-
-
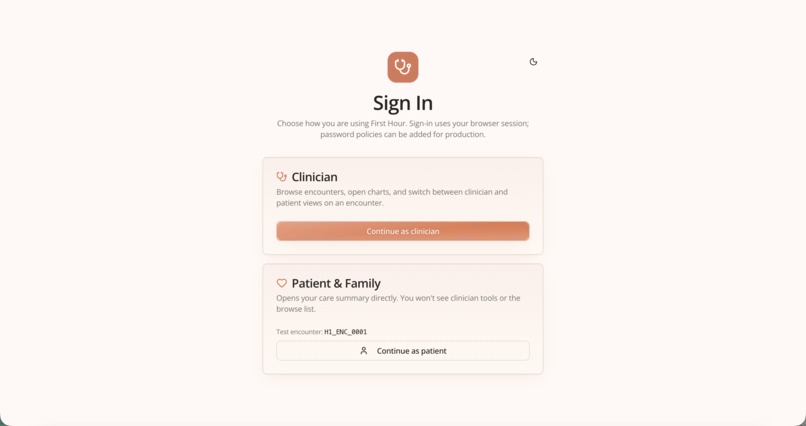
Login Page
-
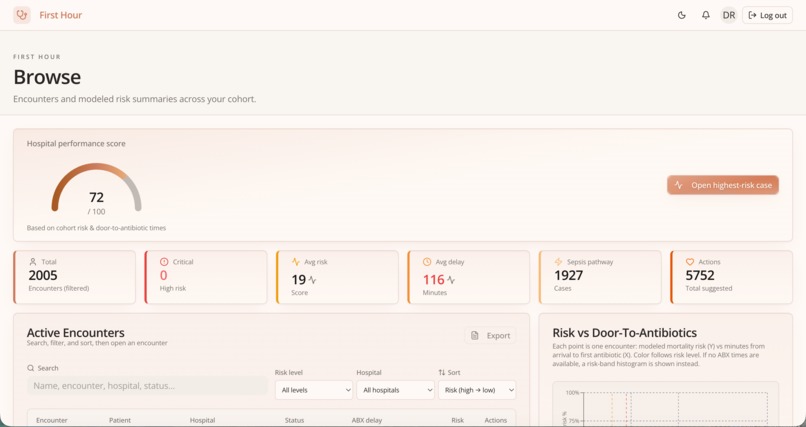
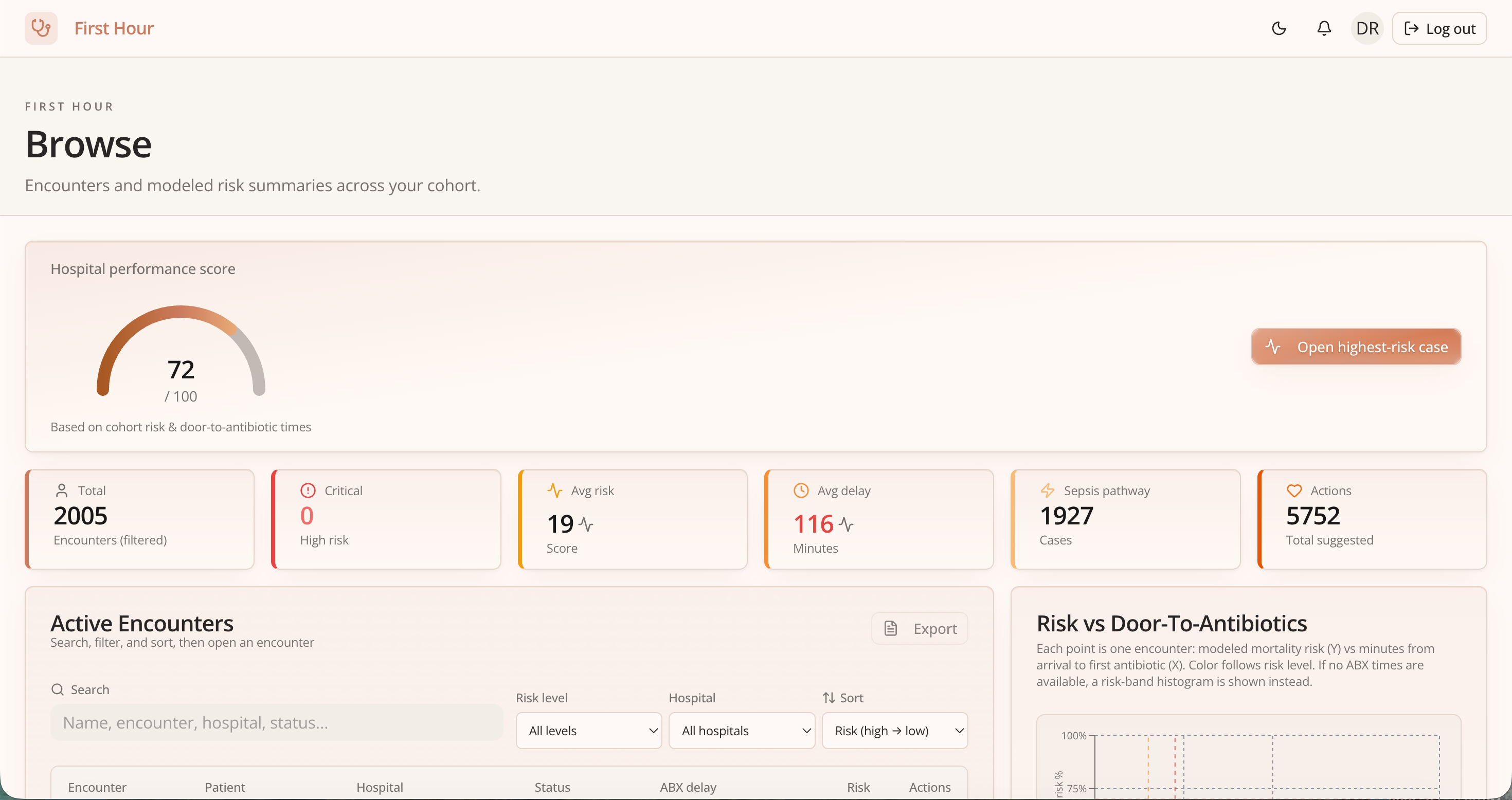
Overview Page
-
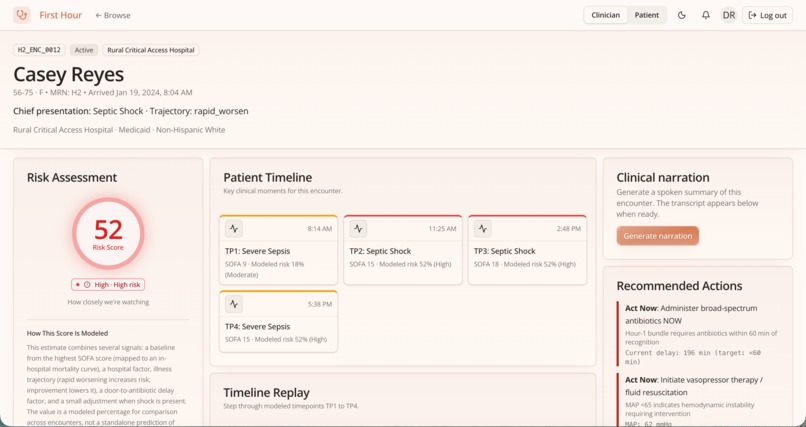
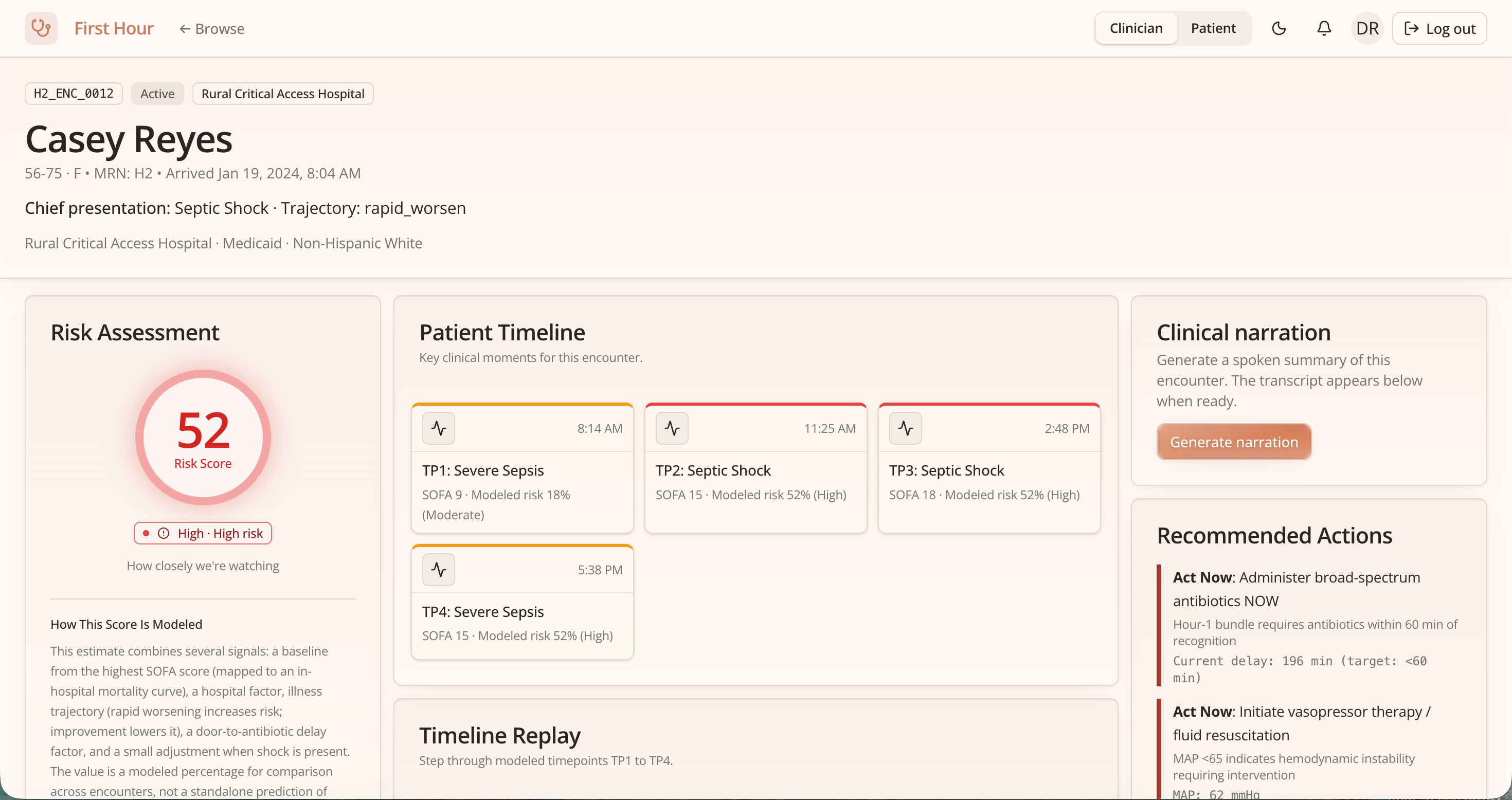
Clinician View
-
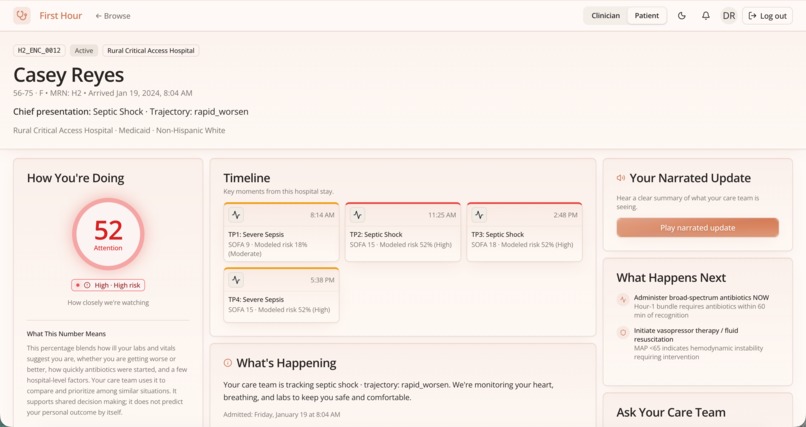
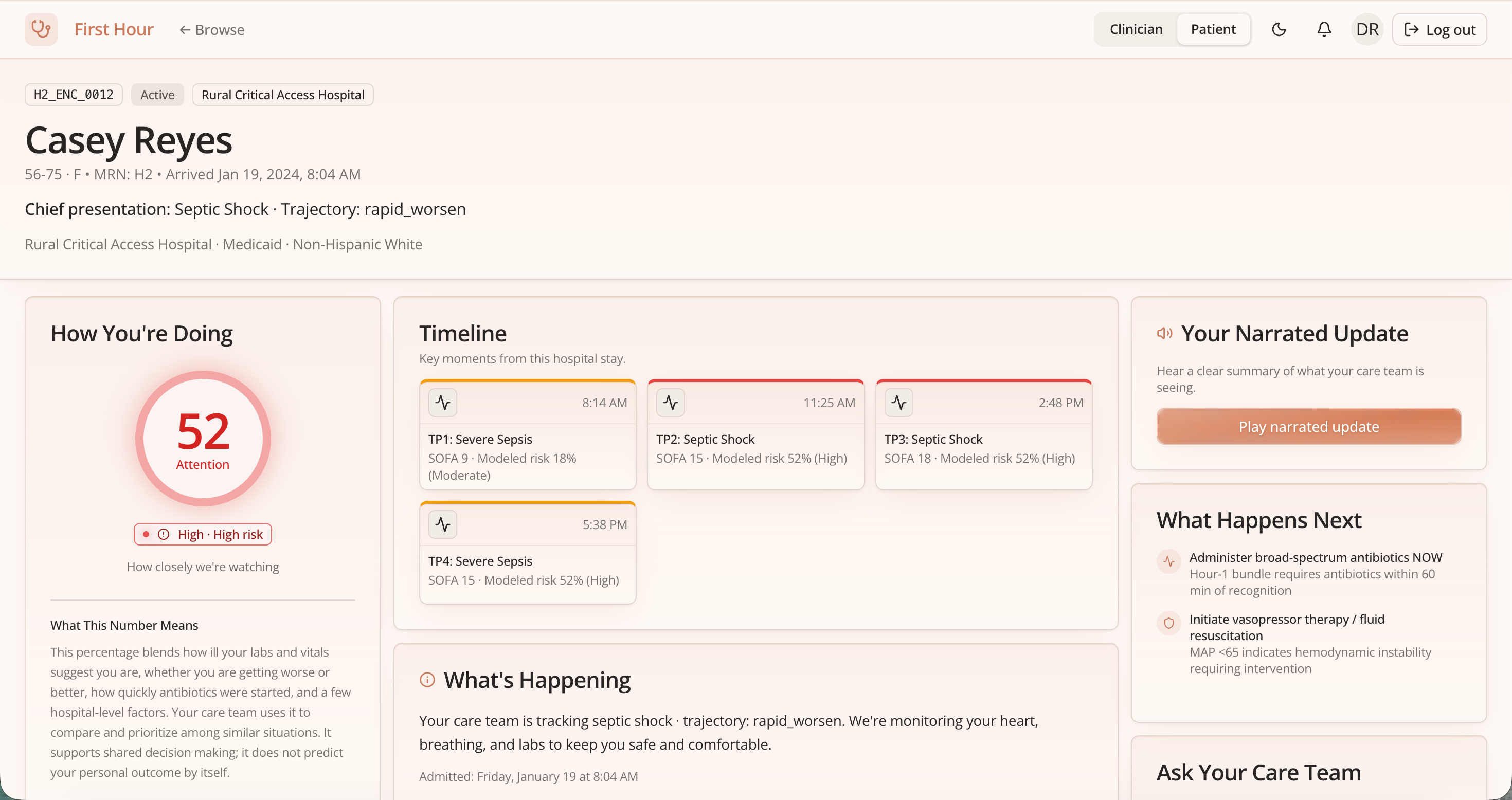
Patient View
About the project
Inspiration
Sepsis moves fast, but information often moves slowly—especially between the bedside team and families in a stressful ED stay. We were inspired by a simple idea: one encounter, two lenses. Clinicians need precision and action; patients and families need clarity, reassurance, and orientation without losing respect for how sick someone might be.
We also wanted transparency to be concrete, not decorative—who opened the care summary and an optional verifiable audit trail on Solana (devnet memos with no PHI on-chain).
What we learned
- Dual UX is a product choice: “Clinician” vs “Patient & family” is not a theme toggle—it changes language, density, and what we emphasize (risk vs comfort, jargon vs plain words).
- Generative AI is a narrator, not the scoreboard: LLM output explains and phrases modeled results; risk and trajectories come from explicit rules over structured fields (SOFA-related signals, timepoints TP1–TP4, bundle timings).
- Infrastructure is part of the demo: shipping with optional keys taught us to degrade gracefully—cache where it helps, fall back to sensible copy when APIs are offline, and keep Mongo/S3/Solana optional for judges who run locally.
- Web3 ops are real: devnet SOL, RPC limits, and faucet rate limits affect whether on-chain signatures appear—treating that as an operator concern, not magic.
We think of the rule-based risk R as a function of severity signals and timepoint features z_t: R ≈ f_rules(SOFA-like signals, z_t1, …, z_t4)
The LLM’s job is to describe R and trajectories in language matched to each audience—not to silently replace clinical logic.
Synthetic data generation
All patient rows come from our master synthetic sepsis generator (gen.py, v7): a reproducible pipeline (fixed global seed) that emits combined_sepsis_data_v7.csv—not real PHI. We simulate six hospital archetypes (academic, rural critical access, quaternary referral, safety-net urban, suburban community, for-profit regional) with archetype-specific ED volume, sepsis prevalence, payer mix, race/ethnicity, and comorbidity patterns. Each encounter draws clinical trajectories across modeled timepoints (TP1–TP4)—vitals, labs, SOFA-related inputs, sepsis severity, and care-process delays (e.g., recognition, door-to-antibiotics)—with v7 fixes for trajectory diversity (e.g., crash–recover beyond shock-only), weekend delay logic, and SOFA mortality calibration aligned to reference tables. The CSV is the single source the FastAPI backend loads for demos and risk/timeline computation.
How we built it
- Data & engine: Synthetic cohort (
combined_sepsis_data_v7.csv) → FastAPI services for encounters, computed risk, timelines, and recommended actions. - Frontend: React + Vite + Tailwind encounter dashboards—vitals and trajectory charts, timeline grids, patient/clinician layouts.
- Generative AI: Gemini for explanations (mode-specific tone), chat, simplified wording, and chart narration; ElevenLabs for spoken summaries; S3 for hosted audio when configured.
- Persistence: MongoDB Atlas (recently viewed, saved cases, access logs, caches), with an in-memory fallback for quick demos.
- Audit: Solana devnet memo transactions with non-PHI payloads and explorer-linked signatures when the signing wallet is funded.
Challenges
- Solana signatures without SOL: Memo transactions need fees; public RPC airdrops often hit HTTP 429. We added operator-facing wallet status, clearer hints, and a manual faucet path so signatures show up once devnet SOL lands.
- “Trustworthy tone”: Writing patient-facing language that is kind without being misleading, and clinician copy that is specific—iterated through separate modes and prompts.
- Scope under time pressure: We chose depth on one coherent encounter story over covering every sepsis edge case in the book.
Built With
- amazon-web-services
- base58
- css
- elevenlabs-api
- fastapi
- framer-motion
- google-gemini-api
- httpx
- javascript
- jsx
- lucide
- mongodb-atlas
- numpy
- pandas
- python
- radix-ui
- react
- react-router
- recharts
- solana-(devnet)
- solders
- tailwind-css
- uvicorn
- vite

Log in or sign up for Devpost to join the conversation.