
AuraRing — Navigate Your Inner World
SDG 3: Good Health and Well-being
Team Member: Sofia Bouazizi
Abstract
Mental health disorders affect over 1 billion people worldwide, yet the average person waits 8 to 10 years between experiencing their first symptoms and receiving any treatment. This gap exists not because therapists are unavailable, but because most individuals lack the physiological self-awareness tools to recognize gradual emotional deterioration before it reaches crisis level. AuraRing is an AI-powered smart ring that continuously monitors five biometric signals — heart rate, heart rate variability (HRV), blood oxygen saturation (SpO2), skin temperature, and motion — and uses Anthropic's Claude Sonnet large language model to detect emotional patterns, compute real-time stress and anxiety scores, and deliver tiered personalized interventions ranging from daily wellness insights to automatic crisis resource surfacing. By combining passive biometric sensing with AI-powered pattern recognition in a wearable device designed to be forgotten on the finger, AuraRing directly advances UN SDG 3 Target 3.4 and is purpose-built for the 2030 global mental health horizon.
1. Introduction
1.1 What is the Problem?
Mental health is the most under-addressed global health crisis of the 21st century. According to the World Health Organization, depression affects 280 million people globally and is the leading cause of disability worldwide. Anxiety disorders affect 301 million people. Suicide is the fourth leading cause of death among individuals aged 15 to 29 globally. Despite this scale, more than 75% of people in low- and middle-income countries receive no mental health treatment at all. In high-income countries, the average delay between first symptoms and first treatment is 8 to 10 years.
The core problem is not solely access to therapists — it is awareness. Most people do not recognize they are struggling until a crisis forces the issue. Current consumer wearables such as smartwatches and fitness bands track steps, sleep, and exercise but are not designed to monitor the physiological underpinnings of mental health: HRV-derived stress, autonomic nervous system dysregulation, or chronic anxiety patterns. There is no widely accessible, passive, always-on tool that bridges biometric data and mental health awareness.
1.2 Why is it Important?
Early detection of mental health deterioration is the single highest-leverage intervention point in the entire care pathway. Research consistently shows that early awareness reduces symptom severity, shortens recovery time, and dramatically lowers the risk of crisis events including hospitalization and suicide attempts. A tool that detects the physiological signature of rising anxiety hours before a person consciously feels it is more valuable than any post-crisis intervention. AuraRing is designed to be that tool — passive, private, and always present.
1.3 What UN SDG Target Are We Trying to Achieve?
- SDG 3.4 — By 2030, reduce premature mortality from non-communicable diseases by one third and promote mental health and well-being
- SDG 3.8 — Achieve universal health coverage including access to quality essential health-care services for all
- SDG 3.d — Strengthen the capacity of all countries for early warning, risk reduction, and management of national and global health risks
2. Background Research
2.1 What Research Did We Do?
We reviewed WHO mental health statistics, peer-reviewed literature on HRV as a validated stress biomarker, clinical studies on PPG-based physiological monitoring, and recent studies on large language model performance in health communication contexts. Key findings include the following.
Shaffer and Ginsberg (2017) established that HRV is a validated, non-invasive biomarker for autonomic nervous system function and psychological stress. RMSSD — the root mean square of successive differences between NN intervals — is the most clinically relevant time-domain HRV metric for real-time monitoring because it specifically reflects parasympathetic nervous system activity, the branch most directly suppressed by stress and anxiety.
Allen (2007) demonstrated that photoplethysmography (PPG) is a reliable optical method for extracting heart rate, HRV, and SpO2 from peripheral blood flow using LED wavelengths. Ring-form-factor PPG achieves comparable accuracy to wrist-based devices for resting measurements due to the dense capillary networks in finger tissue.
Menghini et al. (2019) conducted a systematic review of consumer wearables measuring physiological stress responses and found strong correlations with validated clinical stress instruments including the Perceived Stress Scale (PSS) and State-Trait Anxiety Inventory (STAI) when HRV and HR are combined as inputs.
Yang et al. (EMNLP 2023) showed that large language models demonstrate clinically comparable accuracy to trained mental health professionals at identifying linguistic and contextual markers of depression, anxiety, and emotional distress when given structured input.
The WHO World Mental Health Report (2022) calls urgently for scalable digital mental health tools as a public health priority, specifically mobile and wearable technologies capable of reaching underserved populations at zero marginal cost per user.
2.2 What Existing Tools or Data Did We Explore?
| Tool | Gap / Limitation |
|---|---|
| Oura Ring Gen 3 | Sleep and readiness tracking only. No real-time stress detection. No AI mental health analysis or anxiety scoring. |
| Apple Watch Series 9 | ECG and HR monitoring. No HRV-based stress index. No mental health AI layer. High cost excludes low-income users. |
| Fitbit Sense 2 | EDA (electrodermal activity) stress detection. No AI analysis. No anxiety scoring. No crisis intervention pathway. |
| Whoop 4.0 | Recovery and strain focus for athletic performance. No mental health framing. No AI-generated insights. |
| Moodmetric Ring | EDA-only ring for stress research. No HR, SpO2, or temperature sensors. No AI. Research-only, not consumer device. |
| MoodMap (app-only) | Journaling plus AI pattern analysis. No biometric data at all. Relies entirely on self-report rather than passive sensing. |
No existing consumer product combines continuous multi-sensor biometric monitoring, HRV-based stress and anxiety computation, and AI-powered personalized mental health intervention in a ring form factor. AuraRing fills this gap.
3. Solution Description
3.1 Explain the Idea Clearly
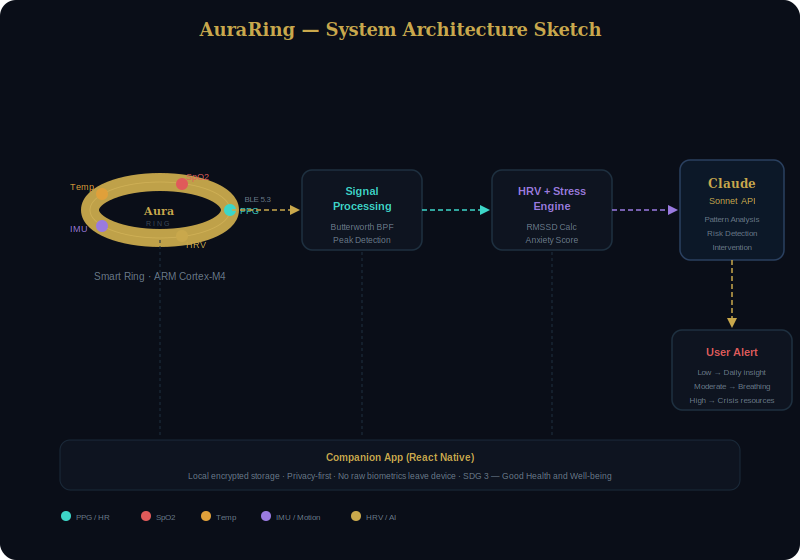
AuraRing is a smart ring and companion app system with three distinct layers.
Hardware Layer. A titanium-and-ceramic ring containing five sensors: a PPG optical sensor for heart rate, HRV, and SpO2; an infrared thermistor for skin temperature; and a 6-axis IMU (accelerometer plus gyroscope) for motion tracking and sleep staging. The ring communicates via Bluetooth 5.3 and runs on an ARM Cortex-M4 microcontroller. Specifications: 7-day battery life, IPX8 waterproofing to 50 meters, approximately 4 grams, available in US sizes 6 through 13.
Processing Layer. On-device digital signal processing handles raw sensor filtering and peak detection. A companion app (React Native) runs HRV computation using the RMSSD algorithm, calculates a composite stress index, computes an anxiety score from HR trend analysis, classifies overall risk level, and stores all data locally with AES-256 encryption. No raw biometrics leave the device unencrypted.
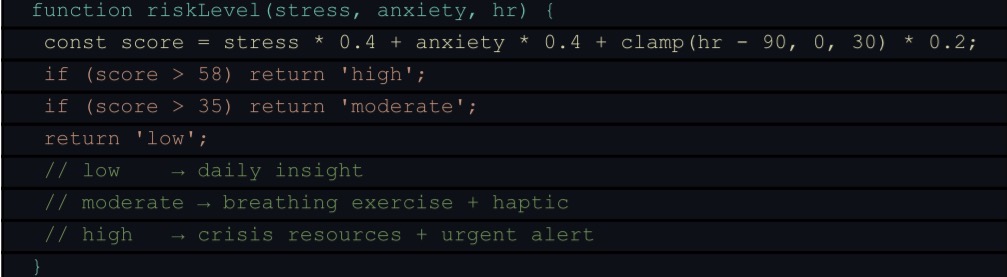
AI Layer. Anthropic's Claude Sonnet API receives structured biometric snapshots and returns plain-English pattern analysis, a risk level classification (Low, Moderate, or High), and a personalized intervention. Responses are tiered: Low risk generates a daily wellness insight, Moderate risk triggers a breathing exercise prompt with haptic feedback on the ring, and High risk surfaces crisis support resources automatically and immediately.
3.2 What Technologies and Algorithms Did We Use?
| Technology | Implementation |
|---|---|
| PPG Signal Processing | 4th-order Butterworth bandpass filter (0.5–4 Hz). IMU adaptive motion artifact subtraction. R-peak detection for NN interval extraction. |
| HRV — RMSSD | Root Mean Square of Successive Differences over a 60-second sliding window. Primary autonomic nervous system stress metric. |
| Stress Index | Composite 0–100 score: HRV deficit weighted 0.65, elevated HR weighted 0.35. |
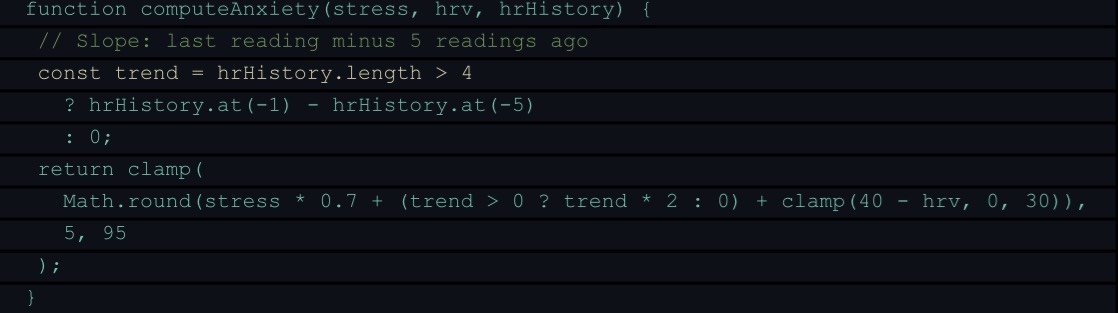
| Anxiety Detection | Extends stress score with HR slope trend over last 5 readings. Rising HR with declining HRV is the primary anxiety signal. |
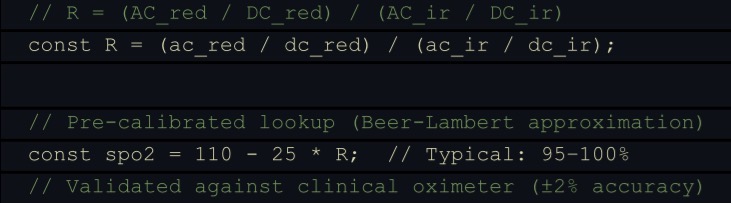
| SpO2 | Beer-Lambert Law R-ratio method: AC/DC ratio at red (660 nm) and infrared (940 nm) wavelengths mapped to oxygen saturation. |
| Risk Classification | Composite: stress × 0.4 + anxiety × 0.4 + HR excess × 0.2. Thresholds: Low < 35, Moderate 35–58, High > 58. |
| Claude Sonnet AI | POST /v1/messages to Anthropic API. Structured JSON output: summary, patterns, riskLevel, riskReason, suggestion. |
| React 18 | Single-file JSX application. Three.js r128 for 3D ring visualization. Recharts for live biometric streaming charts. |
3.4 How Does AI Help Solve the Problem?
Claude Sonnet is the intelligence layer that transforms raw numbers into human understanding. A stress score of 67 means nothing to most users. Claude translates it into a statement such as: "Your body has been running in high-alert mode for the past four hours. Your HRV is compressed and your heart rate is trending upward — classic signs of prolonged tension. Try stepping outside for five minutes." That translation is what creates actual behavior change.
The AI is also the risk escalation engine. It applies consistent, calibrated thresholds that distinguish normal afternoon stress from the early physiological signature of an anxiety crisis, and responds proportionally every time. This is not rule-based keyword matching. It is genuine language-grounded pattern reasoning over structured biometric time-series data, which means the response is contextual, personalized, and appropriate to the specific biometric signature of each individual user.
Built With
- 3d-visualization
- algorithims
- charts
- claude
- datasets
- fronted-framework
- storage

Log in or sign up for Devpost to join the conversation.