-
-
Interface Homepage
-
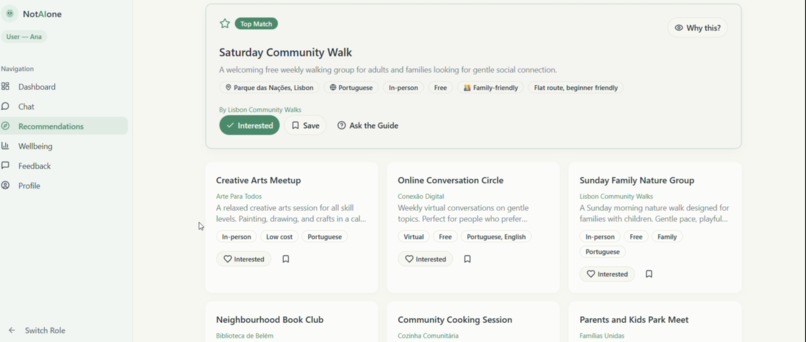
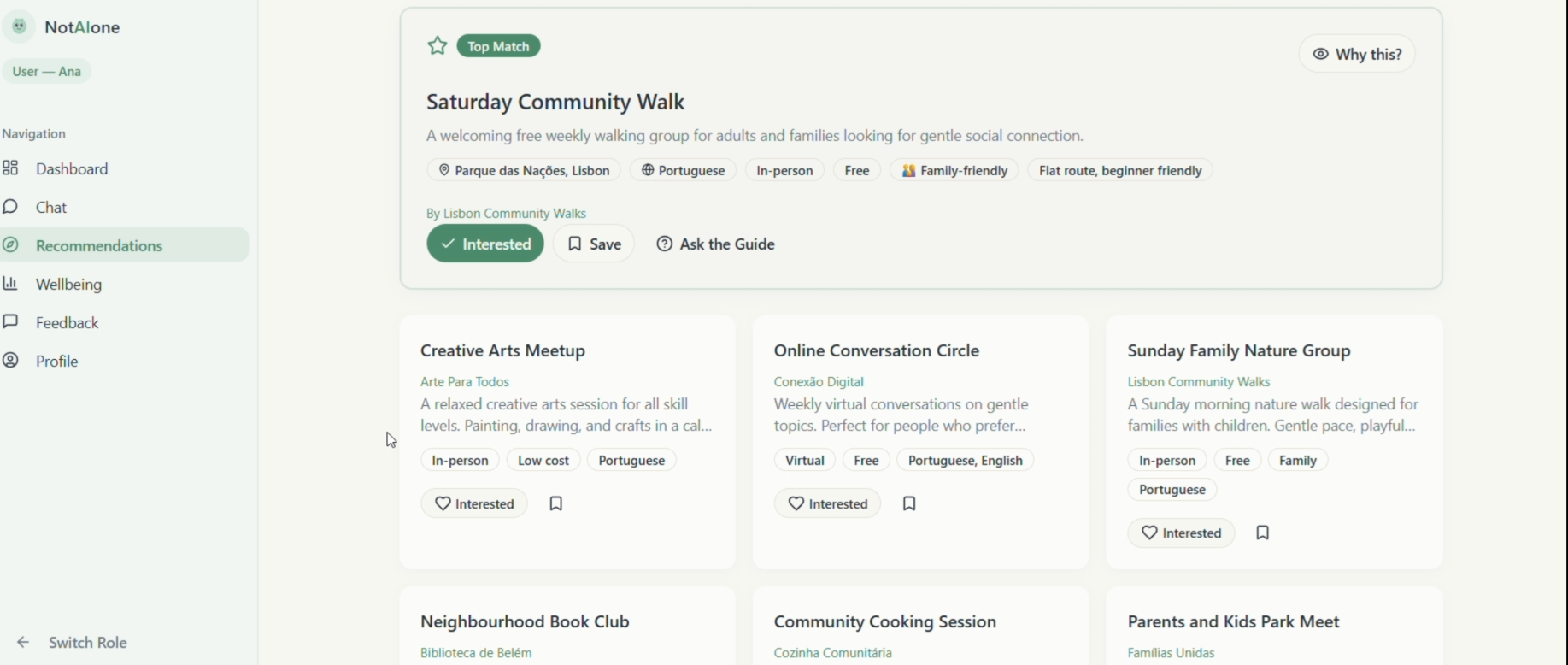
User interface
-
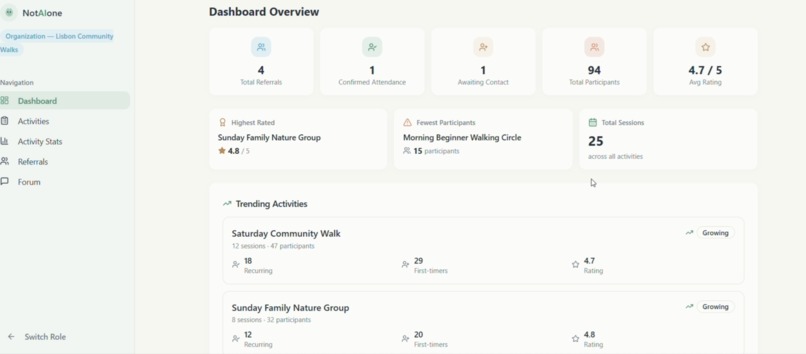
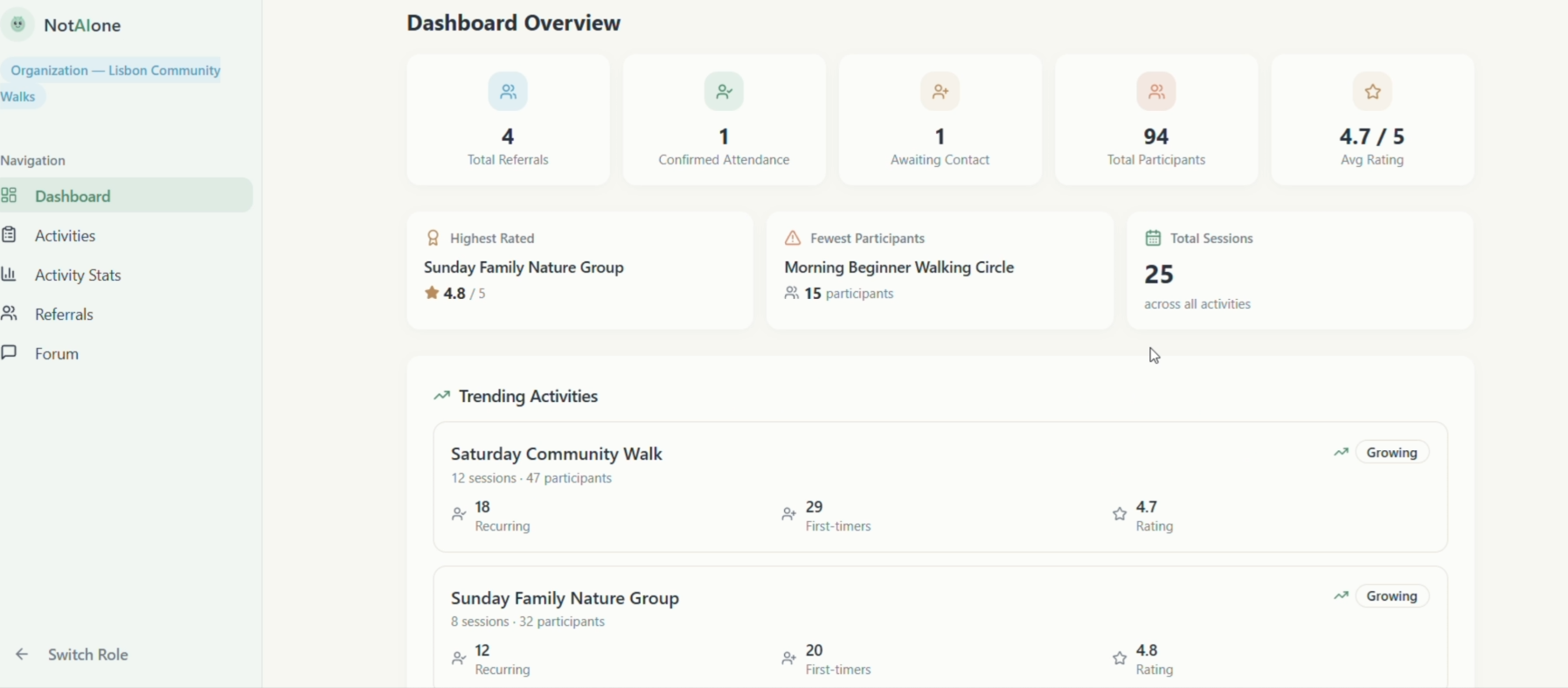
Health professional interface
Inspiration
A few months ago, a young woman (34, recently moved to a new country) came to see a family doctor. She couldn't sleep. She felt tired all the time. Every test came back normal.
And then, almost as an afterthought, she said: "I just don't talk to anyone anymore."
She wasn't sick. She was lonely. And the doctor had nothing to prescribe for that.
This is not a rare story. The WHO and the U.S. Surgeon General have both declared loneliness a global public health crisis. Its health impact is comparable to smoking 15 cigarettes a day, raising the risk of heart disease by 29% and dementia by 50%. And here's the paradox that drove us: in the age of AI, millions of people are already turning to chatbots for emotional support, without any clinical guidance. That may be making isolation worse. We are building AI that keeps people on their screens, when what they actually need is to walk out their front door.
We asked ourselves: what if we used AI not to replace human connection, but to rebuild it?
What it does
NotAlone is a digital social prescribing platform that reconnects lonely people with their communities, using AI as a bridge, not a destination.
A health professional (doctor, psychologist, or social worker) identifies someone at risk of isolation and refers them to the platform. The user then meets an AI companion. A warm, professional, and deliberately non-human that talks with them daily in their own language. Through natural conversation, it learns what they enjoy, what barriers they face, and what kind of connection might work for them.
Then it does something no chatbot on the market currently does: it connects them to real, free local activities (a multilingual parents' cooking class, a weekend hiking group, a volunteer program) things already out there, but invisible to the people who need them most.
The referring professional stays in the loop through a clinician dashboard. They never see conversation content — privacy is absolute — but they receive engagement insights and, critically, real-time safety alerts if the AI detects warning signs. The model is B2B2C: municipalities and healthcare systems pay, because preventing severe mental health cases is far cheaper than treating them.
How we built it
The architecture is straightforward and built on proven infrastructure:
- Conversational AI layer: powered by LLM APIs with multilingual support across 50+ languages, enabling natural conversation without manual translation.
- Community resource database: a structured, searchable database of local activities and organisations, with a self-registration portal for NGOs and associations.
- Referral and access system: role-based access control with a clinician-facing referral workflow and webhook-driven safety alert escalation.
- Clinician dashboard: lightweight engagement metrics and alert management, with no access to conversation content.
- Privacy architecture: designed for GDPR and HIPAA alignment from day one, not as a retrofit.
The real complexity wasn't technical, it was in the conversation design and the clinical workflow integration. Every conversational decision was tested against one question: does this move the user toward real-world connection, or toward more screen time?
Challenges we ran into
- Designing for subclinical users. NotAlone sits in a grey zone: users who are too well for psychiatry but too isolated to recover alone. Calibrating the AI's tone, escalation thresholds, and clinical boundaries for this population required careful iteration.
- Avoiding the AI dependency trap. The companion had to be warm enough to engage users, but deliberately designed to make itself unnecessary over time. That tension is genuinely hard to resolve in conversation design.
- Safety architecture. Building a robust escalation system for edge cases while preserving the lightness and warmth of the experience was one of our most difficult design challenges.
- Bootstrapping community resources. Connecting people to local activities requires a live, structured, multilingual resource database. Making it frictionless for organisations to self-register is an ongoing challenge, particularly in low-resource settings.
- Health system integration. Clinical workflows vary enormously across municipalities and care networks. Designing a referral system flexible enough to adapt without losing clinical rigour took significant iteration.
Accomplishments that we're proud of
- We designed an AI companion that points outward : every conversational pattern celebrates real-world actions, not engagement with the app itself.
- We built a safety escalation architecture that protects vulnerable users while maintaining full conversational privacy.
- We created a model that genuinely bridges the gap between digital AI tools and human social prescribing. A combination the NHS and WHO have endorsed in principle but that has never been delivered at scale.
- We addressed loneliness as a transversal public health challenge, one that cuts across age, gender, and culture, with a single platform adaptable to all of them.
- We aligned the entire product with UN SDG 3 (Good Health and Well-being) and UN SDG 10 (Reduced Inequalities), reaching those who fall through the cracks of the mental health system.
What we learned
Building NotAlone taught us that trust is the real infrastructure. Without it, no vulnerable person will engage — and that shaped every decision we made, from privacy architecture to the companion's non-human design.
We also learned that the hardest problems here aren't technical. The challenge is conversation design: building an AI that is warm without being deceptive, supportive without being addictive, and clinically safe without being cold. That balance requires multidisciplinary thinking sucha s technology, clinical practice, ethics, and community knowledge working together.
Finally, we learned that social prescribing as a model already has a growing evidence base, particularly from the UK, where it has reduced GP visits and improved wellbeing outcomes. What this specific combination of AI and social prescribing needs now is its own rigorous evaluation. The hackathon prototype is step one toward that evidence.
What's next for NotAlone
Our immediate next step is a controlled pilot with one municipality or primary care network: between 100 and 500 users, measuring engagement frequency, community activity attendance, and wellbeing outcomes using validated scales (UCLA Loneliness Scale, WHO-5).
In parallel, we are seeking:
- Clinical collaborators to refine the safety protocols and conversation design.
- Pilot partners : municipalities, integrated care systems, or primary care networks willing to co-design the referral workflow.
- Community organisations to self-register their activities and help us bootstrap the resource database in target cities.
In two years, we want multi-city deployment, integration with electronic health records, and a published outcome study. We are building toward evidence, not just a product.
Because no one should hear "I just don't talk to anyone anymore" and have nothing to offer.
Built With
- lovable
- n8n
- openaiapi
- supabase


Log in or sign up for Devpost to join the conversation.