-
-

Logo
-
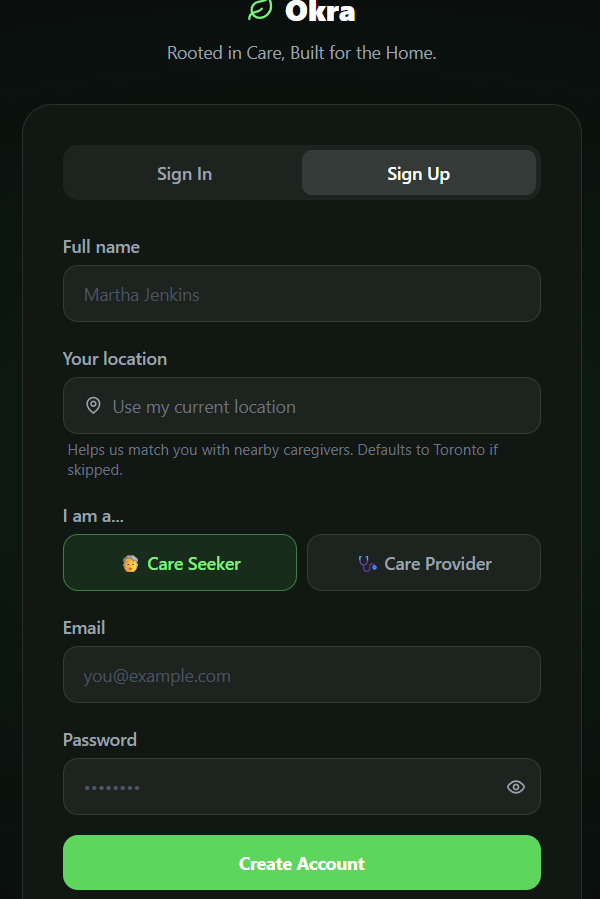
Landing Page
-
Login/Signup
-
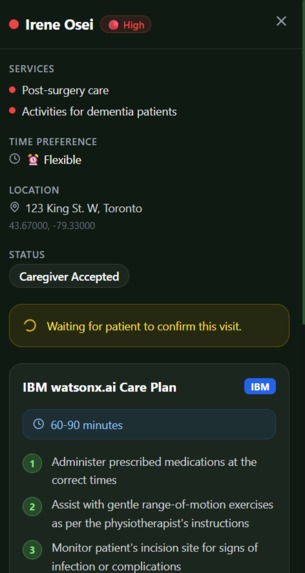
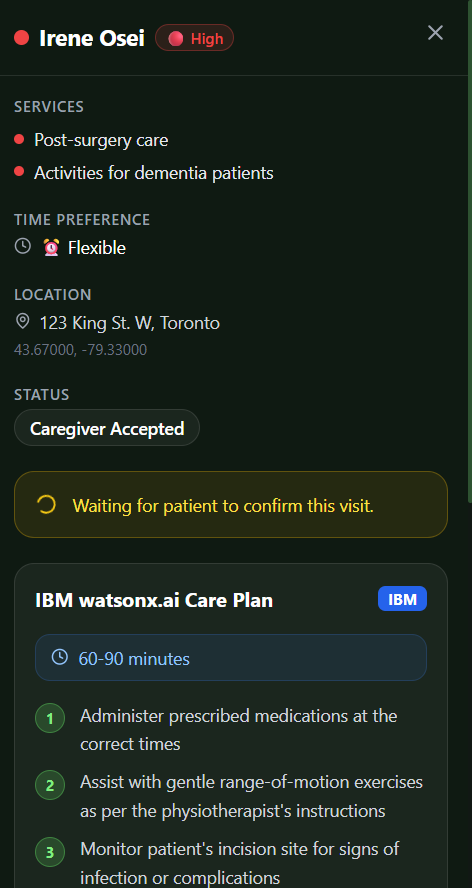
Generated care plan
-
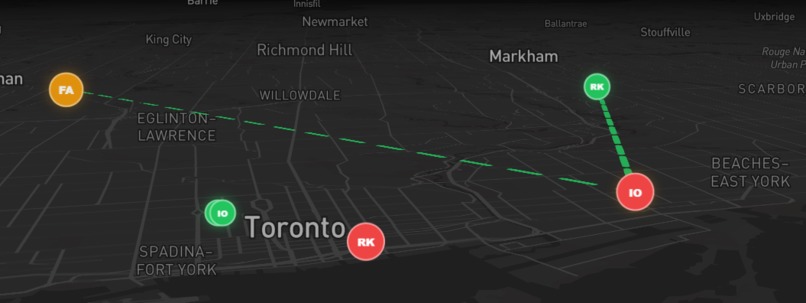
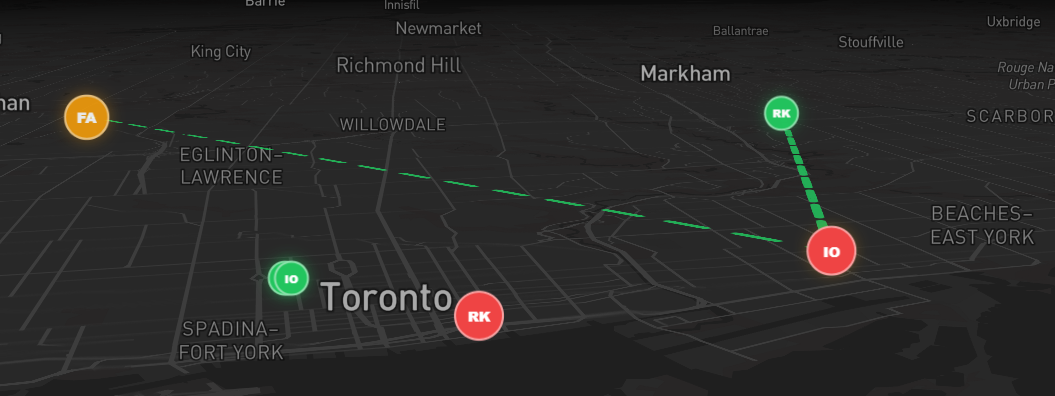
Map view with routed jobs
-
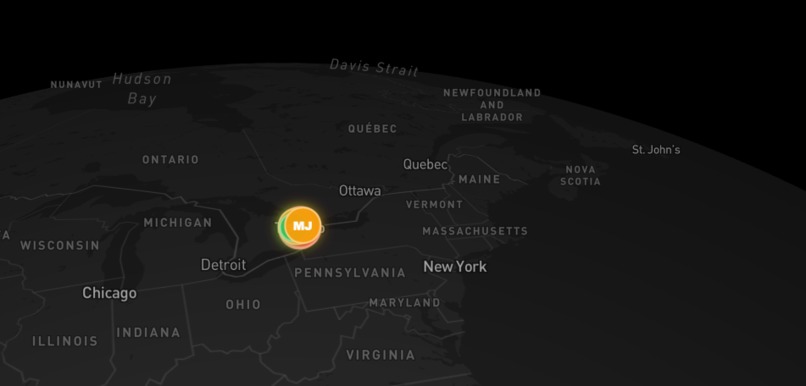
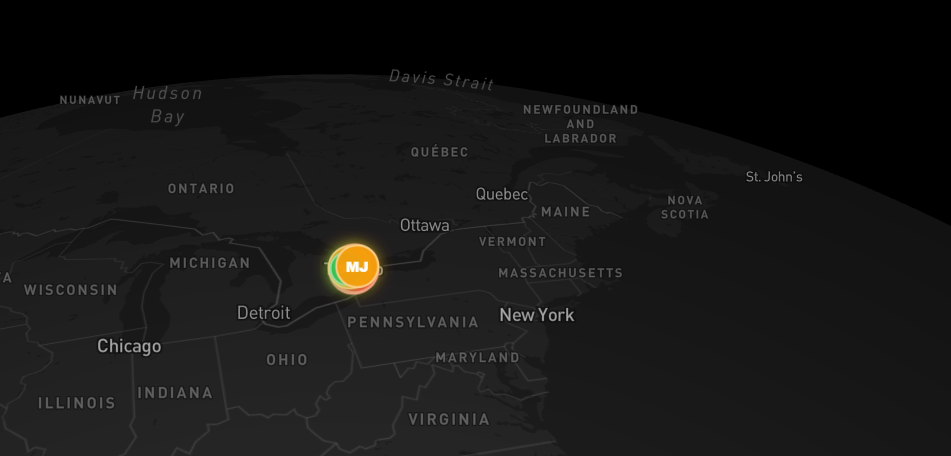
Map view
-
Logo Variation
-

Logo Variation
-
Logo Variation

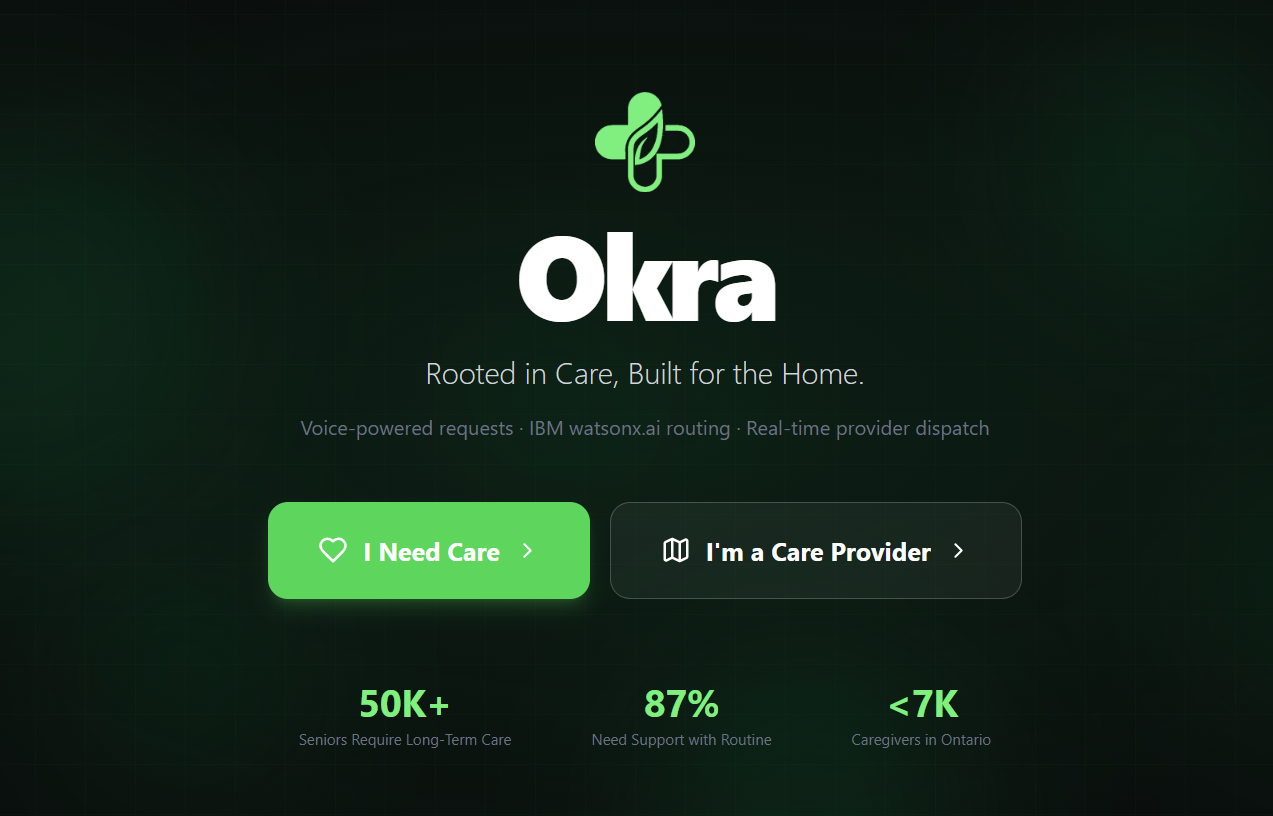


Project Okra: Rooted in Care, Built for the Home
Inspiration
Up to 91% of Canadians want to age in their own homes, yet only 26% believe they actually can (Sinha, 2020; March of Dimes Canada, 2021). The seed for Project Okra was planted when we looked at the stark reality of aging in Ontario: our province isn't just facing a medical crisis; it's facing a connection and logistics crisis.
The Broken System
The current system is fundamentally broken. We were deeply moved by the "Invisible Collapse" of the family unit: today, nearly 47% of family caregivers in Ontario are in high distress, logging over 40 hours of unpaid care a week—effectively a second full-time job (Canadian Institute for Health Information, 2026). This distress is a direct result of a massive health-workforce deficit, with over 100,000 open positions in the sector making professional help nearly impossible to find (CBC News, 2024).
With a long-term care waitlist that has doubled in a decade—leaving over 50,000 seniors in a queue with wait times stretching 18 to 36 months (Ontario Ministry of Long-Term Care, 2025; Ontario Health, 2024)—we saw a system buckling under its own weight. We noticed a "non-obvious" gap: 87% of seniors entering long-term care don't actually need 24/7 medical supervision; they need help with the Activities of Daily Living (ADLs)—meal prep, laundry, and social interaction (Canadian Institute for Health Information, 2025).
The Global Context
By studying the demographic cliff in Singapore—where the old-age support ratio plummeted from 10.5 working adults per senior to just 4.0 in a generation (Pang, 2022)—we realized Toronto faces the exact same demographic collapse. Ontario will need an additional 6,800 personal support workers by 2029 just to maintain current, already-strained service levels (CBC News, 2024). The aging of Baby Boomers will overwhelm current infrastructure unless fundamentally reimagined.
Our Belief
Project Okra was born from the belief that we can fix this broken system. By using Generative AI to lower the barrier for requesting help and professionalizing a decentralized community care workforce, we can bridge the supply-demand gap. We are building the infrastructure required to stop the institutionalization of our seniors, alleviate the crushing burden on family caregivers, and let our communities age with the dignity they deserve.
What It Does
Project Okra is a decentralized, Agentic AI-powered dispatch platform that acts as the missing infrastructure for community care. It optimizes the workforce we already have through two laser-focused user experiences.
For the Requestor: Zero-Friction Voice Intake
We eliminated the friction of complex digital interfaces and medical intake forms, which actively exclude elderly users. A distressed senior or family member simply taps a giant microphone button and speaks their needs:
"My mom fell and needs help getting out of bed, and she needs her medications"
Our AI, powered by IBM watsonx.ai (Granite), performs real-time Semantic Triage, parsing the messy audio into structured data, categorizing the service request, and assessing urgency. This transforms a moment of panic into actionable information instantly.
For the Provider: The "God-View" Dispatch Dashboard
Care agencies and independent Personal Support Workers (PSWs) access a dark-mode, Mapbox-powered geospatial dashboard. Instead of being assigned rigid, inefficient shifts, they can claim requests that fit their location and schedule.
Upon accepting a task, the platform instantly generates an AI Care Briefing—a customized timeline and protocol based on the senior's specific medical history and current request. Providers walk into each home fully prepared, eliminating the "scope creep" that leads to 40-hour unpaid work weeks and ensuring they have total transparency before committing to a job.
Addressing the Core Challenges
Ending "Blind" Care: We solve caregiver anxiety and burnout by providing Total Transparency. Providers see the exact workload and a generated care plan before they commit, eliminating scope creep and the unpaid overtime that leads to burnout.
Bridging the Workforce Gap: By focusing on ADLs—which 87% of seniors actually need—we unlock a new tier of community caregivers, alleviating the pressure on the 100,000-person professional nursing deficit.
How We Built It
In healthcare, an AI hallucination or autonomous mis-scheduling error can cost lives. We engineered a highly constrained, deterministic agentic workflow using an enterprise-grade tech stack.
The Brain: IBM watsonx.ai
We deployed IBM Watsonx as a dual-agent system with strict guardrails:
- The Triage Agent: Parses messy, panicked voice transcriptions from the Web Speech API, categorizes urgency, and outputs strict, actionable JSON mapped to our clinical database.
- The Dispatch Agent: Dynamically generates personalized logistics and care plans for providers upon appointment acceptance.
Core Framework & Language
- Next.js 14 (App Router): Full-stack engine for layouts, server components, and edge-compatible API routes, powered by React 18.
- TypeScript: Utilized as the primary language across the entire stack—including frontend components, API routes, state management, and domain-specific type definitions—to ensure type safety and scalability.
- Supabase (PostgreSQL): The persistent backend with custom schemas, Row-Level Security (RLS) policies for data integrity and user-specific data isolation, Auth for secure logins, and Realtime Subscriptions to push instant appointment updates to caretakers.
Geospatial & Routing
- Mapbox GL JS: Renders the 3D geospatial dashboard for real-time mapping, provider routing context, and location-based request clustering.
- Custom Optimization Algorithms: Travelling Salesperson Problem (TSP) approximation algorithms calculate the most optimal dispatch routes in real-time.
Frontend & User Experience
- Tailwind CSS & Framer Motion: Responsive layouts and high-fidelity fluid animations.
- Zustand: Lightweight global state management for handling client-side stores and session state.
- Lucide React: Clean, accessible iconography.
Voice & Location
- Web Speech API: Frictionless voice intake.
- Geolocation API: Precise request positioning for geographic clustering.
Additional Languages & Tools
- SQL: Custom Supabase schemas and Row-Level Security (RLS) policies for data integrity.
- JavaScript (ESM): Project configuration and runtime scripting.
- CSS: Global styling combined with utility-first Tailwind design layer.
- Utility Libraries: date-fns for complex time-handling, uuid for unique identifier generation, clsx/tailwind-merge for dynamic styling logic.
- Build Tooling: Node.js environment with npm-driven workflows for building, linting, and deployment.
- PostCSS & Autoprefixer: Cross-browser style compatibility.
AI Implementation & Development Velocity
Over 70% of our codebase was AI-generated, enabling rapid iteration while maintaining safety through strict architectural constraints. Every AI decision is logged and auditable for clinical compliance. We leveraged Agentic AI not just in the product but in our development process itself, demonstrating the power of the technology we built.
Challenges We Ran Into
Safety & Clinical Compliance
Building AI systems in healthcare requires absolute precision. We had to engineer guardrails so strict that the AI can never hallucinate a medical decision or mis-schedule a critical appointment. This meant designing a deterministic agentic workflow rather than a generative one—where every output is constrained by our clinical database schema.
The Mismatch Between Demand & Supply
We discovered that the problem wasn't just a shortage of caregivers—it was a structural breakdown in how care gets coordinated. The informal family system is collapsing (46.8% of caregivers in severe distress) while the formal professional system can't scale (100,000+ open positions). We needed a platform that could bridge both worlds simultaneously.
Elderly Users & Digital Friction
Traditional healthcare platforms are designed for younger, tech-literate users. We had to eliminate all digital friction from the requestor side. Voice intake wasn't optional—it was essential. This meant integrating Web Speech API with IBM Granite in a way that handles panicked, nonlinear speech patterns.
Real-Time Routing at Scale
Optimizing provider routes in real-time while respecting geographic clustering and ADL-specific expertise required custom TSP approximation algorithms. We couldn't rely on off-the-shelf solutions; we had to build our own geospatial optimization layer.
The "Non-Obvious" Gap in Care Levels
We had to educate stakeholders that 87% of seniors in long-term care don't need intensive medical intervention—they need community support. This reframing was essential to unlock the potential of a decentralized, neighborhood-based care model.
Accomplishments That We're Proud Of
Agentic Scheduling Innovation
The core innovation is our Agentic Scheduling Assistant. Unlike static marketplaces, our AI doesn't just display data—it acts as a Digital Triage Nurse. It uses IBM Granite to autonomously cluster nearby requests and generate clinical-grade care timelines from raw voice input. This reduces the administrative overhead of care coordination to near-zero.
Voice-First Interface for Accessibility
We built the world's first truly accessible home care platform. By eliminating forms and complex interfaces, we've made it possible for a frail, panicked senior to request help in seconds—just by speaking.
Total Provider Transparency
We solved a fundamental problem in care work: providers no longer walk into jobs blind. The AI Care Briefing gives them complete context—medical history, specific ADL needs, urgency level, and optimal routing. This eliminates scope creep and the burnout it causes.
Deterministic AI in Healthcare
We proved it's possible to use Generative AI safely in healthcare by constraining it to a deterministic, auditable workflow. Every AI decision is logged, explainable, and compliant with clinical standards.
Rapid Development with AI
Over 70% of our codebase was generated with AI assistance, demonstrating that Agentic AI isn't just a product innovation—it's a development methodology. We built a complex healthcare platform in a fraction of the time traditional development would require.
Bridging the Informal & Formal Care Systems
We created a platform that professionalizes informal care without bureaucratizing it. A neighbor, a retiree, or a young person can join the network and start helping seniors in their community—instantly matched and supported by AI.
What We Learned
The Crisis Is Logistics, Not Medicine
Our biggest insight: Ontario's care crisis isn't a shortage of healthcare knowledge—it's a logistics and coordination problem. 87% of seniors in long-term care could be cared for at home if the administrative barrier were lower.
Agentic AI Changes the Economics of Care
By automating triage and routing, we've geometrically multiplied the effective capacity of a single caregiver. An experienced PSW can now handle 3–4x more clients because the AI handles scheduling, routing, and care plan generation.
Voice Is Essential for Elderly Users
Digital forms are a barrier to care, not a solution. Voice-first interfaces aren't just nice-to-have; they're essential for reaching the people who need help most.
The Caregiver Is Often More Vulnerable Than the Senior
We learned that family caregivers are suffering as much as seniors. By relieving administrative burden on providers, we're not just improving care quality—we're protecting the health of an entire generation of burnout-prone workers.
Safety & Speed Aren't Mutually Exclusive
We proved that you can use Generative AI rapidly in healthcare without sacrificing safety. The key is architectural constraints, not restrictions on the AI itself.
What's Next for Okra - Home Care Platform
Scaling Across Ontario
We are building the infrastructure required to stop the institutionalization of our seniors. Our immediate goal is to scale across Ontario, reaching 10,000+ caregivers and serving 50,000+ seniors within three years.
Reducing Long-Term Care Dependency
By keeping vulnerable populations out of overburdened emergency rooms and long-term care institutions, we can directly reduce waitlist pressure. Each senior who ages in place is both a human victory and a fiscal win—home care costs a fraction of institutional care.
Expanding ADL-Specific Care Networks
We're building specialized networks of caregivers trained in specific ADL clusters (mobility support, cognitive care, palliative care). The platform will match seniors not just geographically but by expertise.
Relieving Caregiver Burnout at Scale
We directly target the 46.8% caregiver distress rate by professionalizing informal care. By providing total transparency and eliminating scope creep, we aim to reduce caregiver distress by 50% within two years.
Advancing AI-Driven Care Coordination
We're extending the Agentic AI system to predict care needs before they become emergencies. By analyzing patterns in voice requests and appointment history, we can alert family members and providers to escalating risks—turning reactive care into proactive care.
Building a Blueprint for Global Aging
The demographic cliff is not unique to Ontario. Singapore, Japan, South Korea, and much of Western Europe face the same crisis. Our platform is designed to be replicable, and we aim to become the global standard for AI-orchestrated community care.
References
Canadian Institute for Health Information. (2025). Profile of residents in residential and hospital-based continuing care, 2024–2025. Ottawa, ON: CIHI.
Canadian Institute for Health Information. (2026). Data and reports: Caregiver distress in home care. Ottawa, ON: CIHI.
CBC News. (2024). Ontario seniors, aging population, and home care demand. Retrieved from https://www.cbc.ca/news/canada/toronto/ontario-seniors-aging-population-home-care-demand-1.7118076
March of Dimes Canada. (2021). Aging in place: Perspectives of older Canadians. Toronto, ON.
Ontario Health. (2024). Wait times for long-term care. Retrieved from https://www.hqontario.ca/system-performance/Long-Term-Care-Home-performance/wait-times
Ontario Ministry of Long-Term Care. (2025). Client profile database (CPRO) reports. Government of Ontario.
Pang, W. S. (2022). Healthcare challenges at societal level [CC0007 Science and Technology for Humanity Lecture Slides]. Nanyang Technological University, Singapore.
Sinha, S. K. (2020). Scenarios for seniors' care: Future challenges, current gaps, and strategies to address them. C.D. Howe Institute. Retrieved from https://cdhowe.org/publication/scenarios-seniors-care-future-challenges-current-gaps-and-strategies-address/
Statistics Canada. (2024). Caregiving in Canada: Sandwiched caregivers and the burden of care (Catalogue no. 89-652-X2024002). Retrieved from https://www150.statcan.gc.ca/n1/pub/89-652-x/89-652-x2024002-eng.htm
Built With
- clsx
- css
- date-fns
- framer
- gemini
- html
- ibm-granite
- ibm-watson
- javascript
- lucide-react
- mapbox
- next.js
- node.js
- pusher
- react
- sql
- supabase
- tailwind-css
- typescript
- web-speech-api
- zustand





Log in or sign up for Devpost to join the conversation.