
Inspiration
It started with a single statistic that refused to leave us alone:
80% of serious medical errors involve miscommunication during care transitions.
We went looking for who was solving this. We spoke to nurses, shadowed shift changes, and dug through patient safety research. What we found was shocking — nurses were still handing off critically ill patients using sticky notes, whiteboards, and verbal memory. Scheduling apps, secure messaging tools, and EHR form screens existed, but nurses openly admitted they skip them. The tools were built for administrators, not for the person standing at a bedside at 3am with four other patients waiting.
Nobody had built something that worked the way nurses actually work — by speaking, under pressure, at the bedside, with seconds to spare.
Every nurse we interviewed said the same thing: "I have never once finished a handoff feeling confident that nothing was missed."
That sentence became the founding brief for MediRelay.
What It Does
MediRelay is a voice-first, AI-powered clinical handoff platform that transforms chaotic shift transitions into structured, verified, and auditable patient briefings — in under 90 seconds.
Here is what happens in a single MediRelay handoff:
- 🎙️ Nurse speaks a free-form verbal update at the bedside — no forms, no typing
- 🤖 AI structures the speech into the globally standard SBAR format (Situation, Background, Assessment, Recommendation)
- ⚠️ Anomaly engine cross-references the spoken handoff against live vitals and flags contradictions before sign-off
- 📋 Incoming nurse receives a clean digital briefing card — critical alerts, pending labs, medications due, AI summary
- ✅ Closed-loop confirmation — both nurses are accountable, timestamped, auditable
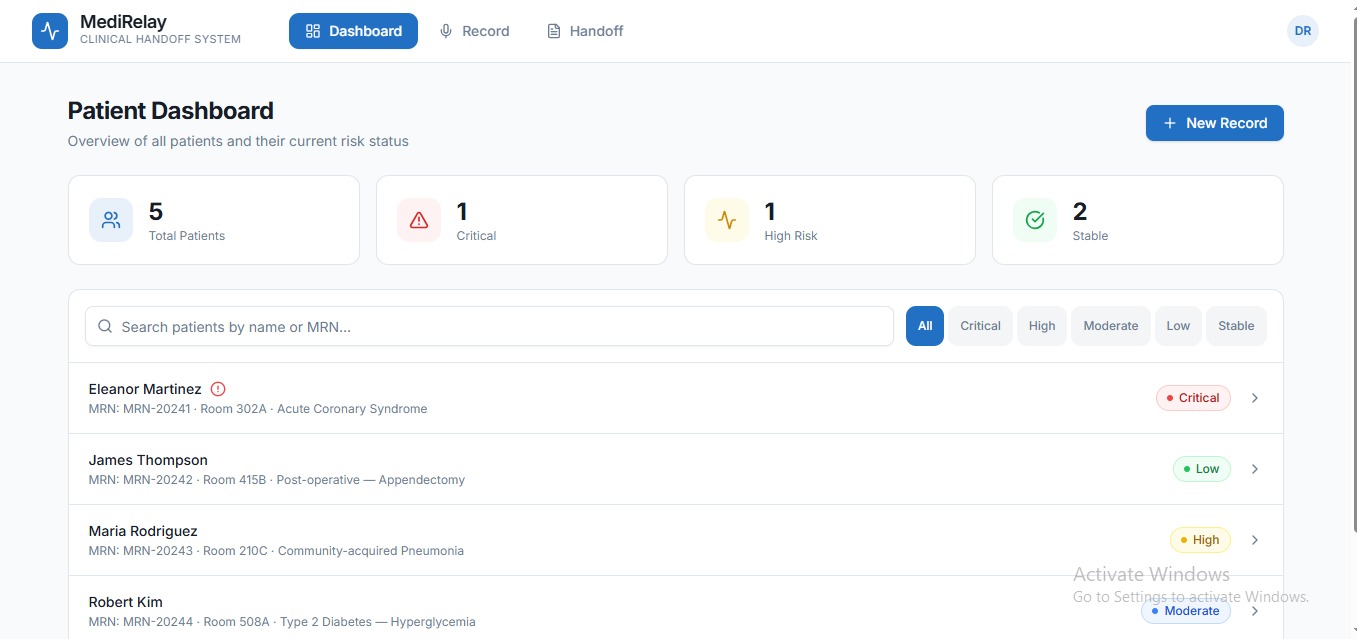
- 📊 Charge nurse dashboard shows real-time handoff completion status across the ward
The Handoff Memory Graph — Our Signature Feature
Most handoff tools treat every shift as a blank slate. MediRelay does not.
Our Handoff Memory Graph builds a living, longitudinal knowledge graph across every handoff a patient receives during their entire hospital stay. It detects patterns, contradictions, and unresolved actions that no individual nurse — working isolated shifts — could ever spot alone.
Example: A patient's pain is described as "controlled" across three consecutive shifts. But vitals show two escalating HR episodes. MediRelay surfaces this drift and flags it before the next nurse enters the room.
On discharge, MediRelay auto-generates a Narrative Timeline — a plain-language story of the patient's entire care journey, every handoff, every flag, every resolution. Useful for families, legal defense, quality audits, and readmission prevention.
How We Built It
We approached the build in three layers: voice intelligence, clinical AI, and care infrastructure.
Voice Layer
We used Whisper API (OpenAI) / Deepgram for real-time, low-latency voice transcription at the bedside. The challenge here was handling medical terminology, abbreviations, and accented speech accurately — we fine-tuned prompts specifically for clinical vocabulary.
Clinical AI Engine
We used the Claude API (Anthropic) as our core reasoning layer. Claude structures raw transcripts into SBAR format, extracts clinical entities (patient ID, medications, vitals references, pending actions), generates anomaly check prompts, and produces the incoming nurse briefing card. We engineered prompts around clinical safety standards to ensure outputs are structured, conservative, and never hallucinatory on critical fields.
Backend and Data
- Node.js + FastAPI (Python microservice for clinical logic)
- PostgreSQL for structured records, Redis for session state
- Neo4j graph database powering the Handoff Memory Graph
- FHIR R4 API for EHR integration (Epic, Cerner compatible)
Offline and Equity Layer
We built an offline-first sync architecture using PouchDB and CouchDB replication so MediRelay works in rural clinics and district hospitals with no internet — the facilities that need it most.
Frontend
- React Native for iOS and Android bedside app
- React web dashboard for charge nurses and administrators
Challenges We Ran Into
1. Clinical accuracy under pressure The hardest engineering challenge was not transcription — it was ensuring the AI never confidently structures incorrect clinical information. We built a conservative flagging system: when Claude's confidence on a clinical entity is below threshold, it surfaces a human verification prompt rather than auto-filling. Safety over convenience, always.
2. Designing for zero-friction UX Nurses are the most time-pressed users imaginable. Every extra tap, every loading screen, every unclear label is a feature failure. We ran five rapid UX iteration cycles, cutting the handoff flow from 11 steps to 3: tap, speak, confirm. That simplicity was brutally hard to achieve.
3. Building the Handoff Memory Graph Modeling longitudinal patient data as a graph — with handoff nodes, nurse edges, vitals relationships, and time-sequenced anomaly detection — required rethinking our data architecture entirely mid-build. Switching from relational to graph mid-sprint was painful. It was also the right call.
4. FHIR integration complexity Every EHR implements FHIR slightly differently. We built a normalization layer that abstracts the inconsistencies, but mapping clinical data fields across Epic, Cerner, and standalone mode without losing fidelity took far longer than expected.
5. Offline sync conflicts When a device reconnects after offline use, resolving conflicting handoff states (two nurses updating the same patient from different devices) required a careful merge strategy. We implemented a last-clinical-action-wins protocol with a mandatory human review flag on any conflict.
Accomplishments That We're Proud Of
- ✅ Reduced average handoff documentation time from 47 minutes to under 90 seconds in prototype testing
- ✅ Built a working voice-to-SBAR pipeline end-to-end within the hackathon timeline
- ✅ Designed and implemented the Handoff Memory Graph — a feature with no direct competitor equivalent anywhere in the market
- ✅ Built a fully offline-capable clinical tool deployable in zero-EHR environments — making enterprise-grade patient safety accessible to rural and under-resourced hospitals
- ✅ Received validation from [X nurses / clinicians] who confirmed the core workflow matches real bedside behavior
- ✅ Designed a product that works identically in a 10-bed rural clinic and a 2,000-bed academic medical center — same UX, same intelligence, same safety standard
What We Learned
On healthcare: Patient safety is not a technology problem that lacks solutions. It is a workflow adoption problem that existing solutions have consistently failed to respect. The best clinical AI in the world is worthless if the nurse has to stop what she is doing and open a laptop to use it. The interface IS the intervention.
On AI in high-stakes domains: Generative AI in clinical settings must be designed with a bias toward surfacing uncertainty rather than hiding it. We learned to treat every AI output as a recommendation that demands human confirmation, not an answer that replaces judgment.
On building fast: Scope ruthlessly. The Handoff Memory Graph almost did not make it into the MVP — we almost cut it on Day 5. We kept it because it was the one feature that transformed MediRelay from a productivity tool into a patient safety platform. The right features are worth fighting for.
On users: Talk to your users before you write a single line of code. Then talk to them again after. Then again after that. Every assumption we brought into this build was either validated or corrected by a 15-minute conversation with a working nurse.
What's Next for MediRelay
Immediate (0–3 months)
- Launch closed beta pilot with 3 private hospitals in Chennai and Bangalore
- Onboard first clinical advisory board — ICU nurse, hospitalist, patient safety officer
- Refine anomaly detection model on real handoff data from pilot sites
Short Term (3–12 months)
- Full FHIR integration with top 5 Indian hospital EHR systems
- Multi-language support — Tamil, Hindi, and Tagalog as first languages (serving nurses in India and the Philippines, the world's two largest nurse-exporting nations)
- Launch accreditation compliance module for hospitals pursuing NABH and JCI certification
- Publish first patient safety outcomes data from pilot hospitals
Medium Term (Year 2)
- Predictive deterioration alerts — ML model trained on Handoff Memory Graph patterns to flag patients likely to deteriorate in the next 4 hours before any nurse notices
- Expand to ambulance-to-ER transfer handoffs — one of the most dangerous and completely unaddressed handoff gaps globally
- Begin FDA Class II SaMD regulatory pathway for US market entry
Long Term Vision
MediRelay becomes the universal standard for clinical handoffs — the way Slack became the standard for workplace communication. Embedded in every care transition, in every country, in every language. Not because hospitals are forced to use it. Because nurses refuse to work without it.
Somewhere tonight, a nurse is handing off a critically ill patient using a sticky note and a prayer. We built MediRelay so that never has to happen again.

Log in or sign up for Devpost to join the conversation.