Inspiration A few years ago, one of our team members watched her grandmother come home from the hospital after a serious treatment carrying a bag full of medications, a stack of discharge papers, and instructions that even the family struggled to understand. They worried constantly: Is she taking the right pill at the right time? Are we missing a warning sign? That moment never left us. Because it isn't rare it's the norm. Every year, nearly 1 in 5 patients is readmitted to the hospital within 30 days of discharge. And in many of those cases, the root cause isn't a failure of medicine. It's a failure of communication. Discharge papers are routinely written at a 12th-grade reading level yet the average patient reads at an 8th-grade level. Elderly patients living alone, those with low health literacy, or anyone managing a complex medication regimen are especially vulnerable. They leave the hospital confused, overwhelmed, and sometimes return in an ambulance. We came to understand that one of the biggest challenges in healthcare doesn't end inside the hospital it begins the moment the patient goes home. So we asked: what if the discharge process was as intelligent and personalized as the care that preceded it? That question born from a personal experience and backed by a systemic reality became DischargeGuardian AI: a system designed to make post-discharge care safer, clearer, and truly understandable for every patient and every family. What it does DischargeGuardian AI is an AI-powered discharge transition platform that transforms complex clinical information into clear, personalized discharge plans simultaneously for both the clinician and the patient.
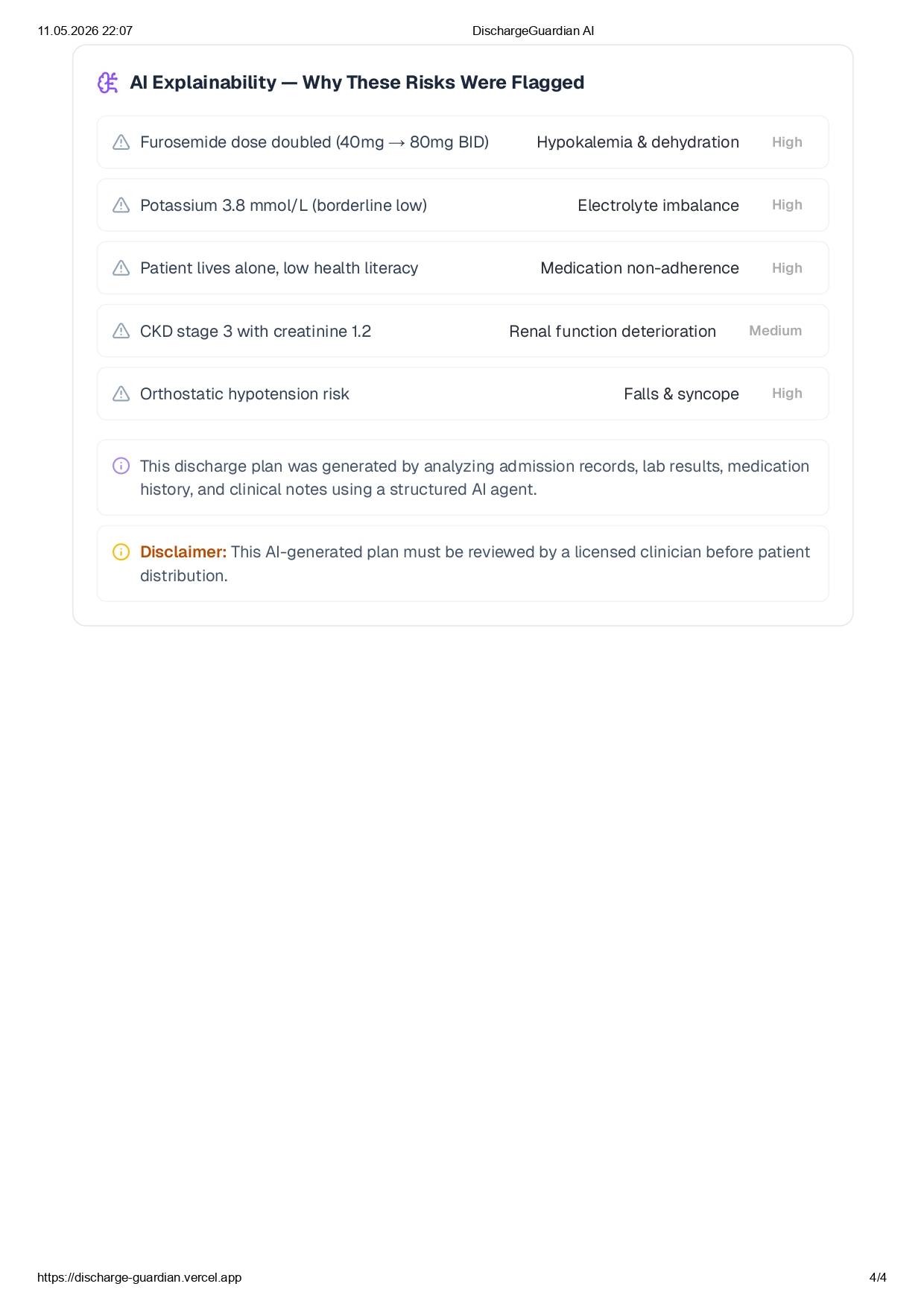
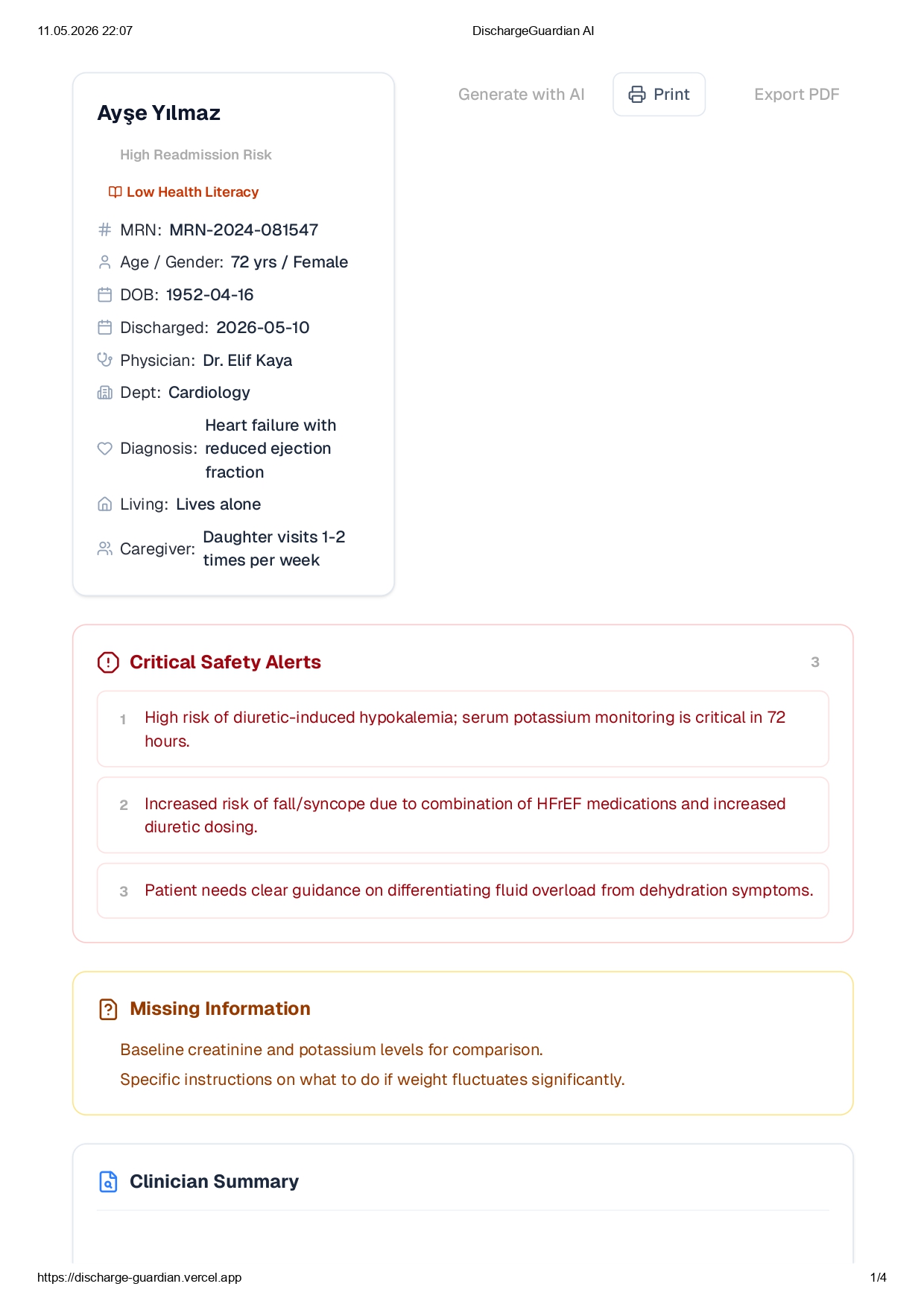
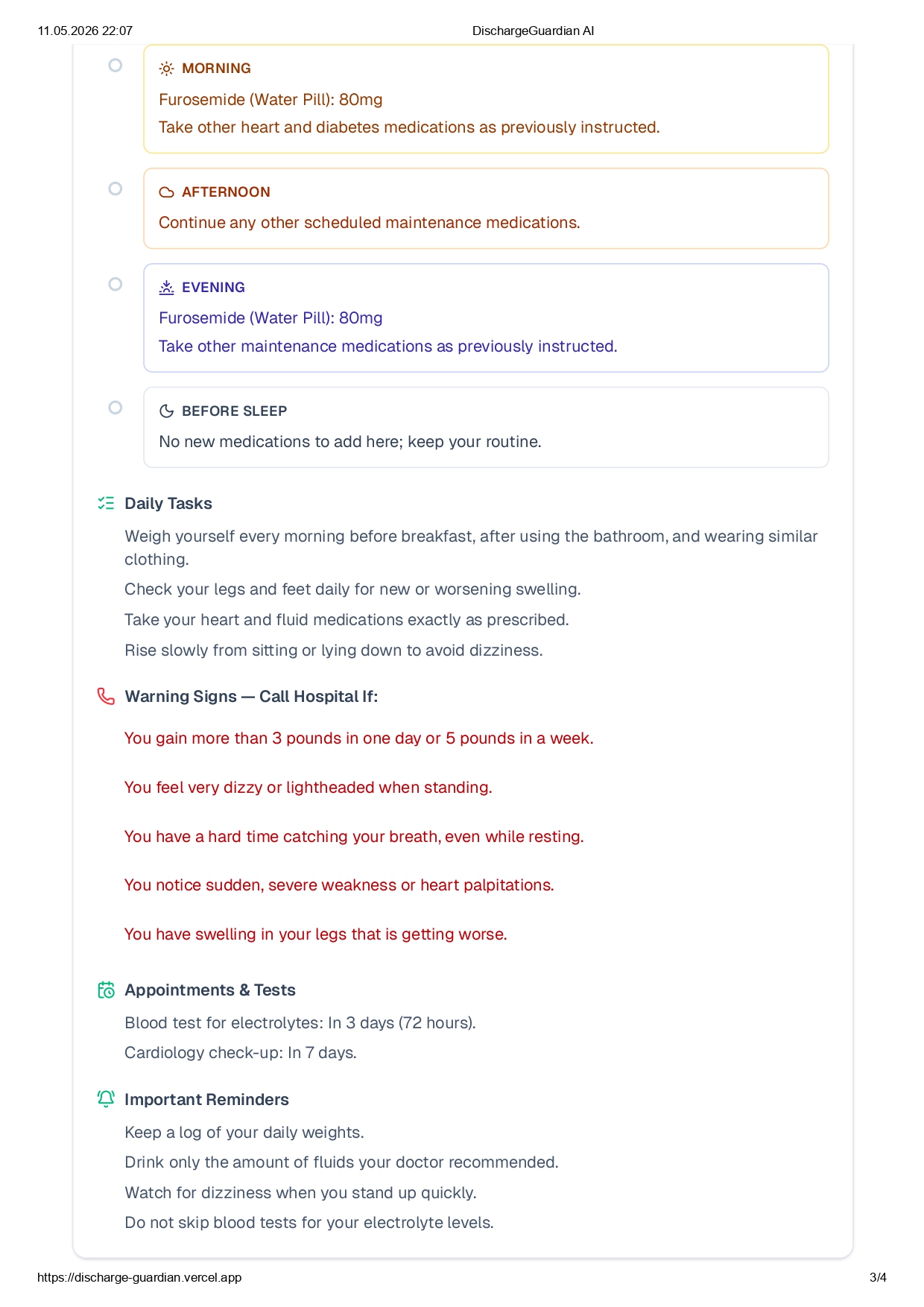
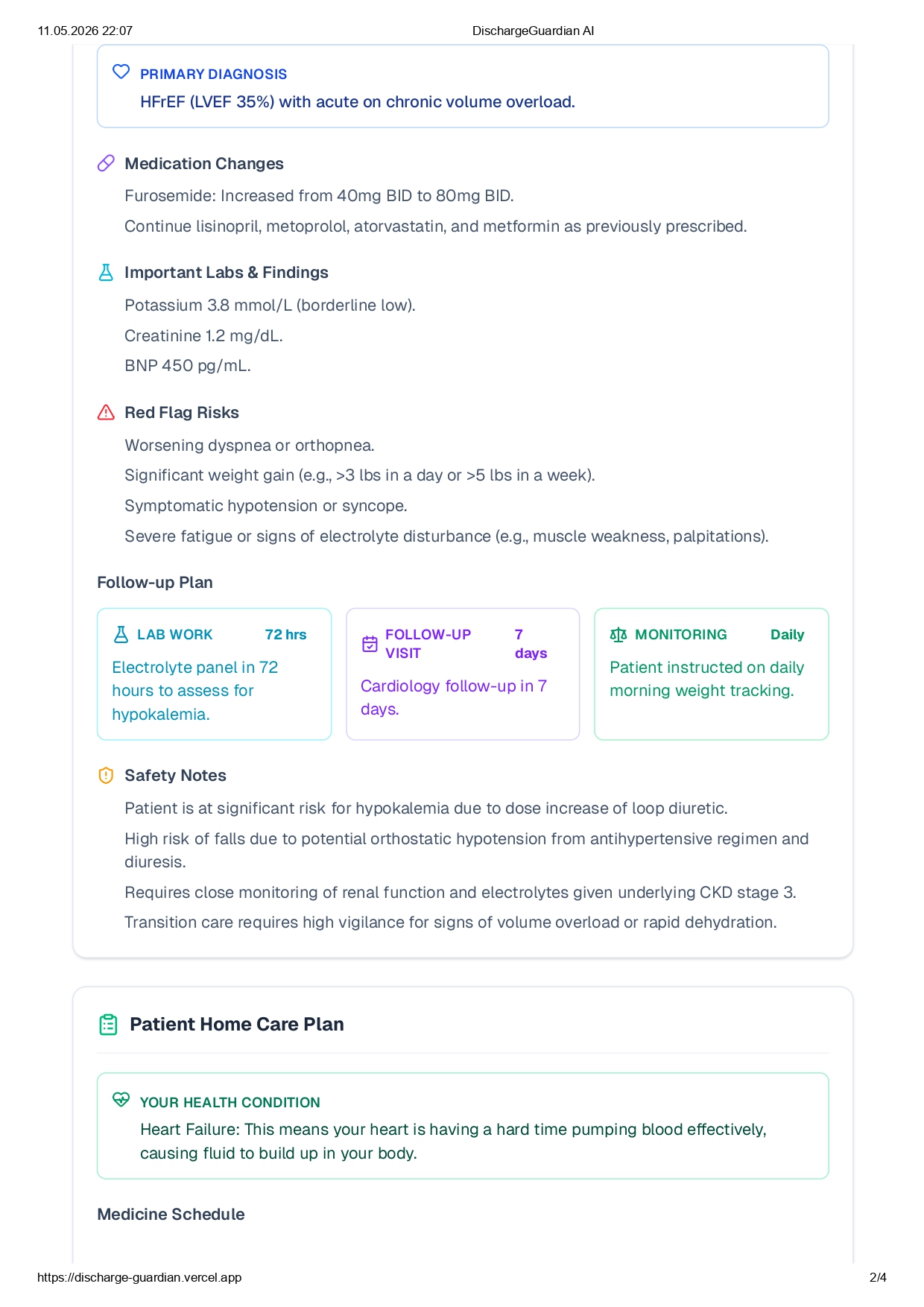
For clinicians: A structured summary with diagnosis, medication changes, red flag risks, lab results, and follow up timeline all auto-generated and review-ready. For patients: A plain-language home care plan with a daily medication schedule, warning signs to watch for, and upcoming appointments written at an accessible reading level. For safety: An AI explainability layer that shows why each risk was flagged, and a missing information detector that alerts clinicians to data gaps before the plan reaches the patient.
The platform supports PDF export, print-ready formatting, and bilingual output (TR/EN).
How we built it We built DischargeGuardian AI on a multi-agent reasoning pipeline powered by Claude (Anthropic). Rather than using a single monolithic prompt, we decomposed the problem into specialized agents:
Risk Stratification Agent — identifies readmission risk factors from clinical data Medication Safety Agent — detects dangerous dose changes and drug interactions Health Literacy Adapter — rewrites clinical content at the patient's reading level Explainability Agent — generates reasoning traces for every flagged risk
Risk score for a patient pp p is computed as: R(p)=∑i=1nwi⋅fi(p)R(p) = \sum_{i=1}^{n} w_i \cdot f_i(p)R(p)=i=1∑nwi⋅fi(p) where fi(p)f_i(p) fi(p) is a clinical risk feature (e.g. polypharmacy burden, social isolation, lab abnormality flags) and wiw_i wi is its importance weight. Patients with R(p)>θR(p) > \theta R(p)>θ are flagged as High Readmission Risk. The frontend is built with Next.js + Tailwind CSS, deployed on Vercel, with PDF/print export and a bilingual interface.
Challenges we ran into Dual-audience output: Generating content that is simultaneously appropriate for a physician and a 72-year-old patient living alone — in the same pipeline — required significant prompt engineering and careful output structuring. Hallucination risk in clinical contexts: In healthcare, a fabricated lab value or wrong dosage can be dangerous. We implemented structured output schemas and validation layers to ensure the AI never invents clinical data. Missing data handling: Real-world clinical data is almost always incomplete. We built a dedicated "Missing Information" detection layer so clinicians are always alerted to gaps before distributing any plan to a patient. Balancing AI autonomy with clinical oversight: The system is intentionally designed as a decision support tool, not an autonomous one. Every output carries a mandatory clinician review disclaimer getting that balance right in both UX and copy was a challenge in itself.
Accomplishments that we're proud of
Built a working end-to-end discharge pipeline that produces clinically structured and patient-readable output from the same input something that typically requires a full clinical documentation team. Designed an AI explainability layer that shows clinicians the exact reasoning chain behind every flagged risk, making the system auditable and trustworthy. Created a bilingual (TR/EN) platform with print and PDF export that is genuinely ready for a clinical pilot. Demonstrated that a small team can tackle a real, high-stakes healthcare workflow in a hackathon timeframe and produce something that feels production-ready.
What we learned
Prompt architecture matters as much as model choice. Decomposing into specialized agents produced far better results than a single large prompt. Context-sensitive risk is hard. A furosemide dose doubling might be routine to a cardiologist but life-threatening without potassium monitoring for a patient with borderline hypokalemia the AI had to surface contextual risk, not just rule-based flags. Explainability is non-negotiable in healthcare AI. Clinicians don't trust black boxes, and they shouldn't have to. Designing for low health literacy is genuinely difficult. Writing clear, actionable instructions without losing medical accuracy requires as much care as the clinical content itself.
Built With
- anthropic-messages-api
- claude-(anthropic)
- next.js
- pdf-export
- react
- rest-api
- tailwind-css
- typescript
- vercel

Log in or sign up for Devpost to join the conversation.