-
-
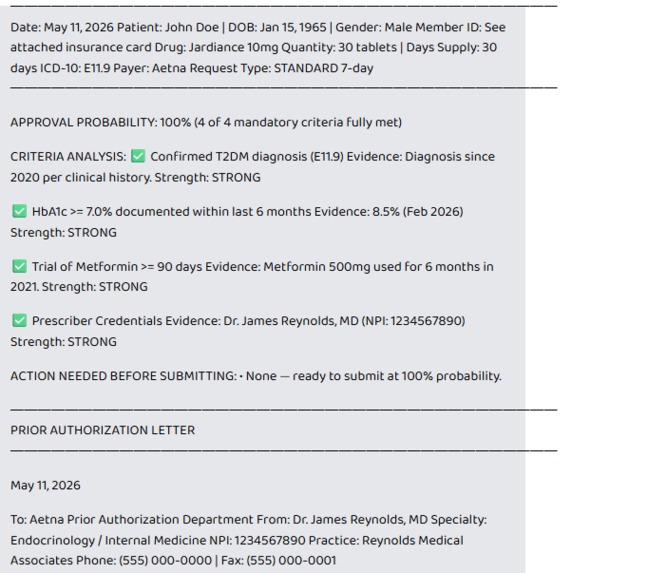
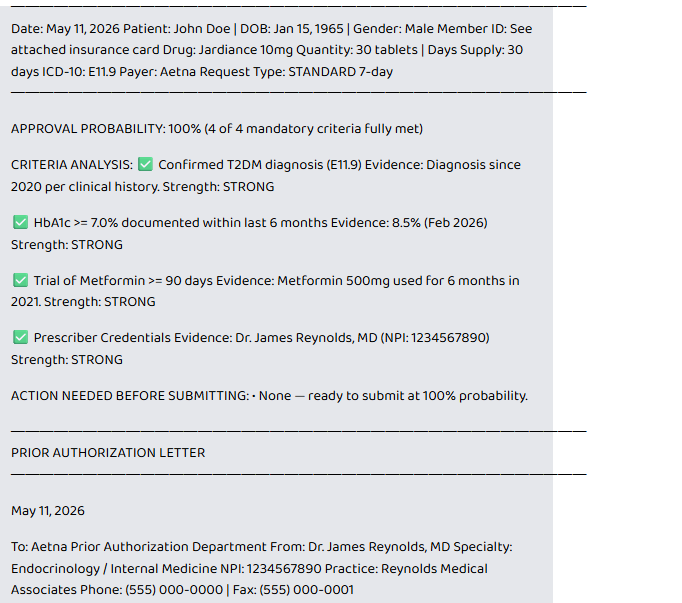
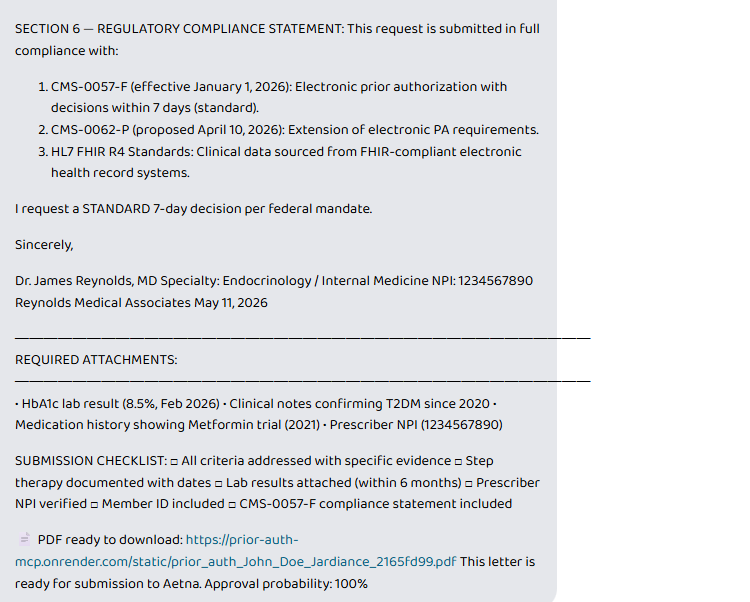
Agent Response
-
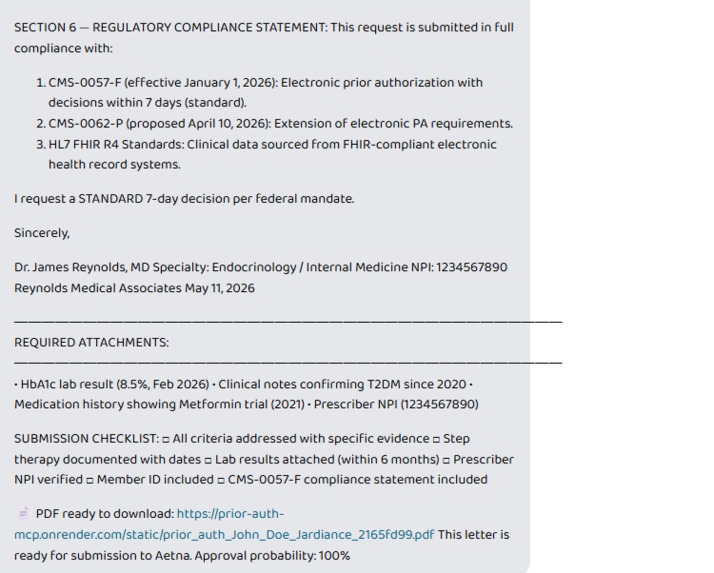
Pdf Download Link
-
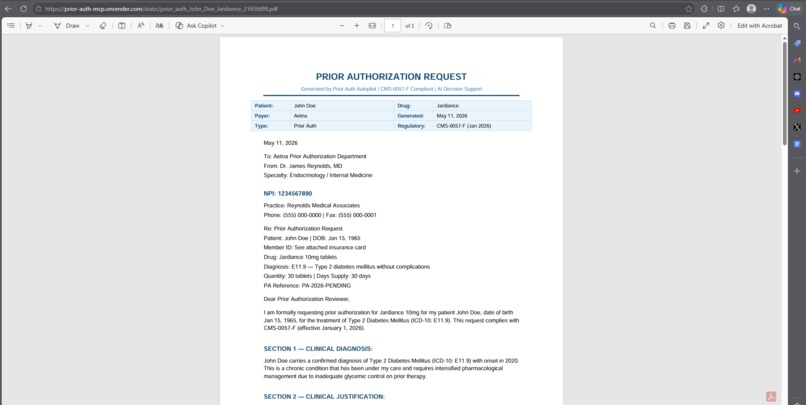
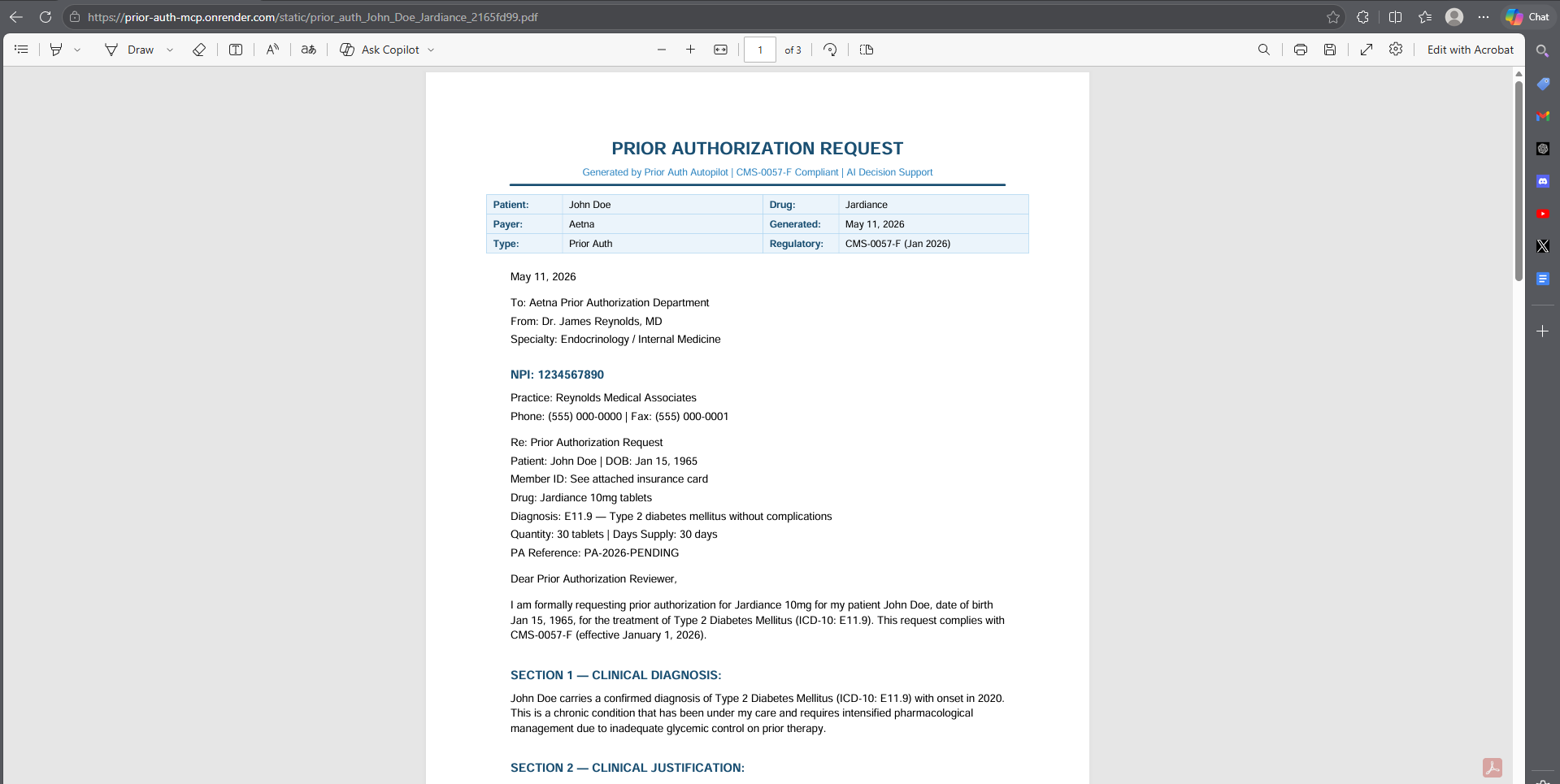
Generated PDF Screenshot
Inspiration
My mother waited 11 days for insulin approval while her blood sugar hit 400 mg/dL. The doctor's office faxed forms three times. The payer "lost" the first two. By day 8, she was in the ER.
This isn't rare — it's the norm. 93% of physicians report care delays due to prior authorization (AMA 2025 Survey). Doctors waste $34,000/year and 700+ hours per provider on PA paperwork. Patients sit at home, getting sicker, while paper shuffles between fax machines.
Then CMS-0057-F hit on January 1, 2026 — mandating electronic PA with 72-hour urgent decisions. But the government mandated speed without giving doctors any new tools. We thought: what if we could turn a 45-minute PA request into a 60-second conversation?
What it does
Prior Auth Autopilot is the first MCP-native clinical AI agent that generates submission-ready prior authorization letters — not drafts, not templates, not "fill in the blanks." Every field is complete. Every criterion is addressed. Every lab value is cited with dates.
The 60-Second Workflow:
- Doctor opens patient in Prompt Opinion
- Says: "I need prior auth for Ozempic through Aetna"
- Agent reads live FHIR data from the EHR automatically
- Fetches Aetna's exact criteria for Ozempic
- Runs a proactive gap check — "⚠️ HbA1c is 8 months old — Aetna requires within 6 months"
- Calculates approval probability: "78% — here's the breakdown"
- Generates a 6-section clinical letter with CMS-0057-F compliance
- Creates a downloadable PDF with color-coded criteria analysis
- If probability is low: auto-generates a peer-to-peer call script
Denial handling: Doctor pastes a denial letter → agent detects denial type → generates targeted appeal → cites regulatory grounds → produces PDF.
How we built it
- FastMCP server (Python) deployed on Render — matches Prompt Opinion's official
po-fastmcpreference architecture - MethodType-based FHIR extension for
ai.promptopinion/fhir-context— readsx-fhir-server-url,x-fhir-access-token, andx-patient-idheaders for real EHR integration - Dual-mode FHIR: automatically uses real EHR data from Prompt Opinion, falls back to HAPI FHIR R4 sandbox for demos — zero PHI
- ReportLab PDF engine with professional clinical formatting — color-coded criteria (✅🟡❌), structured sections, regulatory footer
- Starlette static file serving for PDF downloads alongside the MCP endpoint
- 19+ drug criteria database across 4 major payers with generic fallback
- 7 denial type classifiers — step therapy, medical necessity, missing docs, experimental, quantity limit, expired PA, non-formulary
- 6 MCP tools:
get_payer_criteria(),list_supported_drugs(),get_patient_fhir_data(),generate_prior_auth(),analyze_denial_letter(),generate_pdf_letter()
Challenges we ran into
- The Silent Deprecation: FastMCP v3.2.4 silently deprecated the
descriptionconstructor parameter. Server crashed on deploy with zero useful error message. Took hours of debugging to find a one-word fix. - The Lifespan Trap: Mounting FastMCP inside Starlette causes
RuntimeError: Task group is not initializedunless you passlifespanfrom the MCP app to Starlette — completely undocumented behavior. - The Capabilities Binding Bug: Our FHIR extension used
*args, **kwargswhich silently failed. We reverse-engineered Prompt Opinion's reference repo and discoveredMethodTypebinding with explicit parameters is required. - The Header Blindspot: Without reading
x-fhir-server-urlheaders, the agent always hit the HAPI sandbox instead of real EHR data. We discovered these headers only by reading PO's source code line by line.
Accomplishments that we're proud of
- 45 minutes → 60 seconds: A complete prior auth workflow that used to take nearly an hour now happens in one conversation turn
- Proactive gap detection: No other PA tool warns doctors about weak spots BEFORE submission. We calculate exactly what's missing and how it impacts approval odds
- Approval probability scoring: Quantified 0-100% with per-criterion breakdown — doctors see exactly where they're strong and where they need more evidence
- Peer-to-peer call scripts: When the letter isn't enough, we generate word-for-word scripts with anticipated objections and counter-arguments for the payer's medical director
- 100% submission-ready output: Zero placeholders, zero blanks, zero "fill this in later." Every letter is ready to fax or upload immediately
- Dual-mode FHIR: Seamlessly switches between real EHR data in production and HAPI sandbox for demos without changing a single line of code
- Full regulatory compliance: Every letter cites CMS-0057-F, CMS-0062-P, and 45 CFR 147.136 — we don't just generate letters, we arm doctors with federal regulations
What we learned
- Prior authorization isn't a technology problem — it's an automation gap. The clinical data exists in FHIR. The criteria exist in payer policies. Nobody connected them until now.
- Proactive gap detection is the killer feature. Doctors don't just want a letter — they want to know if it will get approved BEFORE they submit it.
- CMS-0057-F changed the legal landscape, but only tools like this make the mandate actually work for doctors on the ground.
- The MCP protocol is the perfect abstraction for clinical AI tools — it separates the intelligence (LLM) from the capabilities (FHIR queries, PDF generation, criteria lookup) cleanly.
What's next for Prior Auth Autopilot
- Live EHR pilot with a health system partner to measure real-world approval rate improvement
- Expand to 20+ payers with real-time formulary and benefit verification
- Auto-submission via payer FHIR APIs when CMS-0062-P finalizes
- Outcome learning — track which letter patterns, evidence combinations, and phrasings get approved, then continuously optimize
- Multi-language support — generate letters in Spanish for underserved patient populations
- Integration with pharmacy benefit managers for real-time formulary checks before writing the letter
Built With
- api
- fastmcp
- python
- render


Log in or sign up for Devpost to join the conversation.