-
-

Header
-
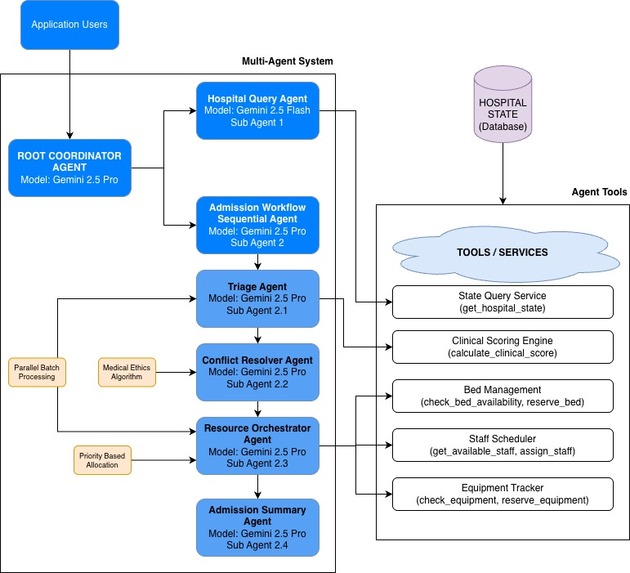
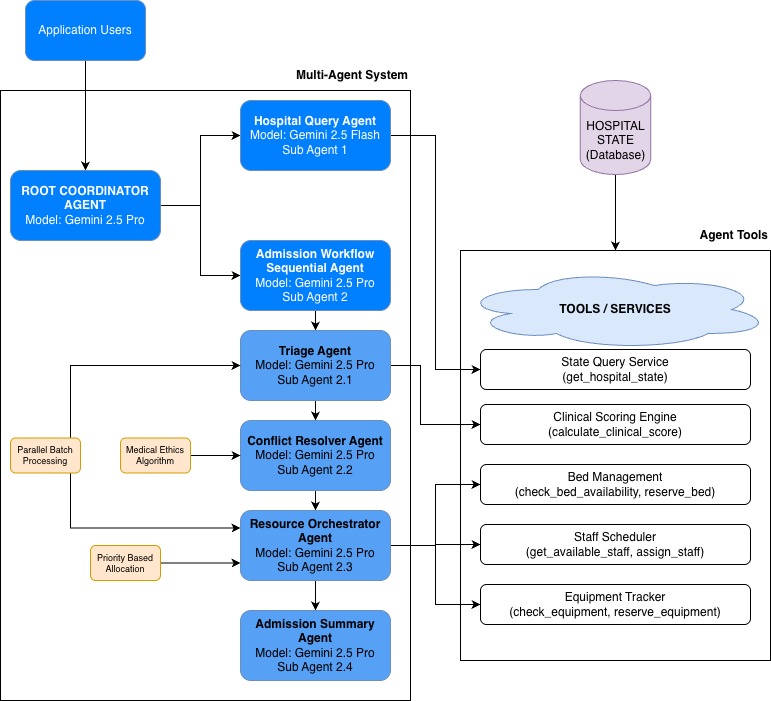
Architecture Diagram
-
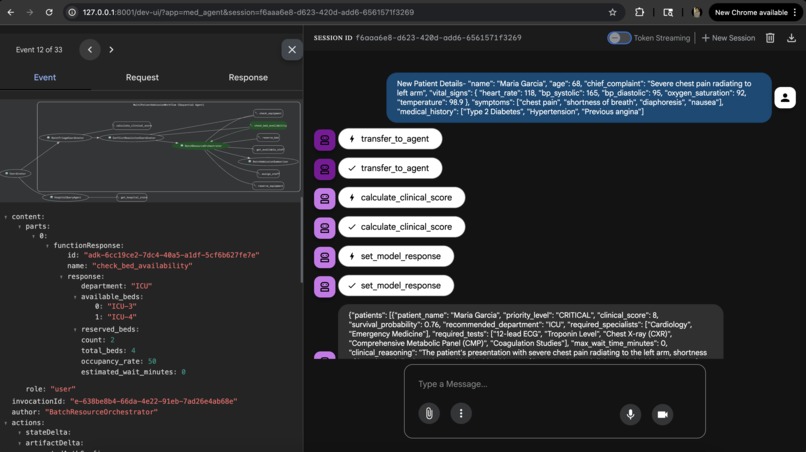
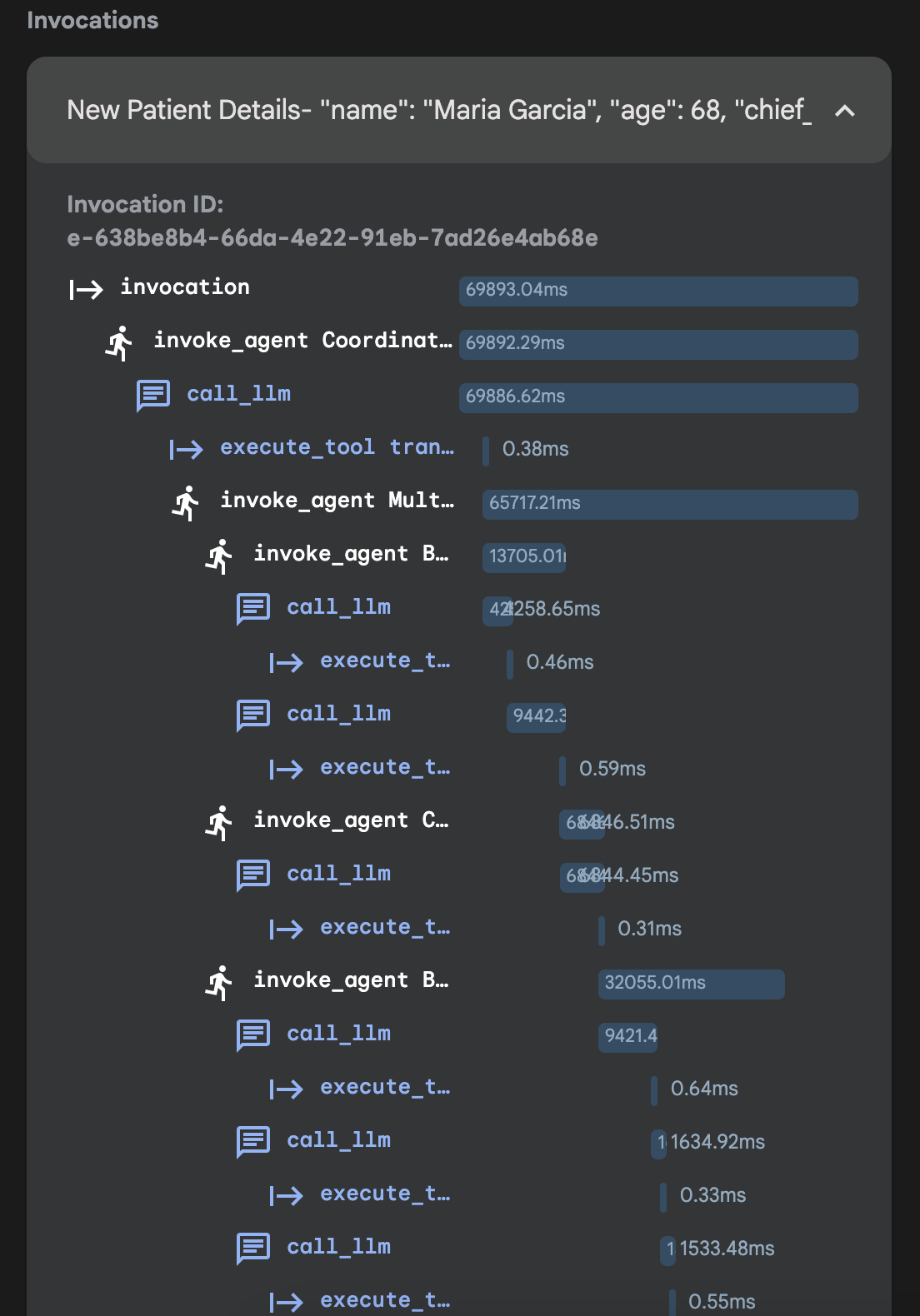
Sample 3
-
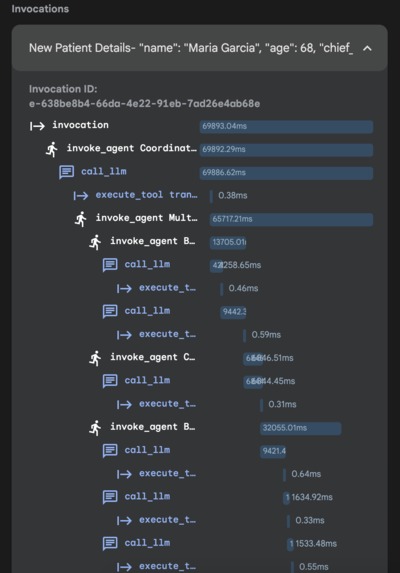
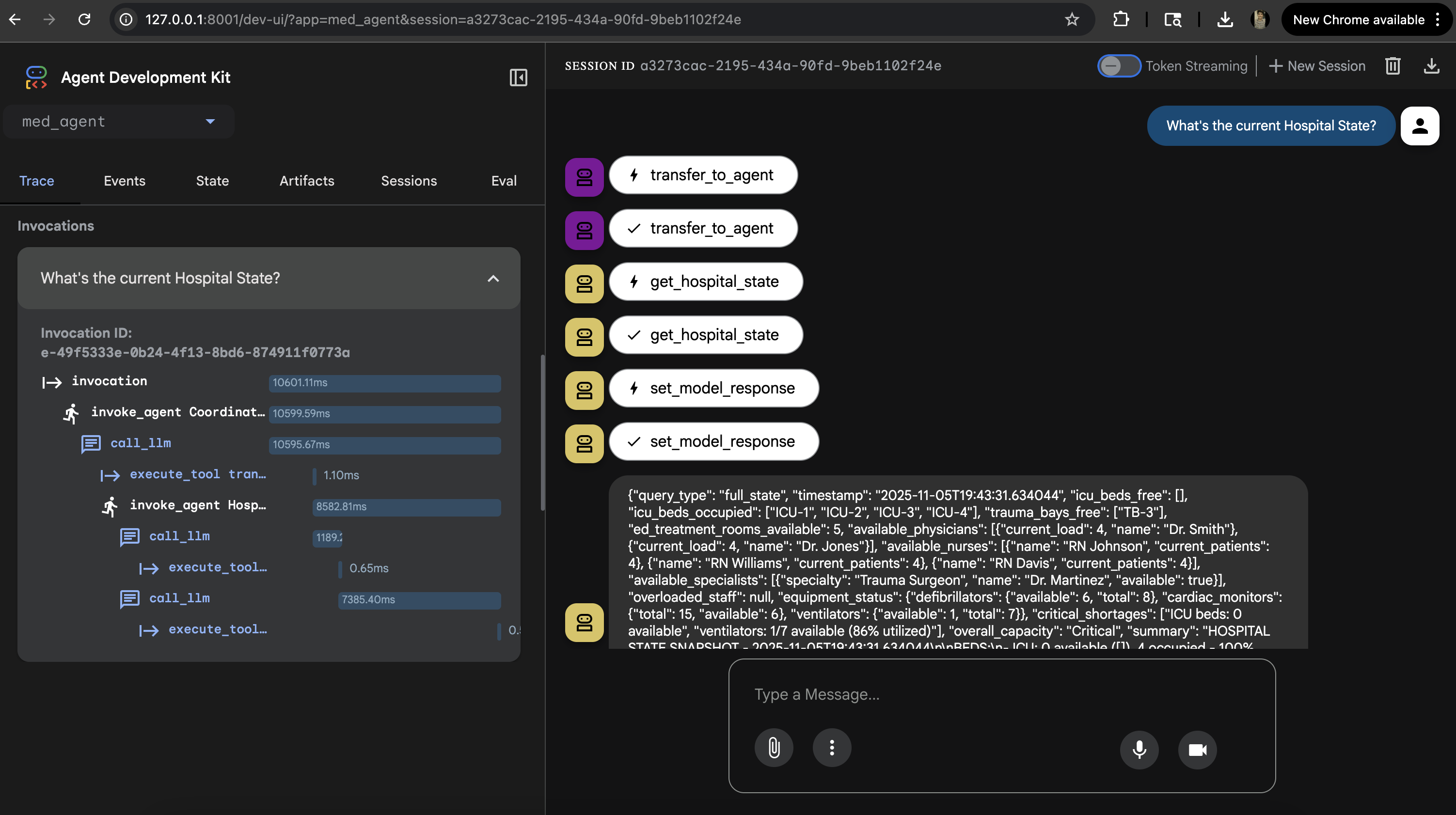
Sample 2
-
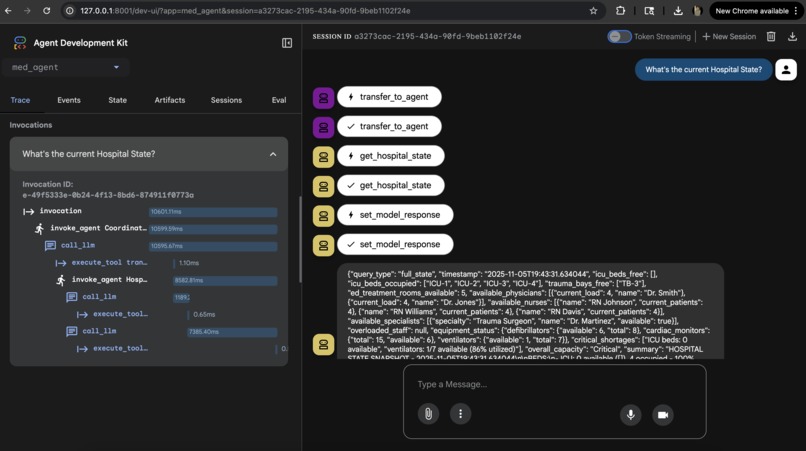
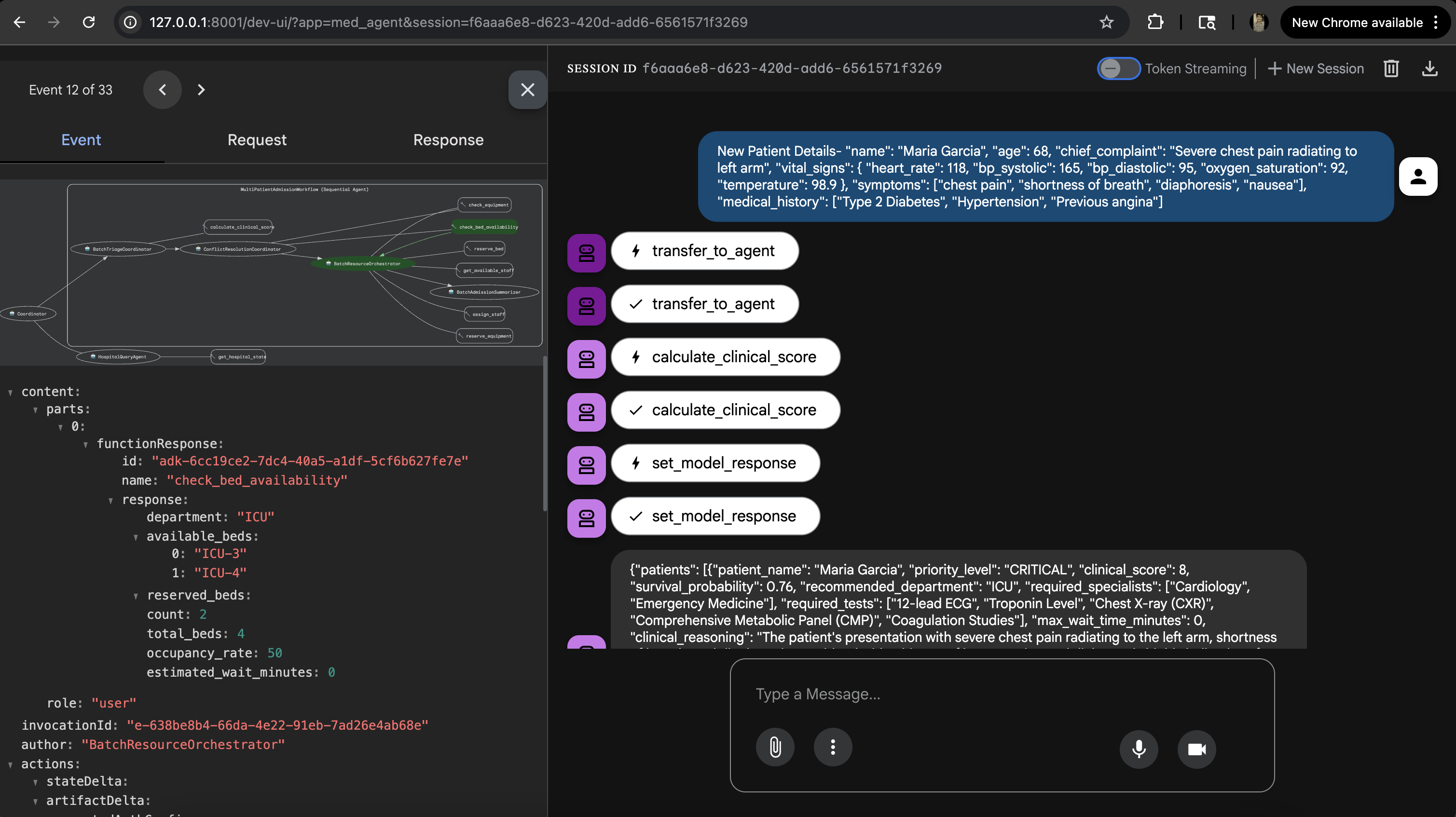
Sample 1

Inspiration for MedFlow
The genesis of MedFlow lies in a severe operational bottleneck in emergency medicine:
- Nearly 5% of emergency department (ED) patients now wait 24+ hours for a hospital bed (University of Michigan, 2024).
- During mass casualty events, manual triage takes 60–110 minutes with only 65% accuracy under stress.
"What if AI could make these life-or-death decisions in minutes, with transparent medical ethics and zero human bias?"
With 139.8 million ED visits in 2024 and a projected 28% increase in elderly patient volume over the next decade, emergency departments desperately need intelligent automation. MedFlow was born from the belief that AI should handle the impossible: simultaneous triage of multiple critical patients with instant, ethical resource conflict resolution.
What MedFlow Does: Core Capabilities
MedFlow is a multi-agent AI system that orchestrates emergency department admissions at superhuman speed.
1. Batch Triage Intelligence
- Simultaneously assesses unlimited patients using APACHE-like clinical scoring.
- Evaluates vital signs, symptoms, and medical history in parallel.
- Assigns priority levels (CRITICAL vs NON_URGENT) with survival probabilities.
- Recommends departments, required specialists, and safe wait times.
2. Automated Conflict Resolution
- Detects resource shortages (ICU beds, ventilators, specialists).
- Applies medical ethics principles: "greatest good for greatest number."
- Prioritizes patients based on clinical severity, survival probability, and time sensitivity.
- Documents every decision with transparent medical reasoning.
3. Intelligent Resource Allocation
- Processes patients in priority order (highest first).
- Reserves beds, assigns least-busy staff, and allocates equipment.
- Updates hospital state in real-time.
- Prevents double-booking and resource conflicts.
4. Executive Summaries & Hospital State Queries
- Executive Summaries: Generates leadership reports for rapid decision-making, tracking admitted vs. waiting patients and providing next actions for care teams.
- Hospital State Queries: Real-time capacity monitoring. Examples: "Which ICU beds are free?", "Who are the least busy physicians?", "What's our current equipment availability?"
How MedFlow Was Built
Tech Stack:
- Google Agent Development Kit (ADK): Multi-agent orchestration framework.
- Gemini 2.5 Pro: Used by specialized AI agents for complex medical reasoning.
- Gemini 2.5 Flash: Used as a Fast Query Agent for hospital state monitoring.
- Python + Pydantic: For type-safe schemas and data validation.
- Custom Medical Tools: Clinical scoring algorithms, resource management.
Key Implementation Decisions:
- Batch Processing Over Sequential: Designed agents to handle entire patient arrays simultaneously for true parallel triage.
- Separation of Concerns: Each agent has one job.
- Context Passing: Agent outputs (e.g.,
{batch_triage},{conflict_resolution}) explicitly become the next agent's input, forming a data pipeline. - Real-time State Management: Built an in-memory hospital state database that tracks bed status, staff workload, and equipment availability, updated atomically by resource tools.
- Medical Ethics as Code: Conflict resolution is implemented using established triage principles.
Tools Built:
calculate_clinical_score(): APACHE-II inspired severity scoring.check_bed_availability(): Real-time capacity queries.reserve_bed(): Atomic resource locking.assign_staff(): Workload-optimized staff allocation.get_hospital_state(): Full system state snapshots.
Challenges Encountered & Solutions
| Challenge | Problem Description | Solution/Learning |
|---|---|---|
| Agent Context Management | Agents "forgot" previous decisions; the resource orchestrator couldn't see triage results. | Implemented strict output_key naming and explicit context passing in agent instructions. Multi-agent systems need explicit data contracts. |
| Conflict Detection Logic | Initial resolver only checked availability, missing cases where beds were reserved by higher-priority patients. | Added reservation status tracking (available, occupied, reserved). Resolver checks both availability AND reservation status. |
| Race Conditions | Double-booking of resources when processing multiple patients in parallel. | Implemented strict sequential processing based on the allocation_order from the conflict resolver. |
| Speed vs. Reasoning Quality | Gemini Flash was fast (1 sec) but poor medically; Gemini Pro was slower (3-4 sec) but clinically sound. | Hybrid Approach: Flash for simple queries (state), Pro for critical decisions (triage, conflict resolution). Accepted 50-90 seconds, still 60x faster than humans. |
| Prompt Engineering for Medical Ethics | Initial prompts produced ethically questionable prioritizations (e.g., always prioritizing younger patients). | Embedded explicit medical ethics principles in prompts: "Apply greatest good for greatest number," "Prioritize survival probability WITH intervention." |
| Testing Mass Casualty | Hard to validate correctness without "ground truth." | Created test cases based on published mass casualty case studies. Built audit trails showing full decision reasoning for human review. |
Accomplishments & Learnings
Accomplishments We're Proud Of
- Real-World Impact Potential: Built a production-ready system with 90% time savings over manual triage. MedFlow could process an 8-patient bus crash faster than a human could triage the first patient.
- Solved an "Impossible" Problem: Successfully automated resource conflict resolution, a problem requiring medical expertise, ethical reasoning, and real-time data, with transparent, auditable decision-making.
- Multi-Agent Architecture Mastery: Successfully implemented a 4-agent sequential pipeline, requiring deep understanding of context management and agent orchestration.
- Medical Ethics in Code: Translated abstract principles into concrete algorithms, ensuring the conflict resolver explains WHY each decision was made, creating accountability.
Key Learnings
- Multi-agent systems need explicit data contracts and careful context management.
- LLMs can do medical reasoning with the right scaffolding: Structured outputs (Pydantic), Tool calling, and focused Prompt Engineering.
- Google ADK requires discipline regarding
output_key, context variables, and explicit agent instructions.
What's Next for MedFlow
Immediate Next Steps (3 months):
- Clinical Validation Study: Partner with EDs to compare MedFlow decisions vs. experienced triage nurses.
- EHR Integration: HL7 FHIR API for real-time patient data ingestion and bidirectional sync with Epic, Cerner, etc.
- Real-time Dashboard: Web UI for hospital administrators with live capacity monitoring and patient flow visualization.
Mid-term Goals (6-12 months):
- Predictive Capacity Planning: ML models to forecast ED surge times ("You'll run out of ICU beds in 2 hours") and recommend proactive staff scheduling.
- Inter-hospital Coordination: Multi-facility resource sharing and regional disaster response coordination.
Long-term Vision (1-3 years):
- Autonomous Emergency Department: Full workflow automation from admission to discharge.
- Global Disaster Response Network: Deploy MedFlow to humanitarian crises in partnership with organizations like the WHO and Red Cross.
- Continuous Learning System: Learn from outcomes to adapt scoring algorithms based on regional disease patterns.
- Regulatory Approval: Seek FDA 510(k) clearance as clinical decision support software and obtain HIPAA/SOC 2 compliance.
Built With
- adk
- agent
- google-cloud
- json
- llm
- machine-learning
- pydantic
- python

Log in or sign up for Devpost to join the conversation.