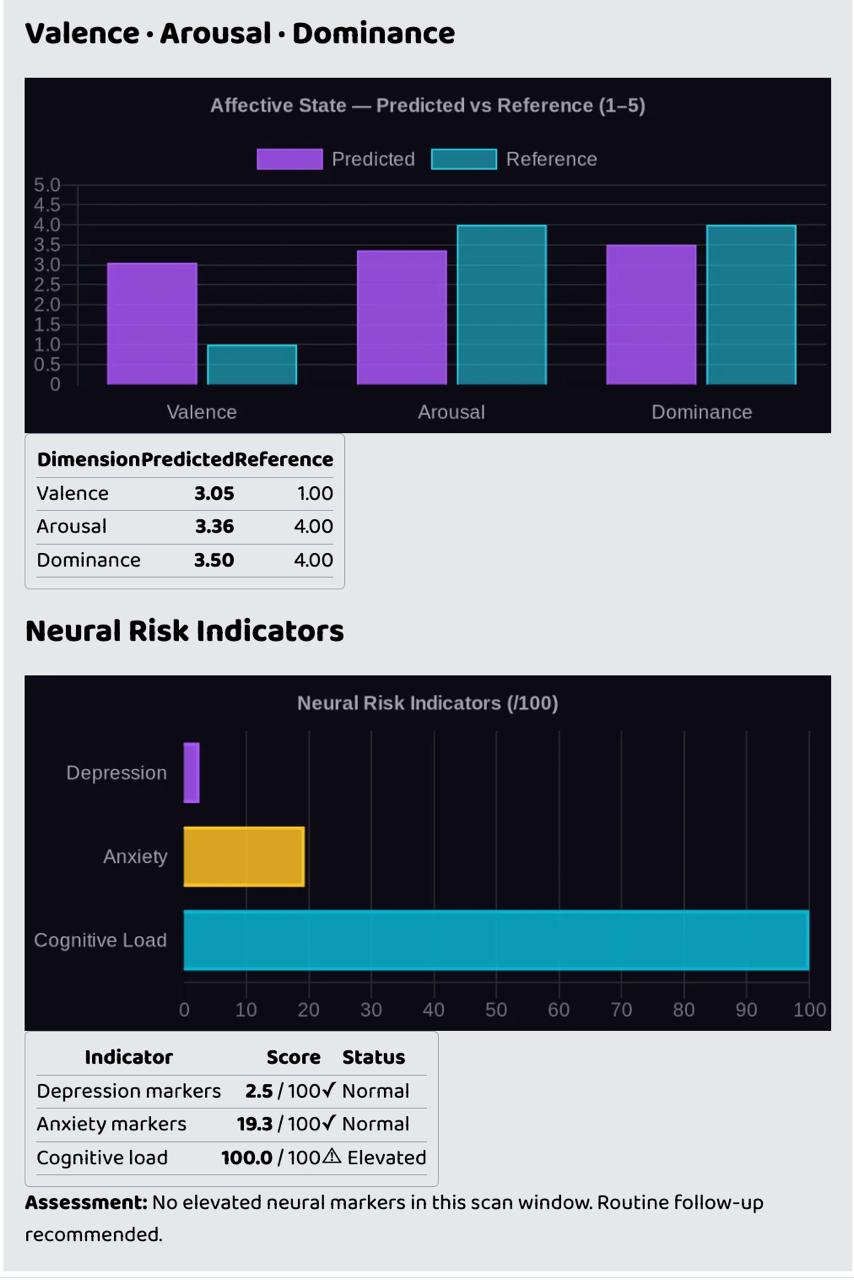
Graph + Image output
-
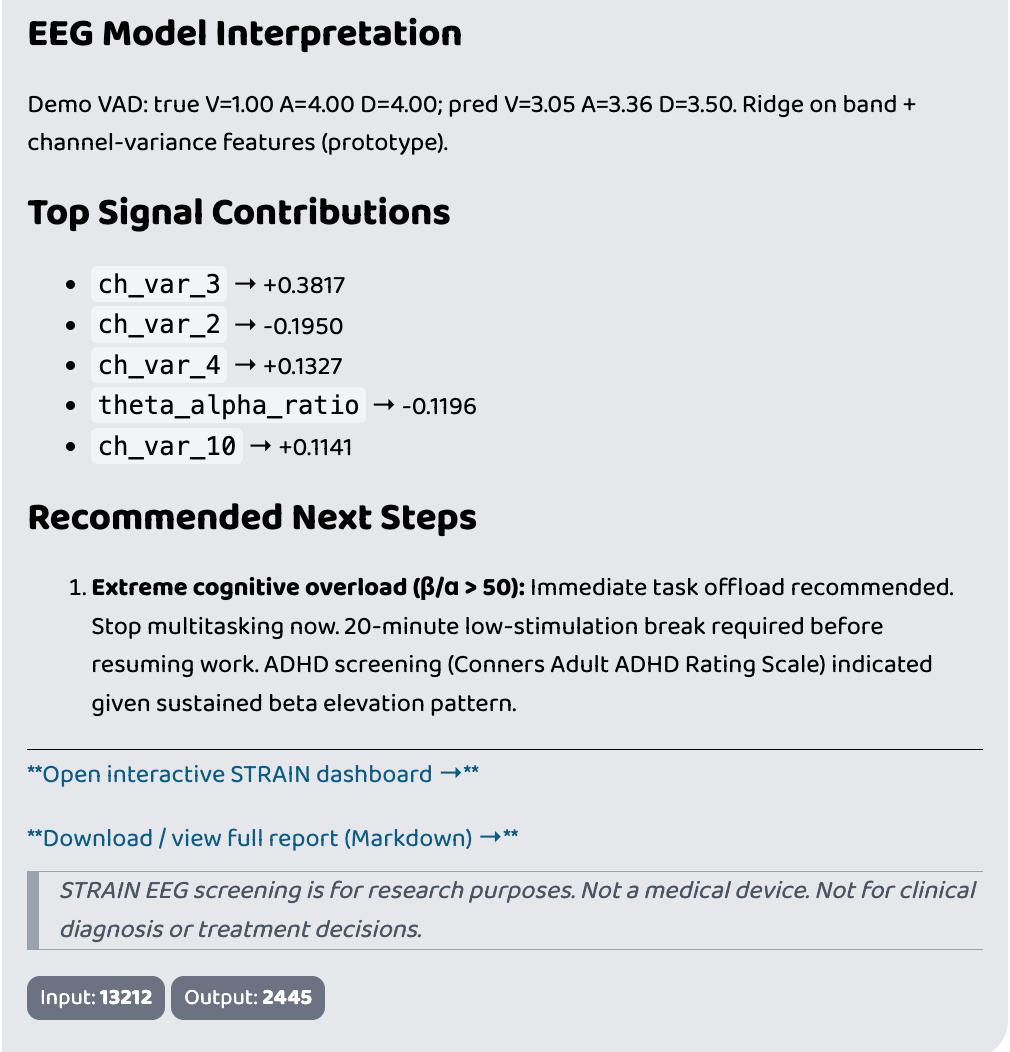
Markdown Report Output


Inspiration
Mental health care has a data problem. Clinicians rely almost entirely on
self-reported symptoms - but by the time a patient articulates that they're
overwhelmed, burned out, or unable to focus, they've often been struggling for
months. We asked: what if a 2-second brainwave snapshot could quantify what a
person can't put into words?
STRAIN (Stress and Affect Recognition via Neural Inference) was built to answer
that question.
What it does
STRAIN is a real-time EEG analysis platform that processes brainwave signals from a 14-channel EMOTIV EPOC+ headset to generate:
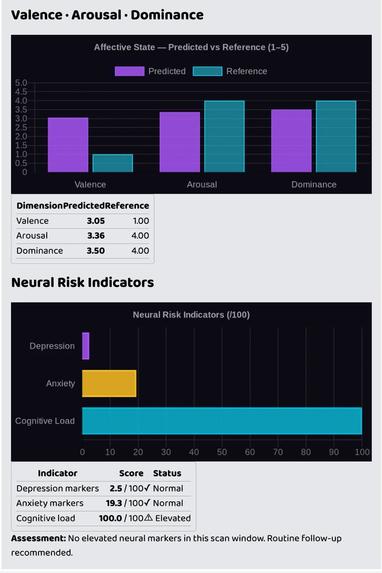
- Affective state predictions - Valence, Arousal, and Dominance scores (1–5) load (β/α ratio), mapped to a 0–100 clinical scale
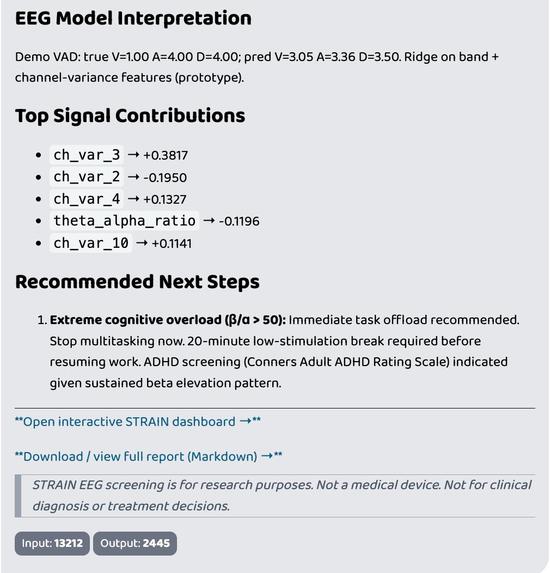
- Explainability - top EEG signal contributions (band power, channel variance) driving each prediction
- FHIR R4 export - structured clinical data bundles ready for EHR integration
The platform includes a full-stack web dashboard (React + Three.js 3D brain visualization), a FastAPI backend, and an MCP-connected AI agent on Prompt Opinion that can converse with patients, triage their symptoms, redirect them to a scan, and generate a full clinical report - complete with a downloadable Markdown file formatted for doctor consultation.
The demo narrative
Sam Rivera is a 26-year-old PhD student. She opens the STRAIN agent on Prompt Opinion and says she's overwhelmed - racing thoughts, can't focus, three deadlines she can't face. The agent empathises, explains that STRAIN can measure cognitive load directly from her brainwaves, and drops a link to the dashboard.
Sam runs a scan. Her results: Valence 1.0 / 5, Arousal 4.0 / 5, β/α ratio 57.6 (normal range: 1–3), cognitive load 100% - an extreme ADHD-stress overlap signature identified in the DREAMER dataset. She returns to the agent, asks for her analysis, and receives a full neural screening report with EEG electrode topography, VAD charts, risk indicators, and personalised next steps - including a recommendation for formal ADHD screening (Conners ACRS).
How we built it
Data pipeline: DREAMER.mat (Zenodo) → sliding-window export (256 samples, 50%
overlap, 128 Hz) → (14, 256) epoch tensors → Welch PSD feature extraction →
subject-holdout Ridge regression (VAD).
Backend: FastAPI orchestrator with agent pipeline (DataCurator →
AnalysisEngine → Explainer), FHIR R4 bundle generator, and a matplotlib EEG
electrode topography renderer.
Frontend: React 19 + TypeScript, Three.js/react-three-fiber 3D brain with
animated dendrite lines and electrode markers, 9-second animated scan sequence.
AI integration: FastMCP server exposing strain-tools over SSE/Streamable
HTTP. Connected to Prompt Opinion BYO agent - the agent calls
analyze_named_patient_tool, which runs the full pipeline and returns a rich
Markdown report with inline charts (QuickChart.io), brain scan image, and a
downloadable report URL.
Interoperability: FHIR R4 Observation bundles for all screening outputs -
designed for real EHR integration.
## Challenges
- EEG feature leakage: Getting subject-holdout cross-validation right so the
model generalises across people, not just memorises one subject's baseline. - MCP + LLM hallucination: The Po agent repeatedly fabricated URLs and patient
names until we locked the tool docstrings, removed example URLs, and added hard
REQUIRED:directives in the system prompt. - Real-time feel from batch data: The 9-second scan animation needed to feel
live while actually processing a pre-recorded DREAMER epoch - deterministic channel power seeding made it reproducible and convincing. - Clinical framing without overclaiming: Every output carries a disclaimer. The language is clinical but the system is explicitly not a medical device - threading that needle in the UI and agent responses took deliberate iteration.
What we learned
Brain-computer interfaces don't need to be invasive or expensive to be clinically
informative. A consumer-grade 14-channel headset, open research data, and a
well-structured ML pipeline can produce explainable, FHIR-ready outputs that a
clinician could actually use as a conversation starter - not a diagnosis, but a
signal worth discussing.
What's next
- Swap Ridge regression for a subject-adaptive 4D-CRNN on the raw epoch tensors
- Live EMOTIV SDK integration (replace DREAMER replay with real-time streaming)
- Longitudinal tracking - compare scans over time to detect trend changes
- Expand to DEAP and SEED-IV datasets for cross-dataset validation
Built With
- docker
- dreamer-dataset
- emotiv
- fastapi
- fastmcp
- fhir-r4
- google-adk
- joblib
- litellm
- matplotlib
- mne
- nginx
- numpy
- prompt-opinion
- pydantic
- python
- react-19
- react-three-fiber
- scikit-learn
- three.js
- typescript
- vite

Log in or sign up for Devpost to join the conversation.