-
-
-
-
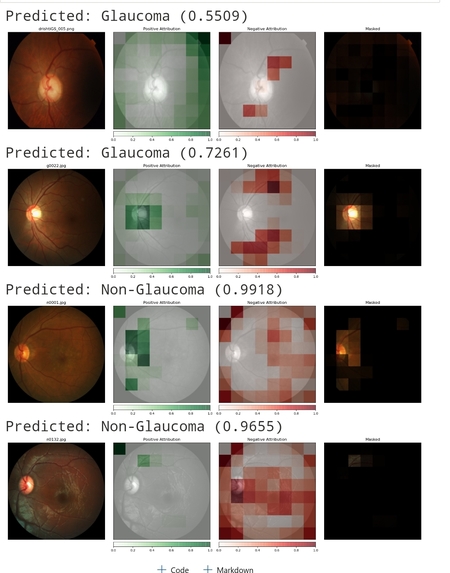
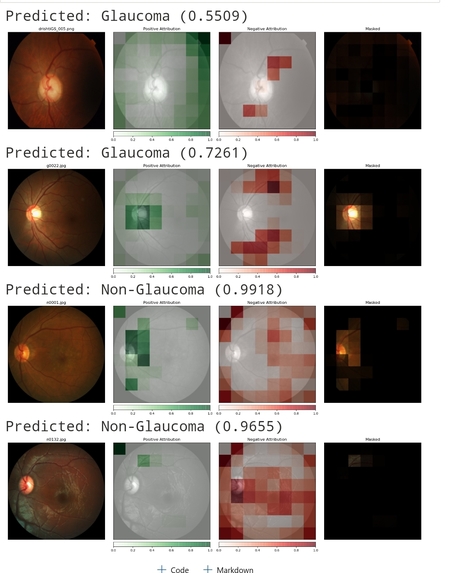
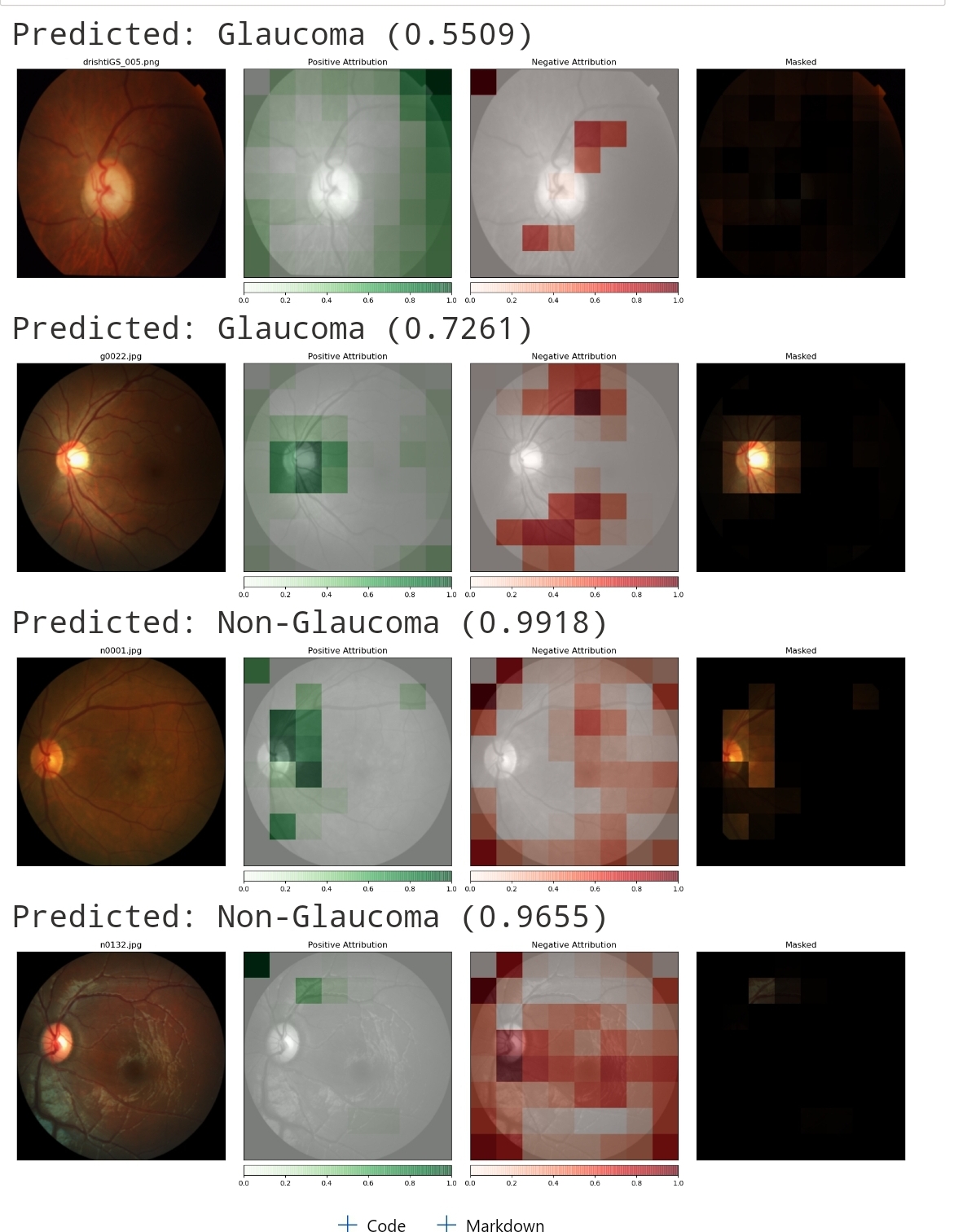
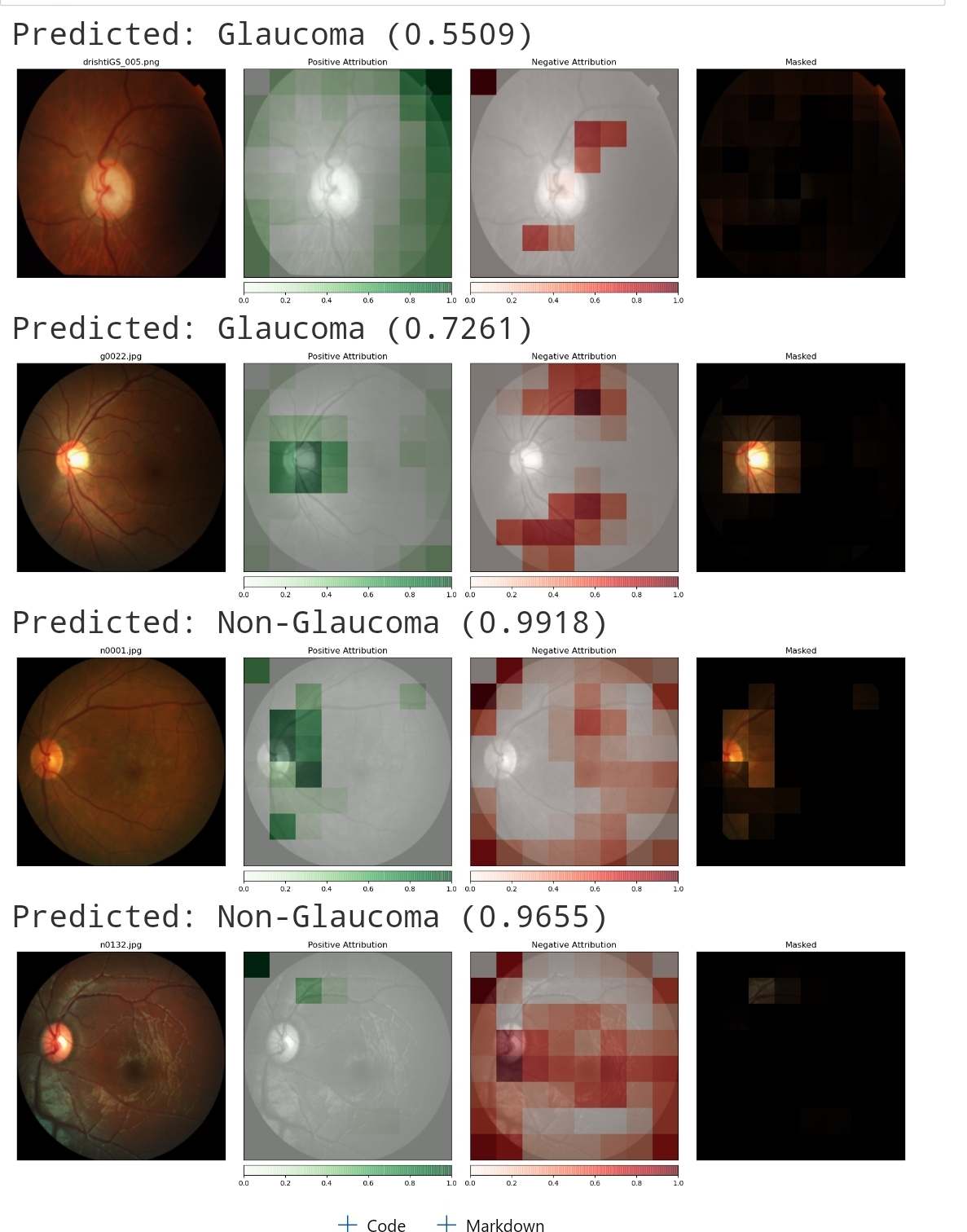
Predictions gallery
-
-
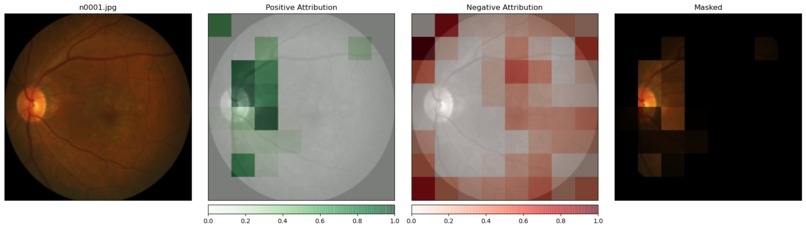
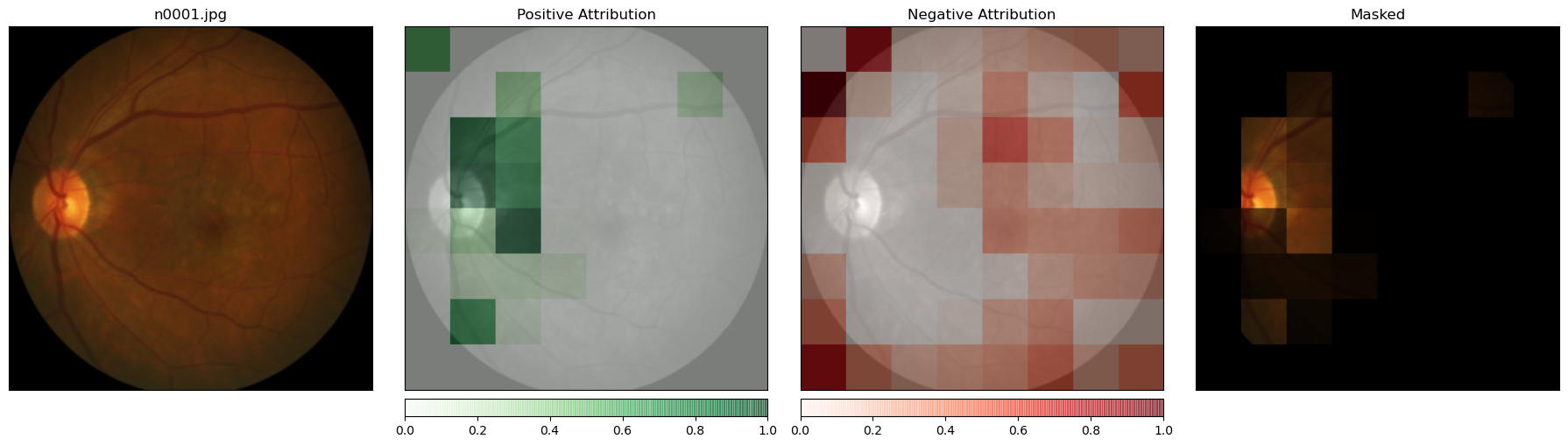
Class activation mapping
-
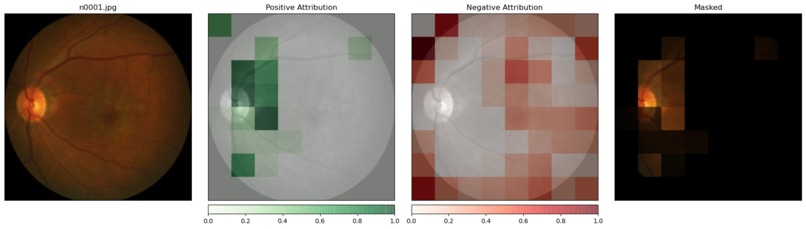
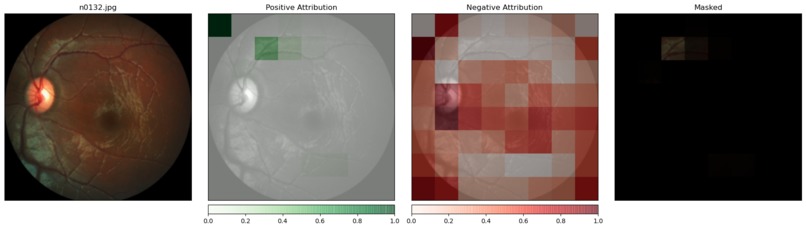
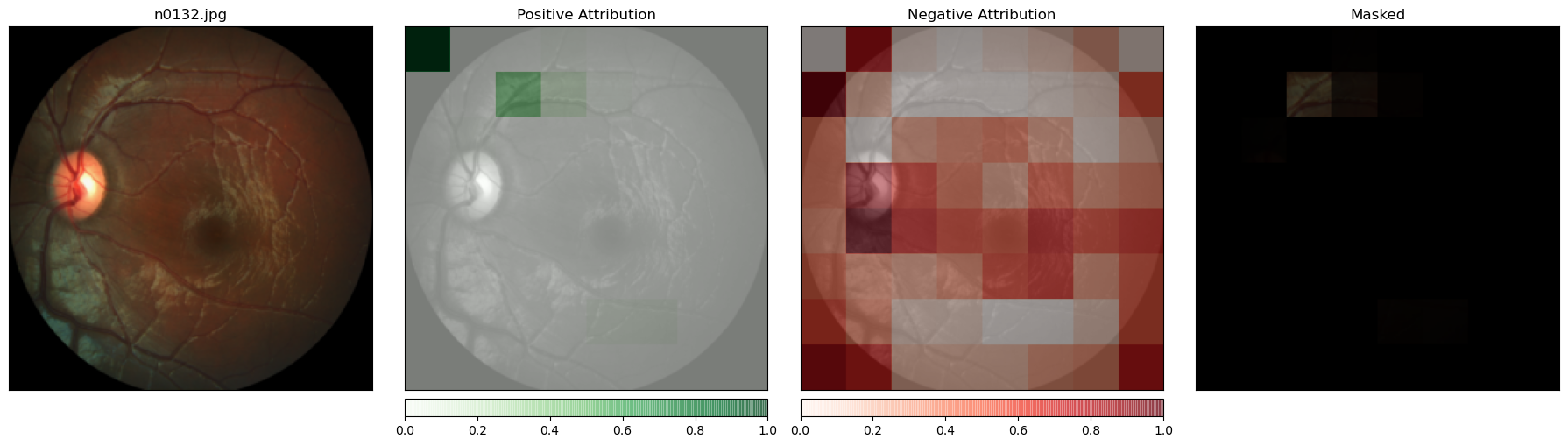
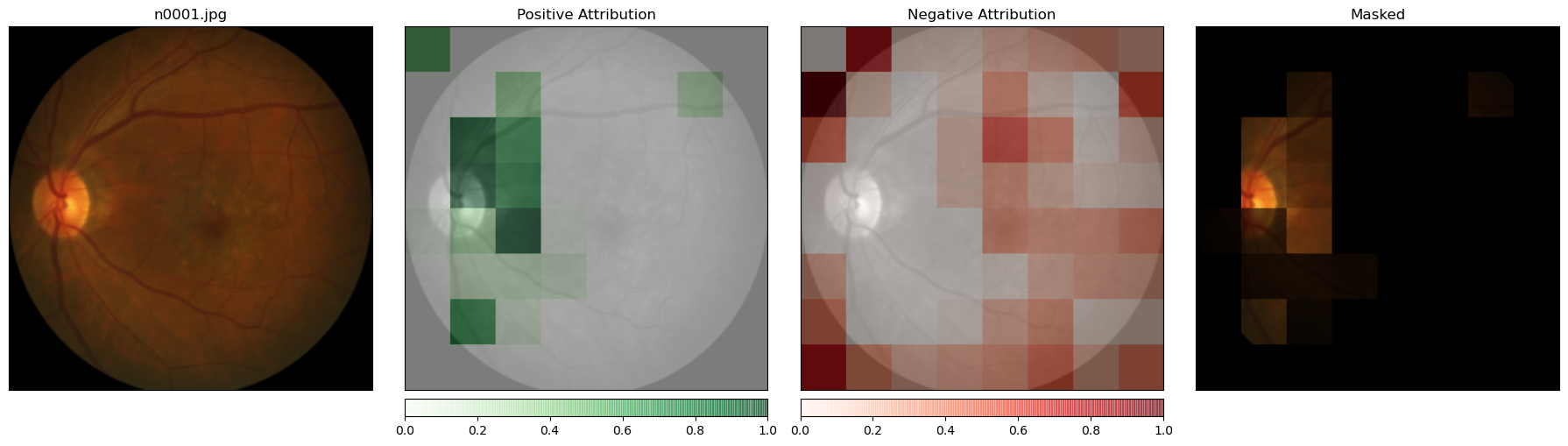
Positive and negative attributions
-
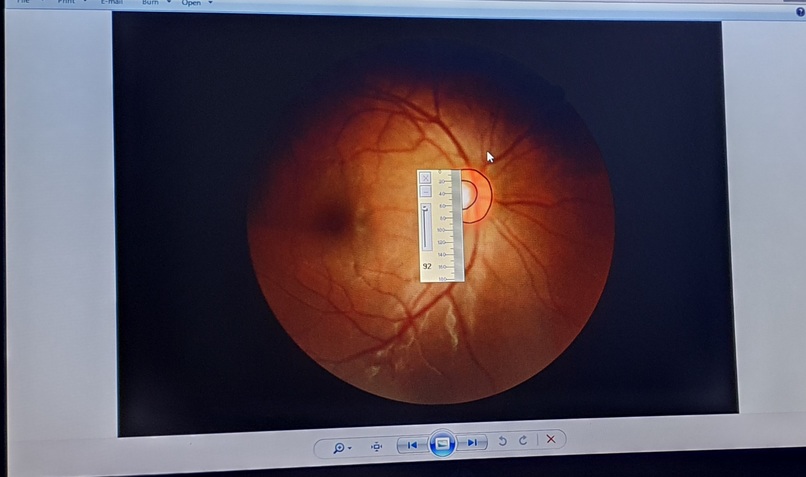
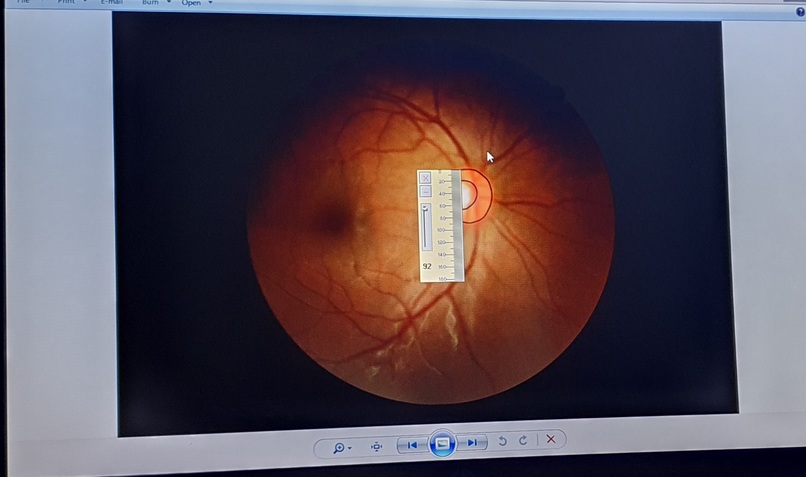
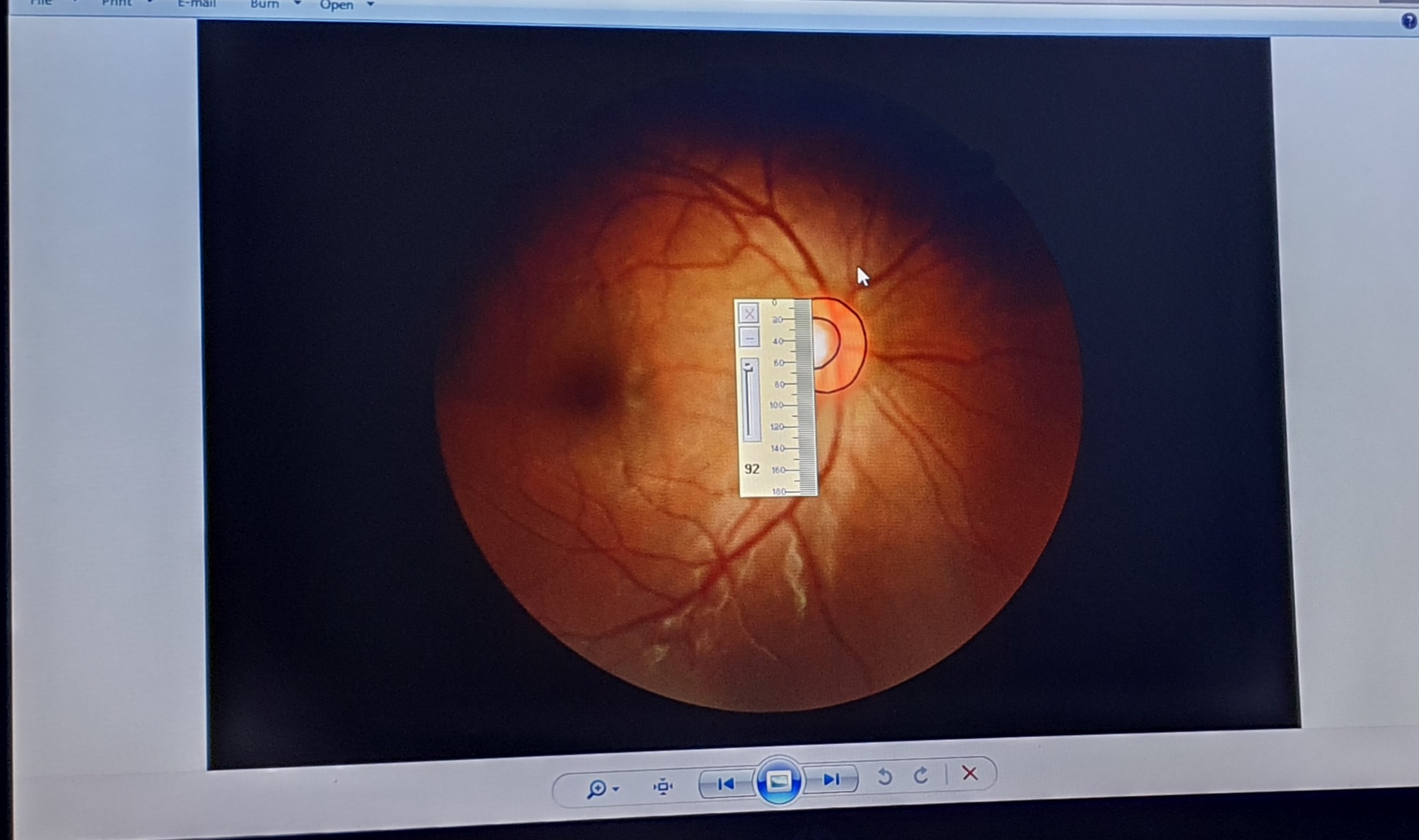
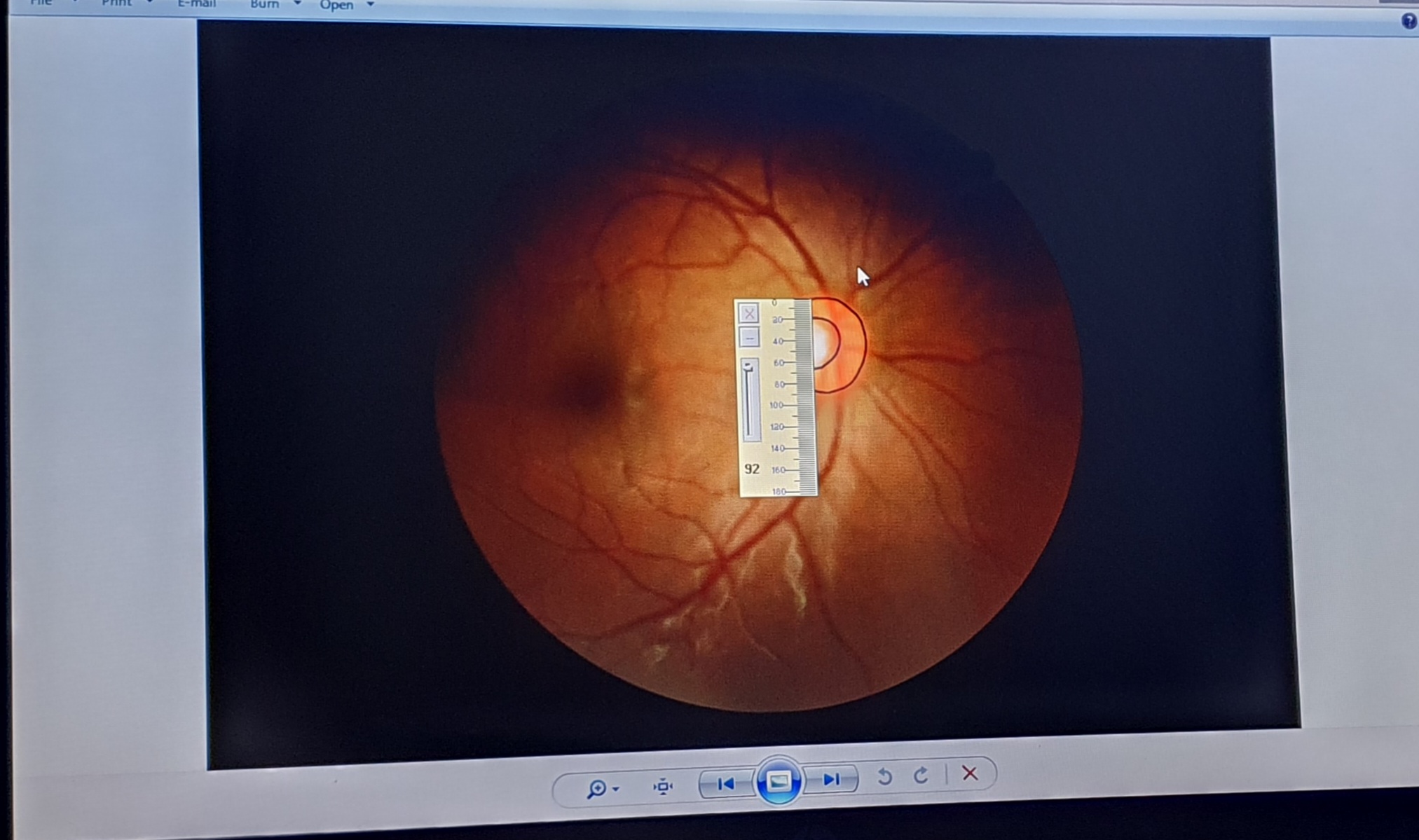
Cup to Disc Ratio and Image labelling
Inspiration
Primary Open Angle Glaucoma is one of the leading causes of irreversible blindness, globally. The situtation is worsened by the fact that Glaucoma does not present symptoms early, making the early detection necessary to stall its progression difficult. Inorder to detect this defect earlier, it is important for everyone to undergo routine eye examimation. However, this is difficult due to lack o qualified eye doctors or their uneven distribution. In Nigeria, there is a shocking statistic of eight ophthalmologists to one million people, and in Sub Saharan Africa, two ophthalmologists to one million people (Vanguard News Nigeria, 2021). This statistic is troubling. In addition, many eye diseases remain undiagnosed and untreated due to the high cost of examination and treatment.
To solve the accessibility and cost issues, many researchers have tried to develop computer assisted diagnosis approaches for Glaucoma detection, however, little to no progress has been made with regards to clinical translation and adoption. In addition, the past efforts involves a lot of preprocessing such as region of interest detection and cropping, channel extraction, etc, which places great demand on compute power and energy. Here, we propose a simple ResNet50 architecture and Azure Custom Vision Classifier for classifying Fundus images into glaucomatous and non-glaucomatous eyes.
What it does
The models can detect if an eye is glaucomatous when fed its fundus image. The ResNet model can provide a label for the image and the probability estimate whereas the Azure Custom Vision model will provide labels in addition to probabilities for both Glaucoma and Non-glaucoma.
How we built it
We finetuned a ResNet50 model by training the network on fundus images collected from O-RIGA, REFUGE, and the Dhrishti dataset. In addition, for the custom vision model, we used smart tagging to quickly create bounding boxes on the disc region. Since, the primary discriminating feature between a Glaucomatous and Non-Glaucomatous image is the Optic Disc central tissue loss symptomized by an increasing Optic Cup to Disc ratio, we observed that we could improve the performance of the classification algorithm if the region of interest (i.e. Disc region) in the training images are appropriately marked prior to training.
Challenges we ran into
- Data collection was a serious hassle
- Labeling: some of the data were without label, hence, we had to manually compute the cup to disc ratio of some of the images and provide a label based on criteria specified in Li et al 2018 where referrable (or suspect) cases are defined as having Vertical Cup to Disc Ratio (VCDR) between 0.7 and 0.9. I.e. 0.7 ≤ VCDR < 0.9, and certain glaucoma iff VCDR ≥ 0.9.
Accomplishments that we're proud of
Ability to use Azure custom vision for some parts of the project. The no-code platform is very accessible.
What we learned
Apart from disc cupping, damage to retinal blood vessels is another symptom of the incidence of glaucoma – this was shown by some of the positive attributions in the class activation mapping outputs. Also, cupping or rim thinnning is more apparent in upper or lower temporal sides of optic disc in early stages of glaucoma.
What's next for AI-EYE DOCTOR
Deployment, Devops and Prediction service. We are also looking to carry out user testing first and using the feedback to improve the product. For now, we have reached out to the ophhamologists of some hospitals includping MetroEyes in Nigeria. We are looking to conduct in-person and remote interviews to understand how the product will ease their work by automating some tasks. We propose that the product will be very useful in the pre-screening stage of patient engagement.


Log in or sign up for Devpost to join the conversation.