MOCHA — AI Hospital Automation Platform
Inspiration
Healthcare is broken in a way that's hiding in plain sight.
A physician working a standard week spends 13 hours on documentation — not on patients, not on diagnosis, not on healing. That's nearly a quarter of their working hours consumed by typing into systems that were designed to store data, not to think.
We didn't need to read a research paper to feel this. One of our team members watched a family member sit in a hospital room for 40 minutes while a doctor struggled to pull up the right records, asked the same questions three times, and then spent the last 5 minutes of the visit typing notes instead of talking. That moment stuck.
The math is staggering. If a hospital has 200 physicians each losing
$\frac{13 \text{ hrs}}{\text{week}} \times \$120/\text{hr}$,
the annual cost of documentation overhead alone is:
$$ C_{\text{doc}} = 200 \times 13 \times 120 \times 52 \approx \$16.2\text{M/year} $$
And that's before factoring in burnout and missed follow-ups.
43% of physicians report clinical burnout in 2024. The system isn't failing them — the system was never designed to help them.
We built MOCHA because the best use of AI isn't to replace doctors. It's to give them their time back.
What We Built
MOCHA is an end-to-end AI hospital automation platform with two core layers:
1. AI Documentation (Perplexity)
The moment a patient completes intake, Perplexity's AI generates a fully structured clinical note — chief complaint, history, relevant context — before the doctor enters the room. No dictation. No typing. The doctor walks in already briefed.
This is the core of MOCHA. The time saved here is immediate and measurable:
$$ \Delta t_{\text{per visit}} = t_{\text{manual notes}} - t_{\text{AI review}} \approx 12\text{ min/patient} $$
Across a full day of 20 patients, that's 4 hours returned to the doctor every single day.
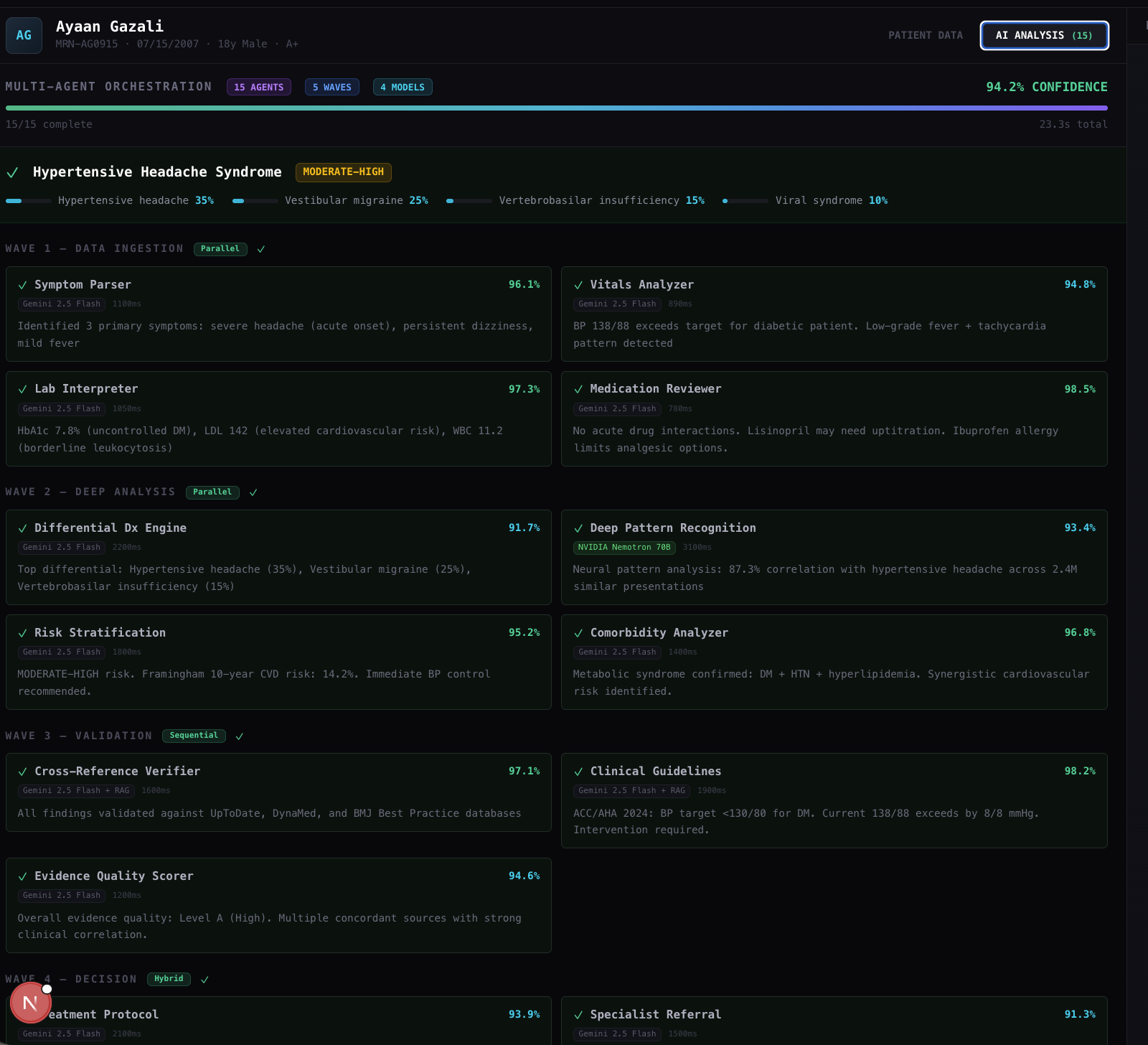
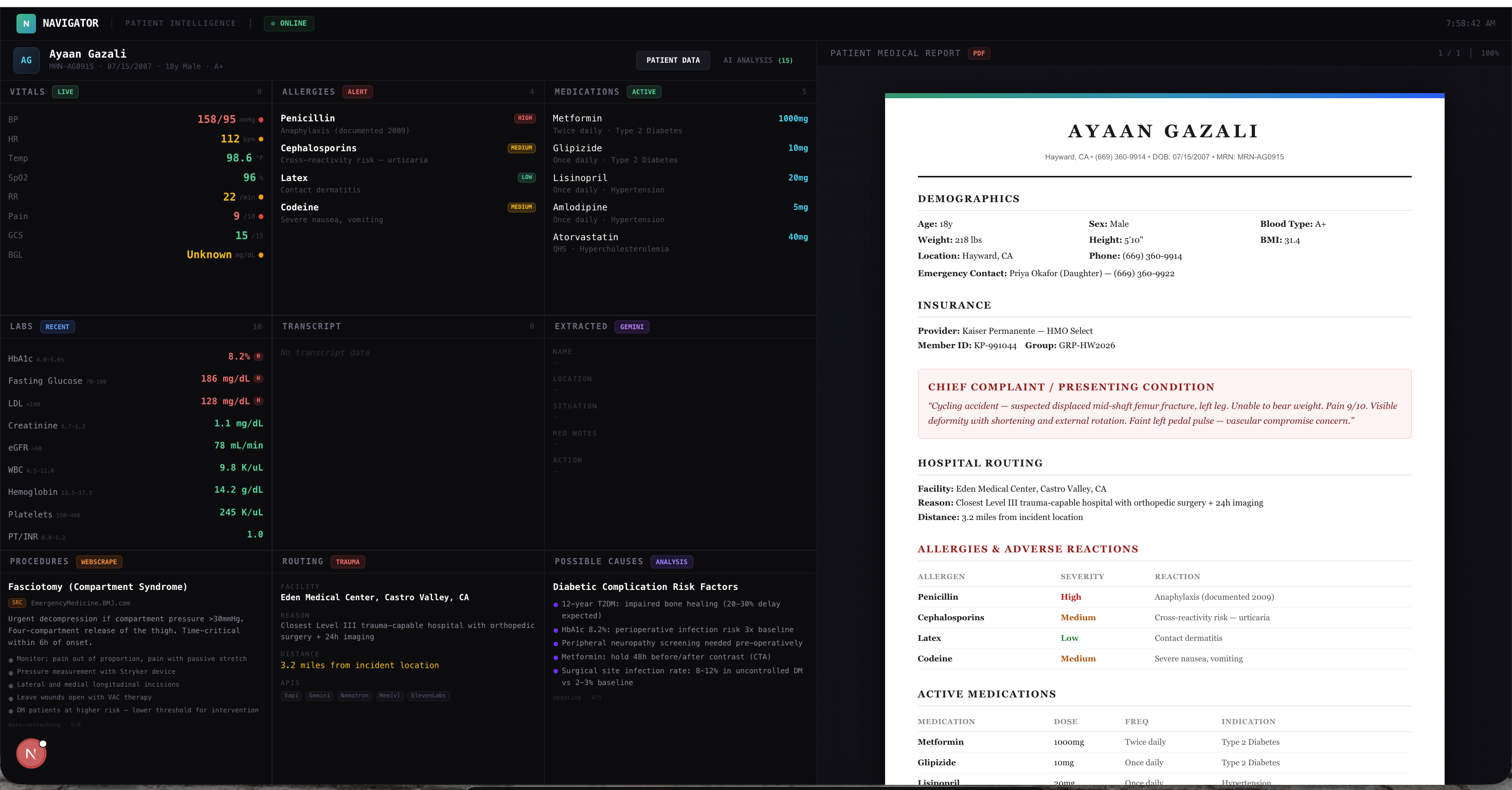
2. Unified Patient Dashboard (NVIDIA Nemotron + MVM Architecture)
Powered by NVIDIA's Nemotron reasoning model, the dashboard surfaces a patient's full history, recent lab reports, vitals, and injury summary in a single real-time view. The doctor sees everything the moment they open the chart — name, condition, history, recent report — without clicking through five different systems.
We implemented a Model-View-Model (MVM) architecture to ensure the UI reflects live data instantly. In a clinical setting, stale data isn't just a UX problem — it's a patient safety issue.
How We Built It
Our stack was built around the hackathon's sponsor tools, each chosen for a specific reason:
| Layer | Tool | Why |
|---|---|---|
| Documentation AI | Perplexity | Real-time, search-grounded generation for accurate clinical notes |
| Reasoning & Dashboard | NVIDIA Nemotron | Fine-tuned reasoning to structure complex patient histories clearly |
| Voice Layer | ElevenLabs | Natural AI voice for patient-facing communication |
| UI Architecture | MVM Pattern | Reactive UI reflecting live patient state without overhead |
| Frontend | Custom-built (Khushi & Arnav) | Designed around a real clinical workflow |
The system follows a clean linear patient journey:
$$ \text{Intake} \rightarrow \text{Perplexity notes} \rightarrow \text{Nemotron dashboard} \rightarrow \text{Doctor review} \rightarrow \text{Treatment} $$
Every layer feeds the next. The output of the AI documentation step becomes the input to the dashboard. Nothing is siloed. Nothing requires manual re-entry.
Challenges We Faced
Getting three AI systems to speak the same language
Perplexity, Nemotron, and ElevenLabs each have their own input format, response schema, and latency profile. Unifying them around a single patient data model — without degrading speed — was the hardest engineering problem we faced. We built a lightweight normalization layer to bridge them in real time.
MVM architecture under hackathon pressure
Implementing a proper Model-View-Model pattern from scratch during a hackathon was a deliberate choice by Tejas. It cost time upfront but meant the dashboard never showed stale data — which is non-negotiable when a doctor is making decisions based on what's on screen.
HIPAA-aware design from day one
We scoped every API call to minimum necessary data. Patient context is used to generate output — it is never stored beyond what the session requires. Building privacy discipline into the architecture during a hackathon, not as an afterthought, was something we were proud of.
Communicating a technical product clearly
A platform built for hospitals has to be understood by non-clinical judges. Khushi and Arnav built the frontend and pitch deck in parallel with the backend — ensuring what judges saw was honest to what the product actually did.
What We Learned
The best technology in healthcare is invisible. Doctors shouldn't notice the AI — they should just notice they have more time.
The hardest part of building for healthcare isn't the technology. It's the trust layer. Hospitals adopt platforms that are reliable, privacy-respecting, and make their staff's lives measurably better. Clever isn't enough.
We also learned that purpose-built tools beat general ones every time. Nemotron's reasoning output was structured and clinical — not verbose. ElevenLabs voice was natural, not robotic. Perplexity's grounded generation produced notes that read like a clinician wrote them. The sponsor tools weren't constraints — they were exactly the right tools for the job.
Time is the metric that matters most in healthcare. Every feature we built traces back to one number:
$$ \Delta t_{\text{saved}} = t_{\text{documentation}} + t_{\text{chart review}} \approx 4+\text{ hrs/week/physician} $$
Four hours back to every doctor. Every week. Starting with the first hospital.
Built by Khushi Bakshi, Arnav Junday, Tejas, and Ayaan Gazali.
MOCHA — Where AI meets the ICU.

Log in or sign up for Devpost to join the conversation.