-
-
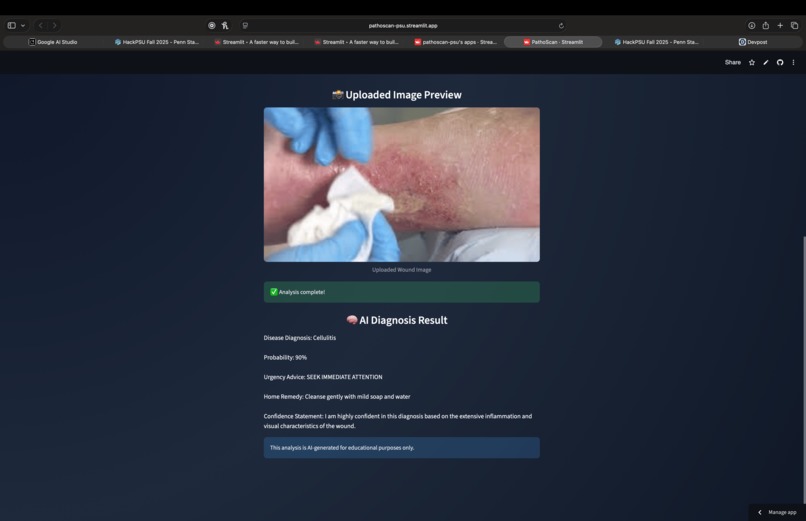
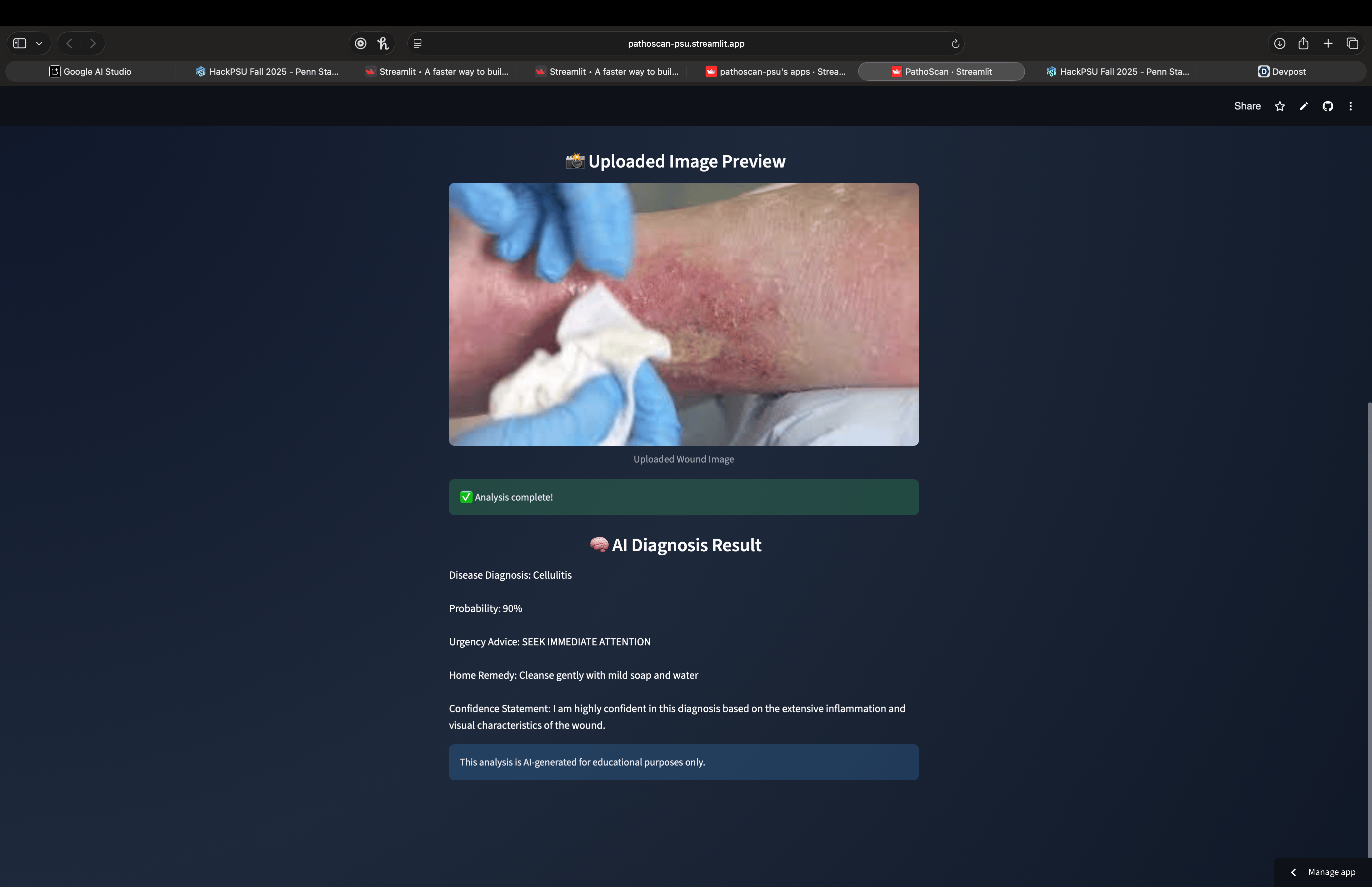
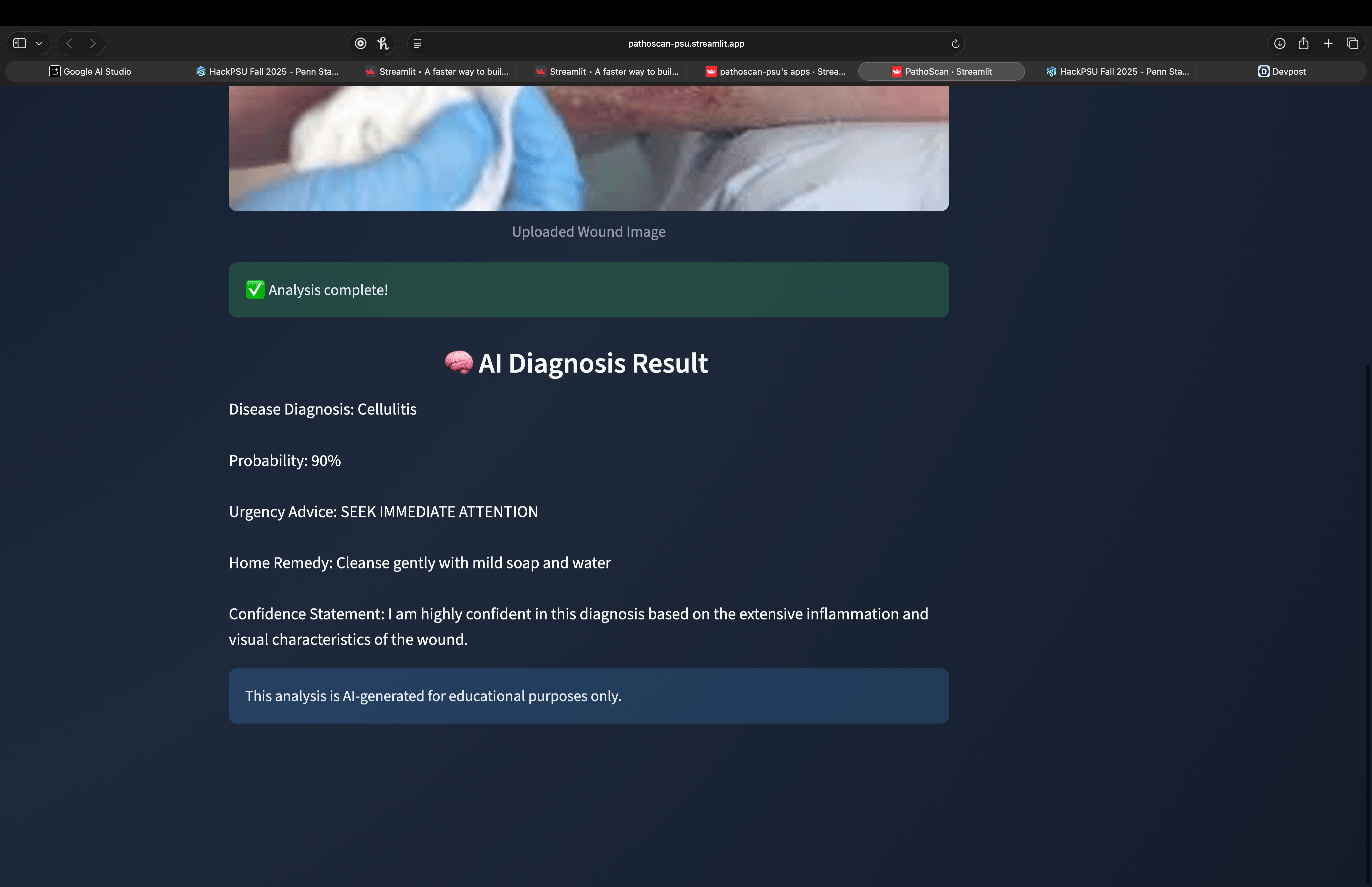
AI diagnosis of seeking immediate attention
-
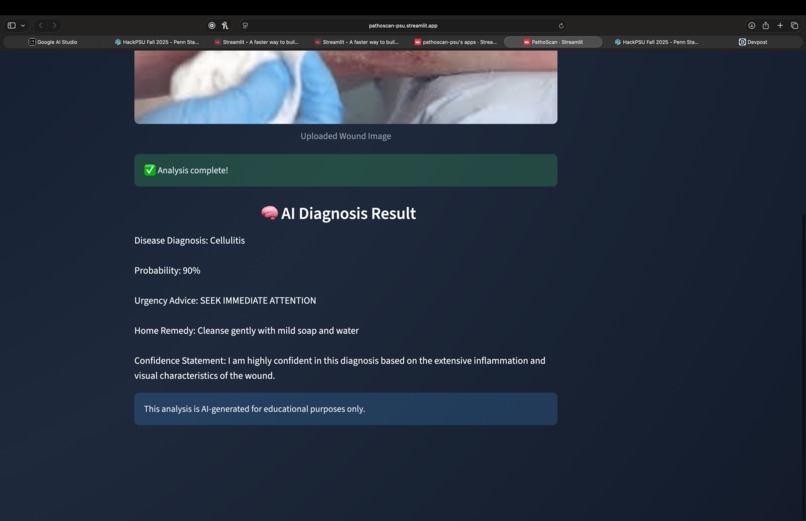
AI diagnosis of seeking immediate attention
-
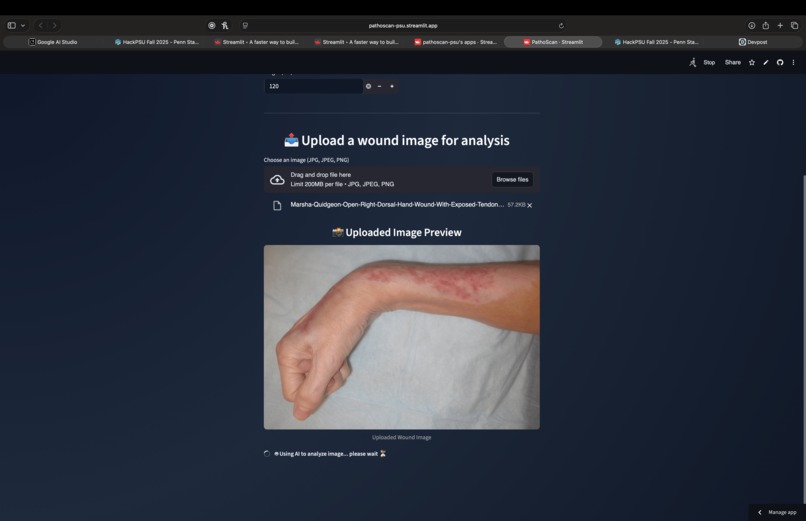
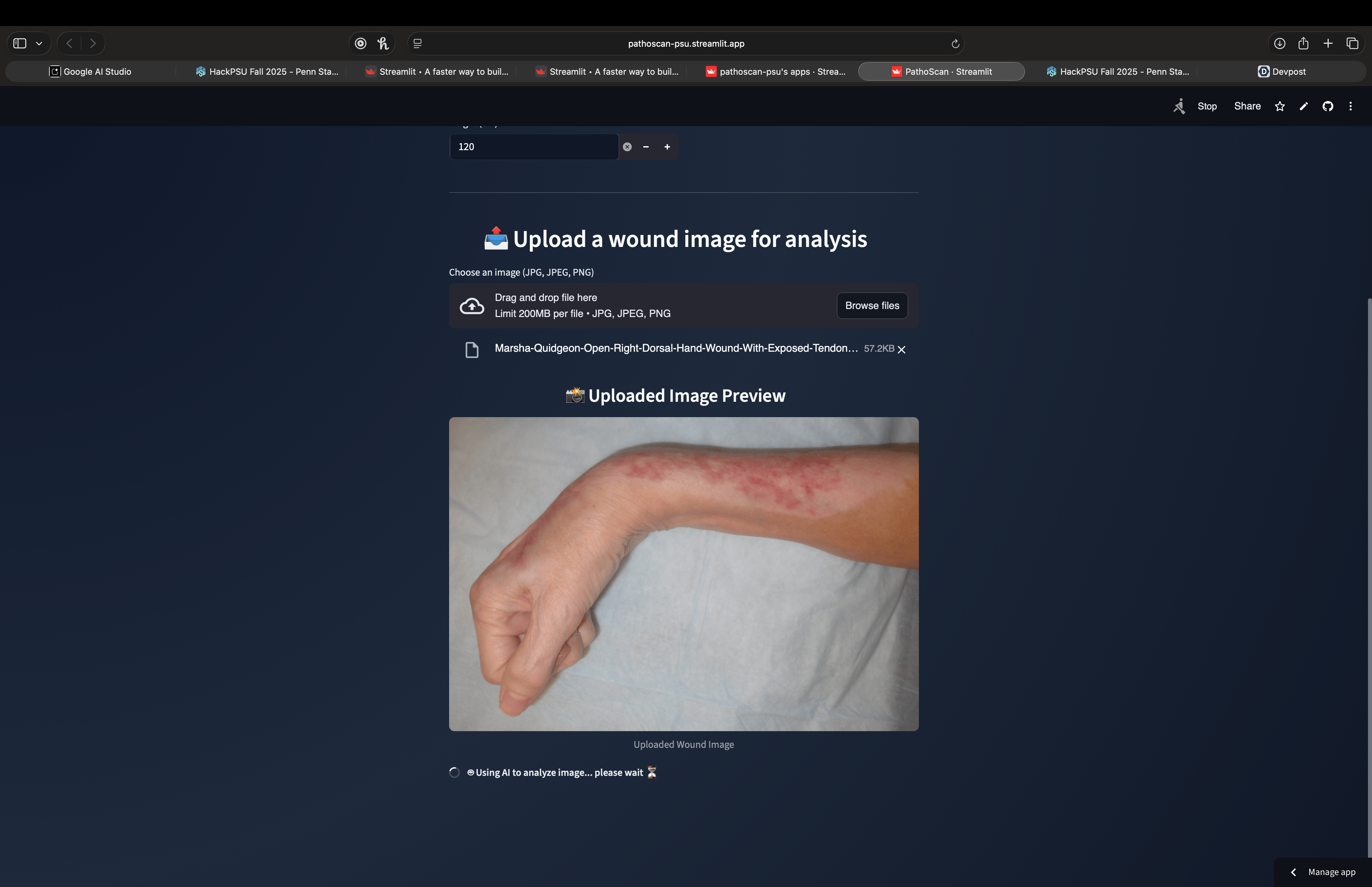
analysis of the infection
-
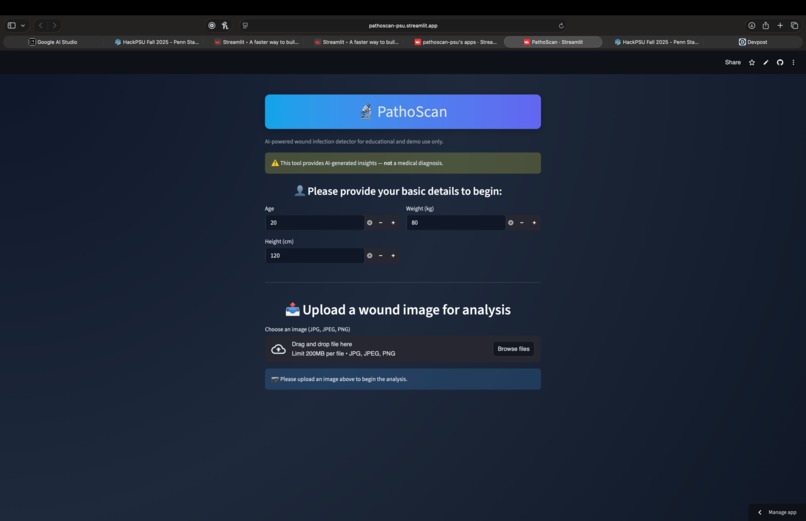
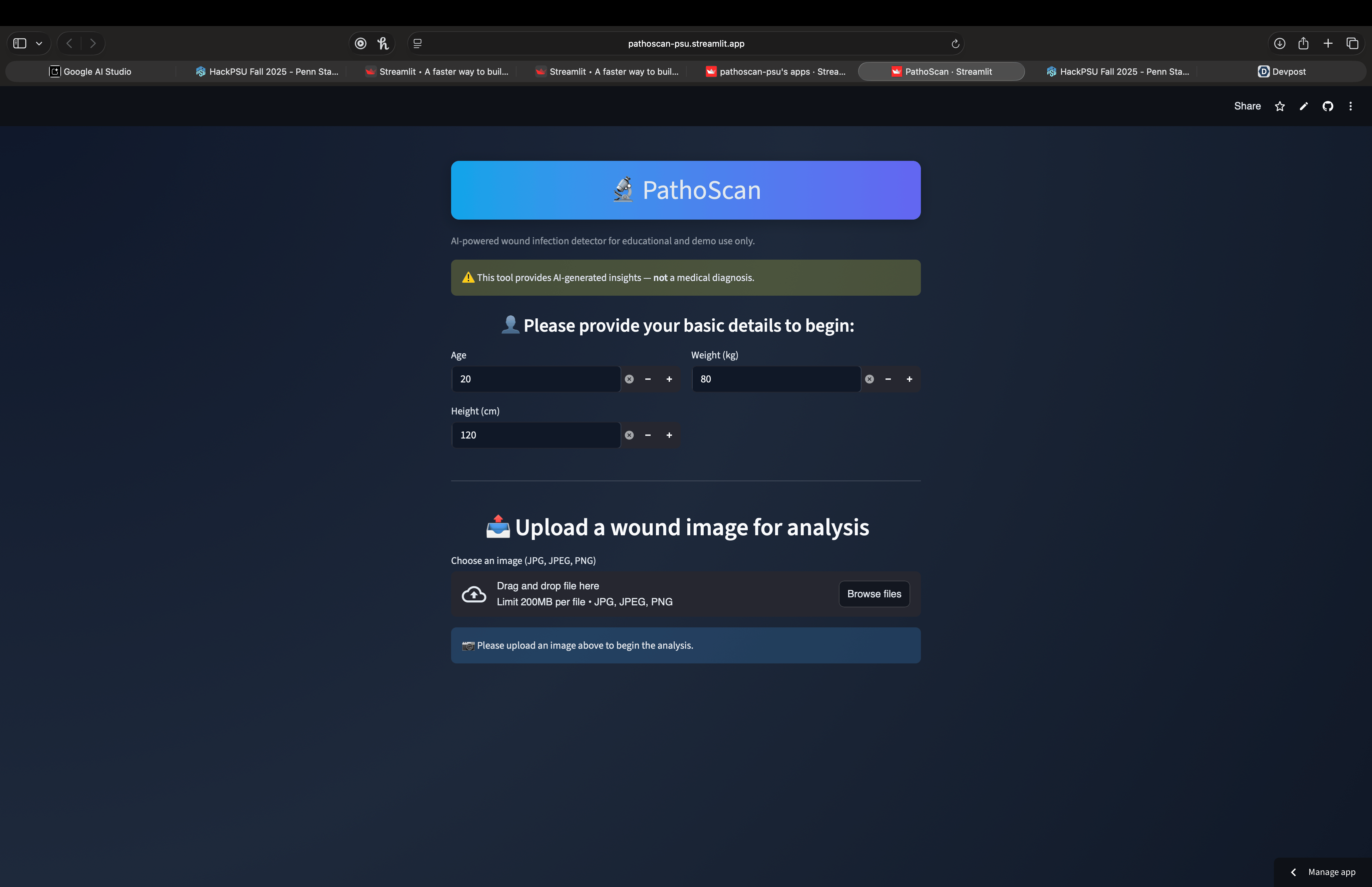
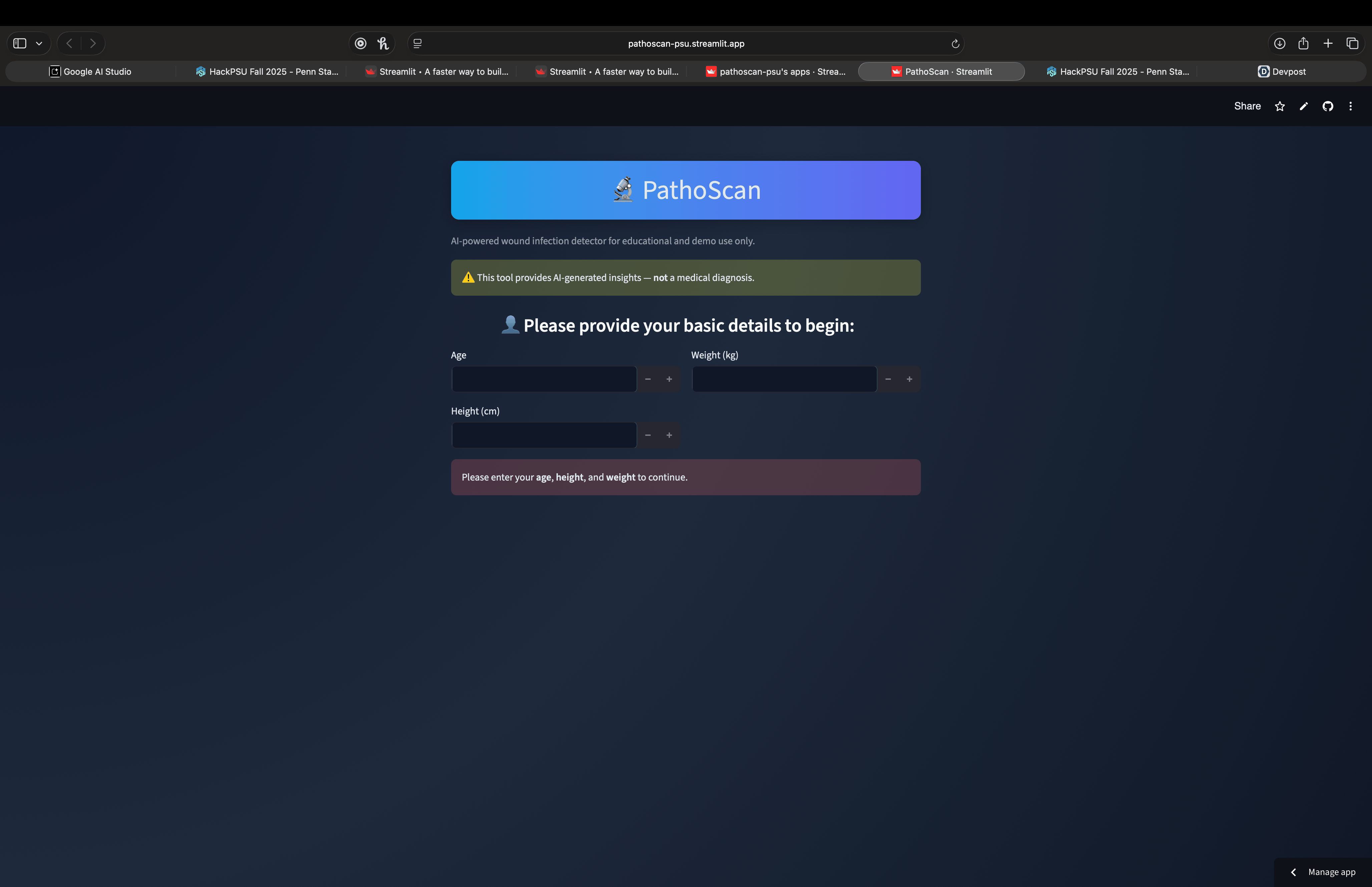
required vitals taken
-
landing page
PathoScan — early Infection warnings for people who wait too long to seek care
Why this is so Important and Impactful: Every year, millions of people hesitate to go to the hospital for wounds and infections—because of cost, stigma, shyness, long waits, or fear of the system. Many infections are underdiagnosed until it’s too late, leading to avoidable hospitalizations, amputations, or even death. We built PathoScan to offer a , fast and private nudge toward earlier care—so fewer “small problems” turn into life‑altering emergencies. We believe a simple, trusted prompt at the right moment can change behavior at scale. Even if we get to 10% of the population, we have a potential to save 200,000+ people with our early diagnosis system.
The problem we’re tackling
- Delay is deadly. A small wound today can become a severe infection in days. For many, the first “symptom” isn’t pain—it’s avoidance.
- Barriers stack. Cost, anxiety, stigma, transportation, and time all discourage visits. People often say, “I thought it was nothing.”
- Hidden consequences. Late care increases the odds of systemic infection and limb damage; we’ve all heard too many stories of unnecessary amputations that started as “just a cut.”
- Access is already in your pocket. Smartphones are everywhere—so early, private guidance can meet people where they are.
Our intention: PathoScan is not a diagnosis. It’s a compassionate, private, early warning to encourage timely care—especially for people who are shy, stigmatized, poor, uninsured, or scared of the medical system.
What inspired us
We kept meeting versions of the same story: a loved one or neighbor kept waiting—one more night—until a simple wound became something far worse. We wanted to make the easiest possible step: take a photo, get a clear signal, act earlier. No forms, no pressure, no judgment.
What we built
- A mobile‑first wound image checker that returns a strict five‑line summary: likely condition, probability, urgency, one short self‑care tip (if appropriate), and a confidence note.
- Stigma‑aware copy that avoids shaming and emphasizes clear next steps.
- Privacy by default: age/height/weight are collected locally to personalize the experience and are not sent to the vision model.
How we built it
- Interface: Streamlit with a modern, high‑contrast dark UI for readability and trust.
- Vision prototype: Multimodal image analysis prompted to produce auditable, plain‑text outputs.
- Reliability: On‑upload image downscaling, timeouts, and retries to avoid cloud latency spikes.
- Safety rails: Consistent “not medical advice” wording and conservative urgency prompts.
What we learned
- Trust beats cleverness. People need clarity and empathy more than dazzling UI.
- Friction kills follow‑through. One screen, one upload, one answer works.
- Bias is everywhere. We must train/validate on diverse skin tones, ages, and comorbidities.
- Public‑health alignment matters. Language should encourage earlier care, not self‑treatment in risky cases.
Challenges we faced
- Ambiguous photos: lighting/distance/occlusion can flip a prediction.
- Latency: some cloud calls hang—compression + retries stabilized real‑world use.
- Scope creep: we refused to over‑promise. PathoScan remains an educational nudge, not a diagnostic device.
- Ethics: false reassurance is dangerous—we bias toward “seek care” when risk signals stack.
Impact we’re aiming for
- Convert hesitation into earlier evaluation, especially for people delaying care because of cost, stigma, fear, or logistics.
- Help reduce severe infections and a slice of preventable amputations by prompting faster escalation when wounds look worrisome.
- Make equitable support the default by putting early guidance on the phones people already use.
We know this is ambitious—and that’s the point.
How can we expand onto this?
- Train a dedicated wound model (e.g., cellulitis/abscess/ulcer/necrosis) on de‑identified, clinician‑verified images with robust augmentation across skin tones and devices.
- Calibrate risk with probability thresholds + human‑in‑the‑loop review to reduce dangerous false negatives.
- Validation on external test sets, fairness audits (e.g., Fitzpatrick skin types), and prospective outcome measures (time‑to‑care).
- Edge inference to enable offline screening for privacy, speed, and reach.
- Care navigation: one‑tap links to local clinics/telehealth, community resources, and wound‑care education.
Inline math example: We imagine a research risk score \(R\) that blends visual cues and host factors: \( R = w_1\cdot\text{erythema} + w_2\cdot\text{exudate} + w_3\cdot\text{tissue damage} + w_4\cdot\text{host factors} \).
Display math example: $$ R = w_1\cdot\text{erythema} + w_2\cdot\text{exudate} + w_3\cdot\text{tissue damage} + w_4\cdot\text{host factors (e.g., diabetes)} $$
Our ethos
We’re building for people who wait—because life is complicated, money is tight, stigma hurts, and fear is real. PathoScan’s job is simple: shine a small light earlier so fewer wounds become life‑changing emergencies.
Credits & disclaimer
We’re a student team building PathoScan to demonstrate how careful design + accessible AI can support earlier decisions. PathoScan is not a medical device and does not diagnose. If our app suggests “seek attention,” please see a clinician promptly.

Log in or sign up for Devpost to join the conversation.