-
-
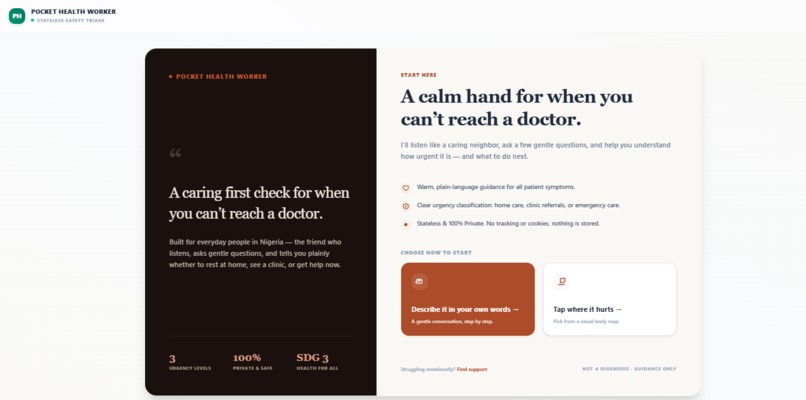
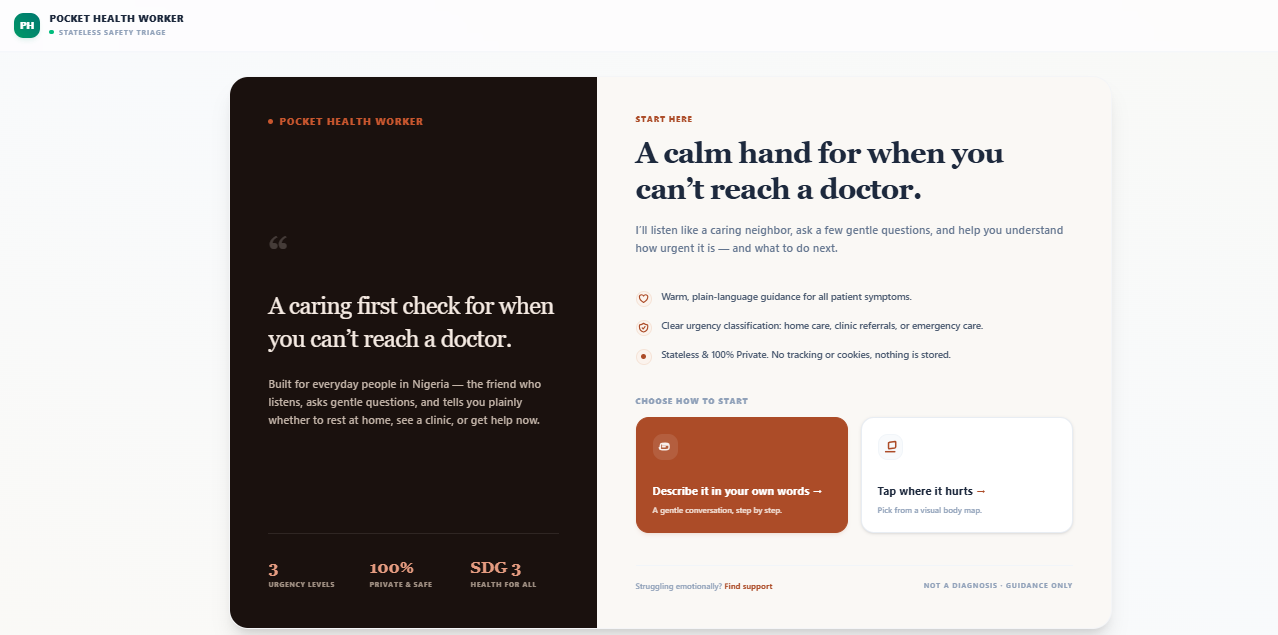
the landing page
-
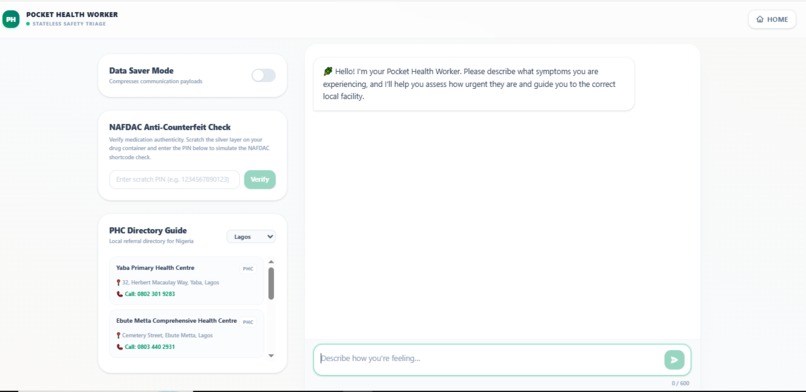
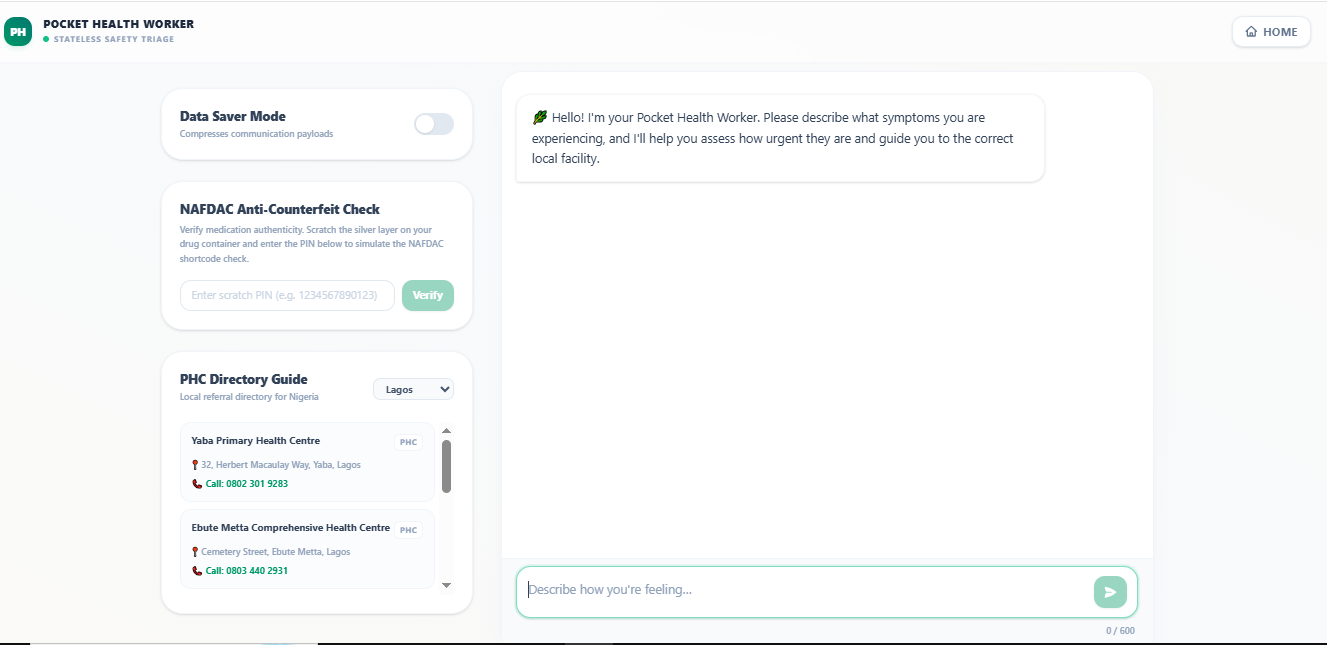
Symptom-triage chat with Nigeria's care toolkit built in — drug verification, Data Saver, and an offline clinic directory.
-
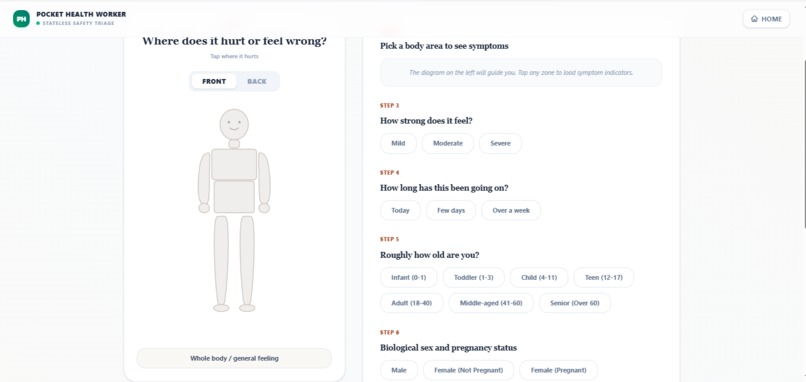
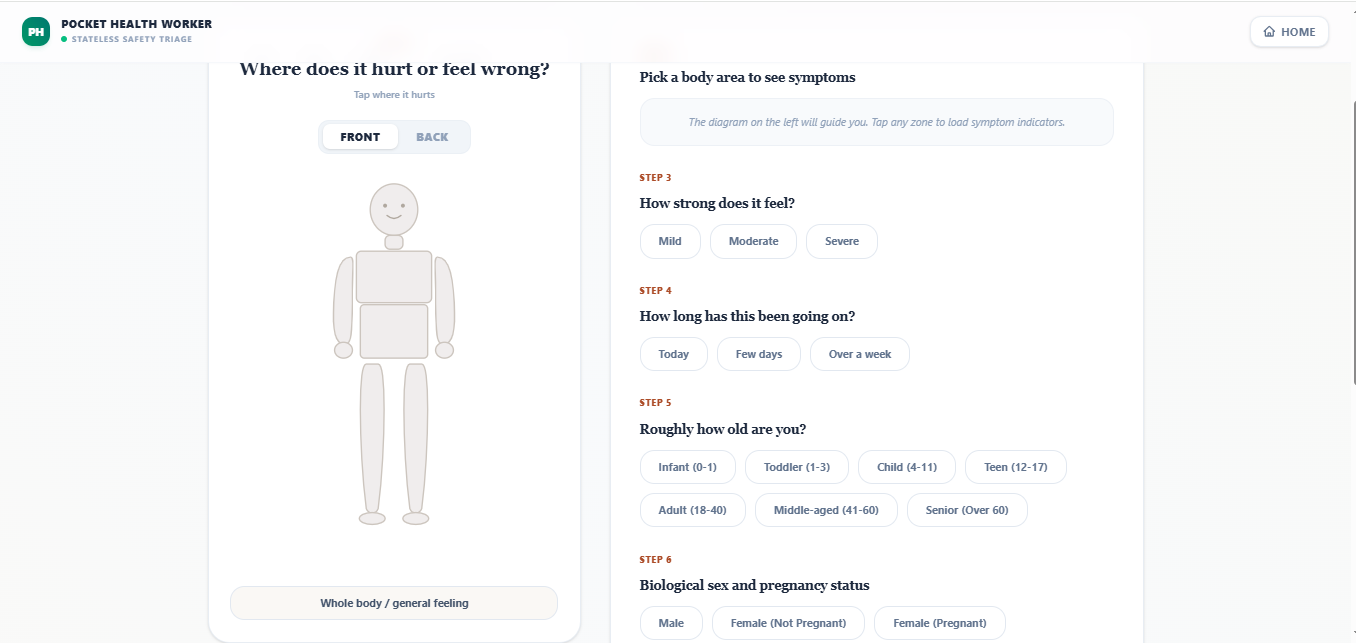
Tap where it hurts body map that questions on severity, duration, age, and pregnancy accessible triage that runs even offline.
-
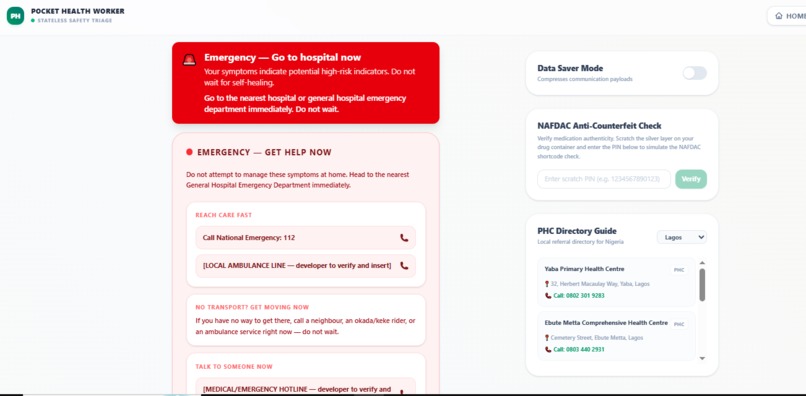
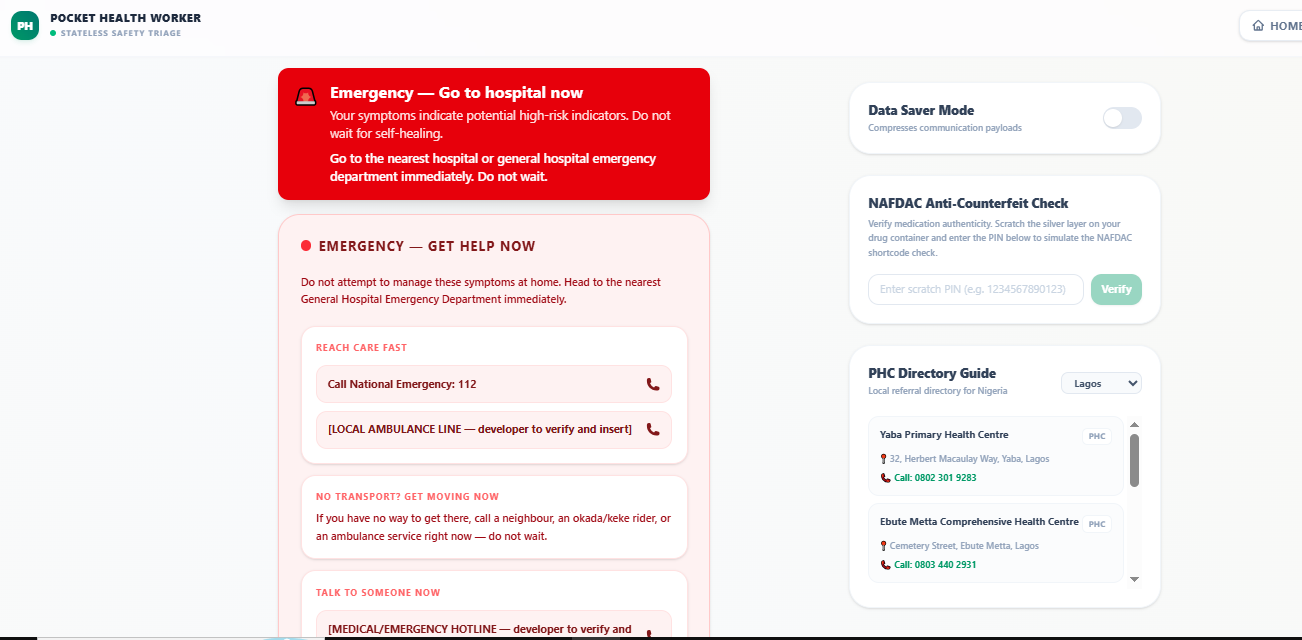
Emergency mode — when high-risk symptoms are detected, the app stops triage and routes the user straight to care:
💡 Inspiration
In Nigeria, there is roughly one doctor for every few thousand people, most of them concentrated in big cities. So when someone falls sick — especially at night, or far from a hospital — the first stop is rarely a doctor. It's a chemist's counter, a WhatsApp message, a neighbour's advice, or simply waiting and hoping.
The most dangerous moment is the uncertainty: "Is this something I can manage at home, or do I need to get to a hospital right now?" A mother whose baby spikes a fever at 2 AM doesn't need a diagnosis — she needs to know how urgently to act, and where to go. Getting that judgement wrong, in either direction, costs lives.
Pocket Health Worker was built for that moment. It doesn't try to replace a doctor — it's a calm, careful first step that helps people understand how urgently they need real care and connects them to it. This directly serves UN SDG 3 (Good Health and Well-being) by closing the deadly "last-mile" gap in access to health guidance.
🩺 What it does
You describe your symptoms — by typing, or by tapping an interactive 14-region body map (with inputs for age, severity, duration, pregnancy, and existing conditions). Pocket Health Worker reasons like a careful health worker, asks a few clarifying questions, and returns a clear urgency level:
- 🟢 GREEN — likely safe to manage at home, with advice
- 🟡 YELLOW — see a clinic soon
- 🔴 RED — emergency, get to care now
…along with next steps localized to Nigeria. Crucially, it never diagnoses or prescribes — it guides you toward real care.
⚙️ How it works
Most AI health tools have two fatal flaws: they hallucinate, and they break completely without internet. We designed Pocket Health Worker to confront both head-on.
A dual-engine architecture:
- Online, it uses Google Gemini, tightly constrained by strict safety prompts, for nuanced triage.
- Offline, it runs as a Progressive Web App with an in-browser deterministic rules engine — so even with zero mobile data, the body map still works, emergencies are still caught, and a cached directory of clinics is still available.
Three hardcoded safety layers that override the AI:
- A self-harm crisis interceptor — if it detects crisis language, it bypasses the AI entirely and surfaces verified Nigerian crisis lines (MANI and SURPIN) with one-tap calling.
- A deterministic red-flag catcher — danger signs like chest pain, difficulty breathing, or infant warning signs are caught locally and routed straight to an Emergency Bridge with the nearest facility and emergency numbers — no waiting on the AI.
- Conservative urgency-rounding — when in doubt, the engine always rounds up toward caution.
Built for the Nigerian reality:
- A NAFDAC counterfeit-drug check based on the official SMS verification flow, for a country with a serious fake-drug problem.
- A Data Saver mode that trims network payloads for spotty MTN/Glo/Airtel connections.
- An offline Primary Health Centre directory across 12 states, with tap-to-call numbers.
Privacy by design: the app is 100% stateless — no database, no accounts, no stored chat history. When you close the tab, your medical data is gone.
Tech stack: Next.js 16.2.6, React 19, TypeScript, Tailwind CSS, the Google GenAI SDK (Gemini), and a custom service worker for offline support.
🧗 Challenges we ran into
The hard part of a medical AI isn't the AI — it's everything you build around it to make it safe. The biggest challenge was guaranteeing the app could never give dangerous advice: that meant moving life-or-death decisions (emergencies, crisis situations) out of the AI's hands and into deterministic, hardcoded logic that runs first and overrides everything. Making triage work offline — with a conservative rules engine and reliable caching — was the second hard problem. And insisting on real, verified data (actual crisis-line numbers, real facility info) instead of anything the AI might invent took discipline, but it's the difference between a demo and something a real person could trust.
📚 What we learned
We learned that safety and honesty are design constraints, not afterthoughts — and that the most responsible thing an AI health tool can do is know its limits, refuse to diagnose, and route people to real human care. We also learned to design for the actual environment our users live in: limited data, high costs, counterfeit drugs, and long distances to care.
🚀 What's next
- USSD/SMS access so even feature-phone users can triage without a smartphone.
- Multilingual voice triage (English, Pidgin, Yoruba, Hausa, Igbo).
- Reviewing the triage logic against published clinical guidelines (e.g. WHO IMCI) together with practising clinicians.
Built With
- css3
- google-gemini
- html5
- javascript
- next.js
- progressive-web-app
- react
- service-workers
- tailwindcss
- typescript

Log in or sign up for Devpost to join the conversation.