-
-
architecture
-
workflow
Inspiration
Every year 2.3 million newborns die within 28 days of birth — about three-quarters in sub-Saharan Africa and South Asia, and three-quarters within the first week. Most of these deaths are preventable, and the bottleneck usually isn't medicine — it's detection. The WHO IMNCI protocol defines a systematic newborn danger-sign assessment, but in the field a community health worker (CHW) is often the only health contact a baby gets: trained knowledge decays, there's no diagnostic equipment, and a paper checklist can't calculate a dose or reason over a photo. Field studies put CHW danger-sign sensitivity anywhere from 33% to 91%.
The cruel twist is that the places where this matters most are exactly the ones with no reliable internet. A cloud-only medical agent abandons those babies; a purely offline one leaves the cloud's best multimodal reasoning on the table. That tension is the whole reason EdgeAgent is the right track for this problem — and why I built LUMEN to be both, and to switch between them automatically.
What it does
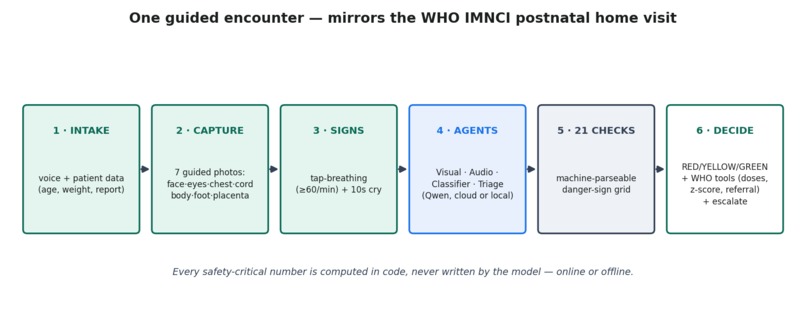
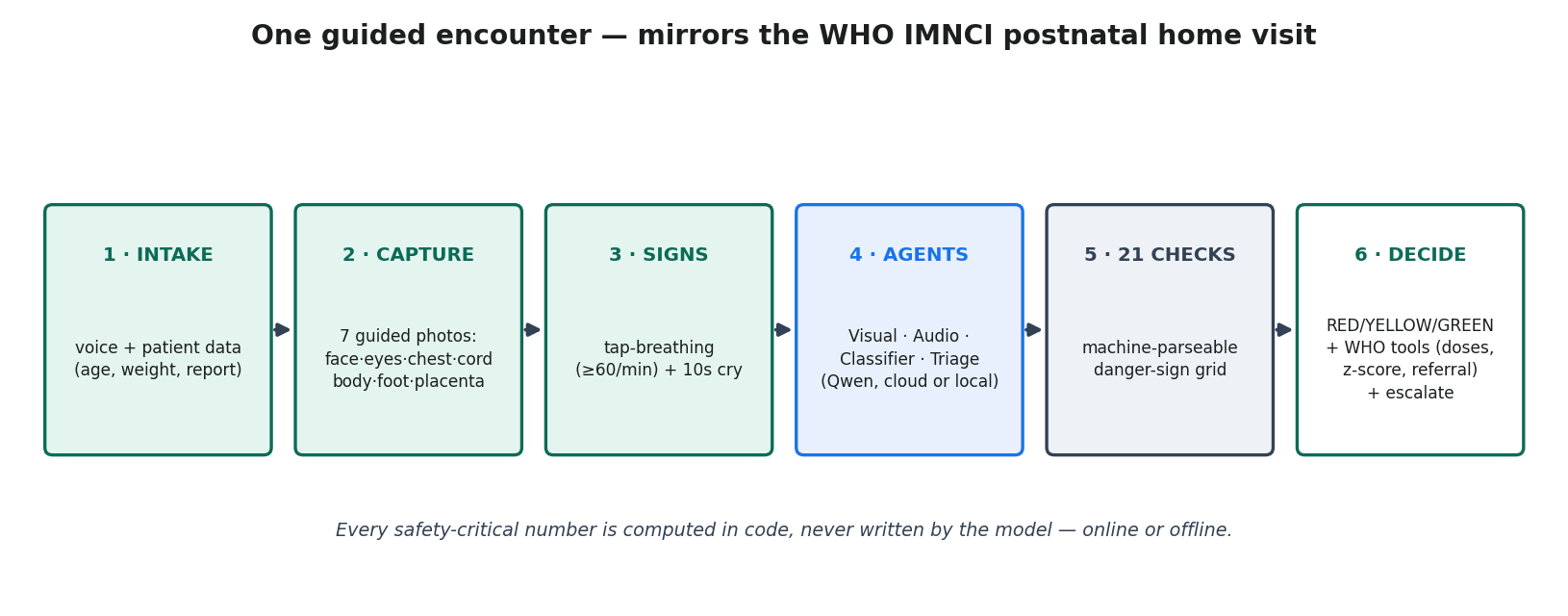
LUMEN turns the phone or laptop a CHW already carries into an AI neonatal specialist that follows the WHO postnatal home-visit workflow end to end.
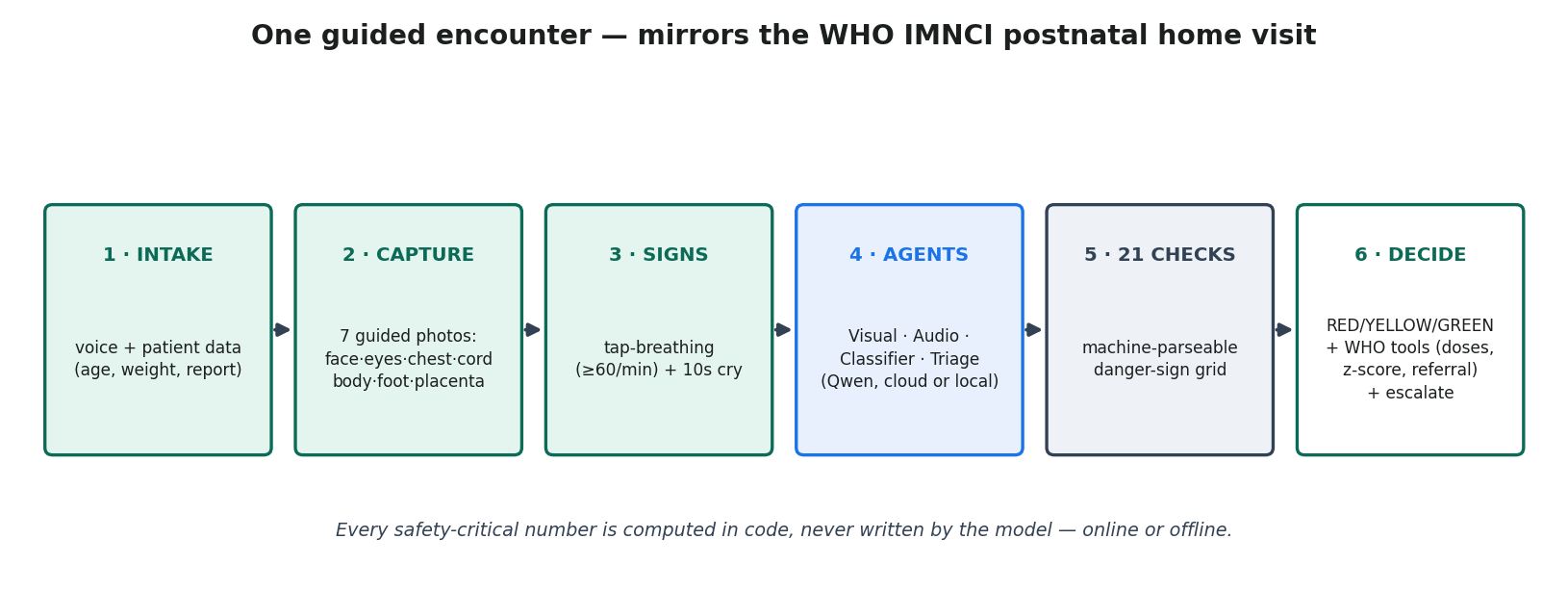
A single guided encounter collects voice intake (in 12 languages), a camera-guided 7-capture visual exam (face, eyes, chest, umbilicus, full body, foot sole, optionally placenta), a tap-to-count respiratory measure, and a 10-second cry recording. From those inputs it produces 21 structured danger-sign checks, a WHO IMNCI classification with a RED / YELLOW / GREEN traffic light, an action plan with exact medication doses, a referral letter, and a follow-up date — and it escalates RED/YELLOW cases to a supervisor queue for human sign-off. Encounters are stored locally and sync to the cloud when the network returns, so the worker is never blocked and the record always arrives.
Crucially, every safety-critical number is computed in code, not written by the model — online or offline.
How we built it
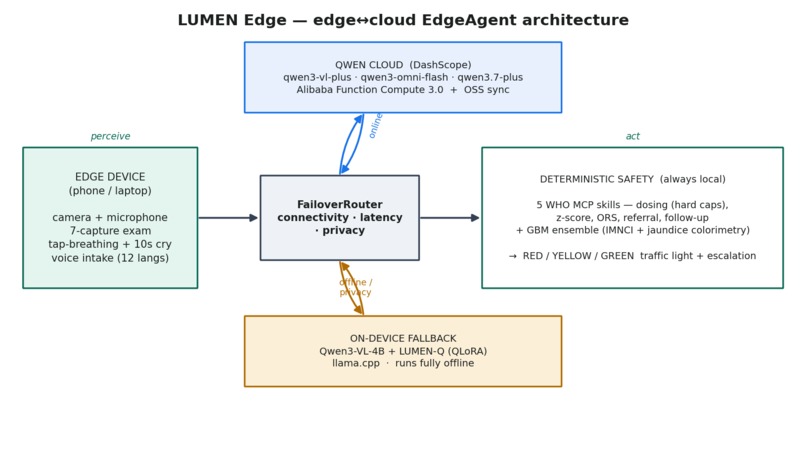
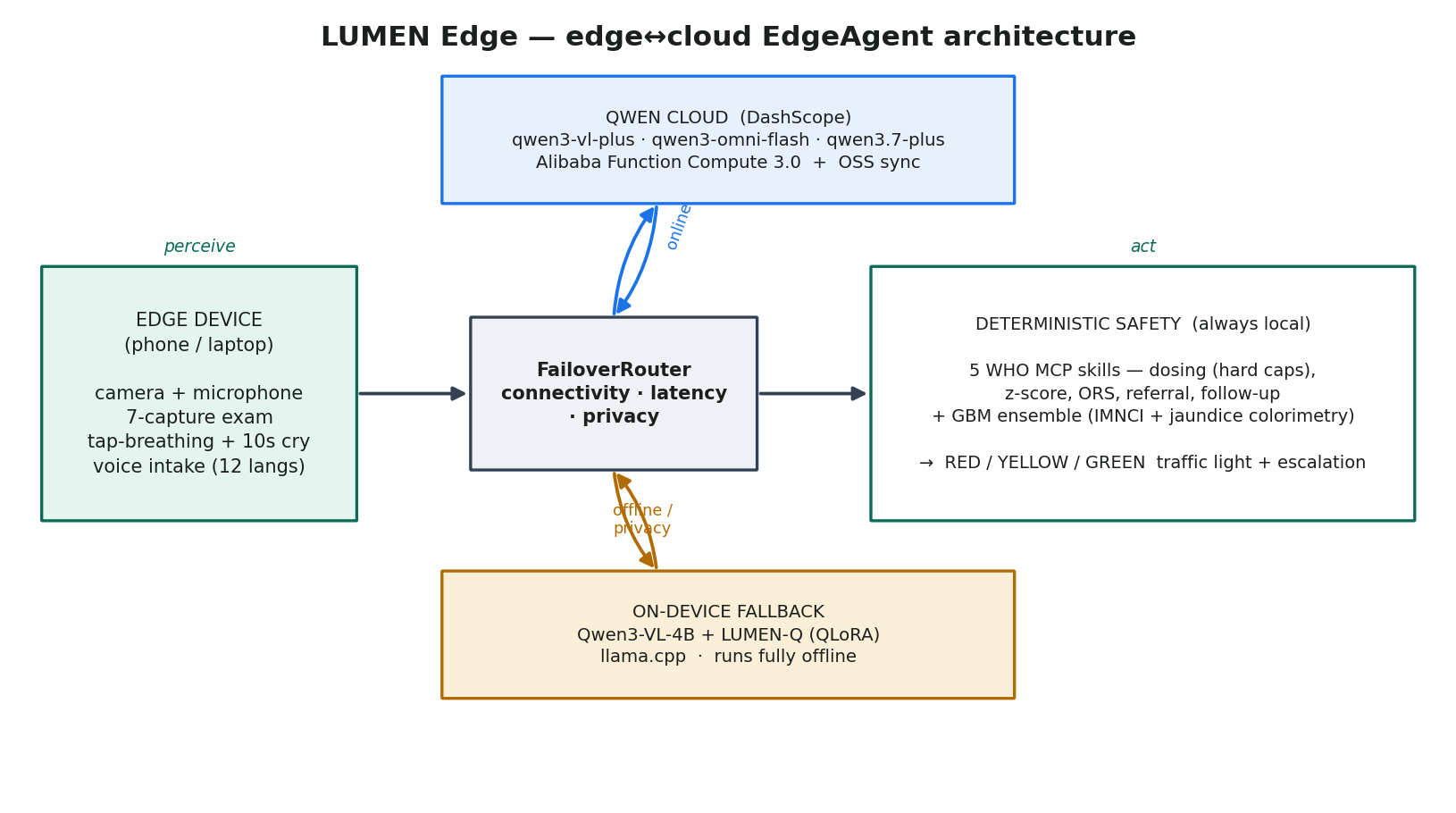
LUMEN is one provider interface with two backends — Qwen Cloud and a local model — behind a FailoverRouter that picks per request on connectivity, latency, and a privacy flag.
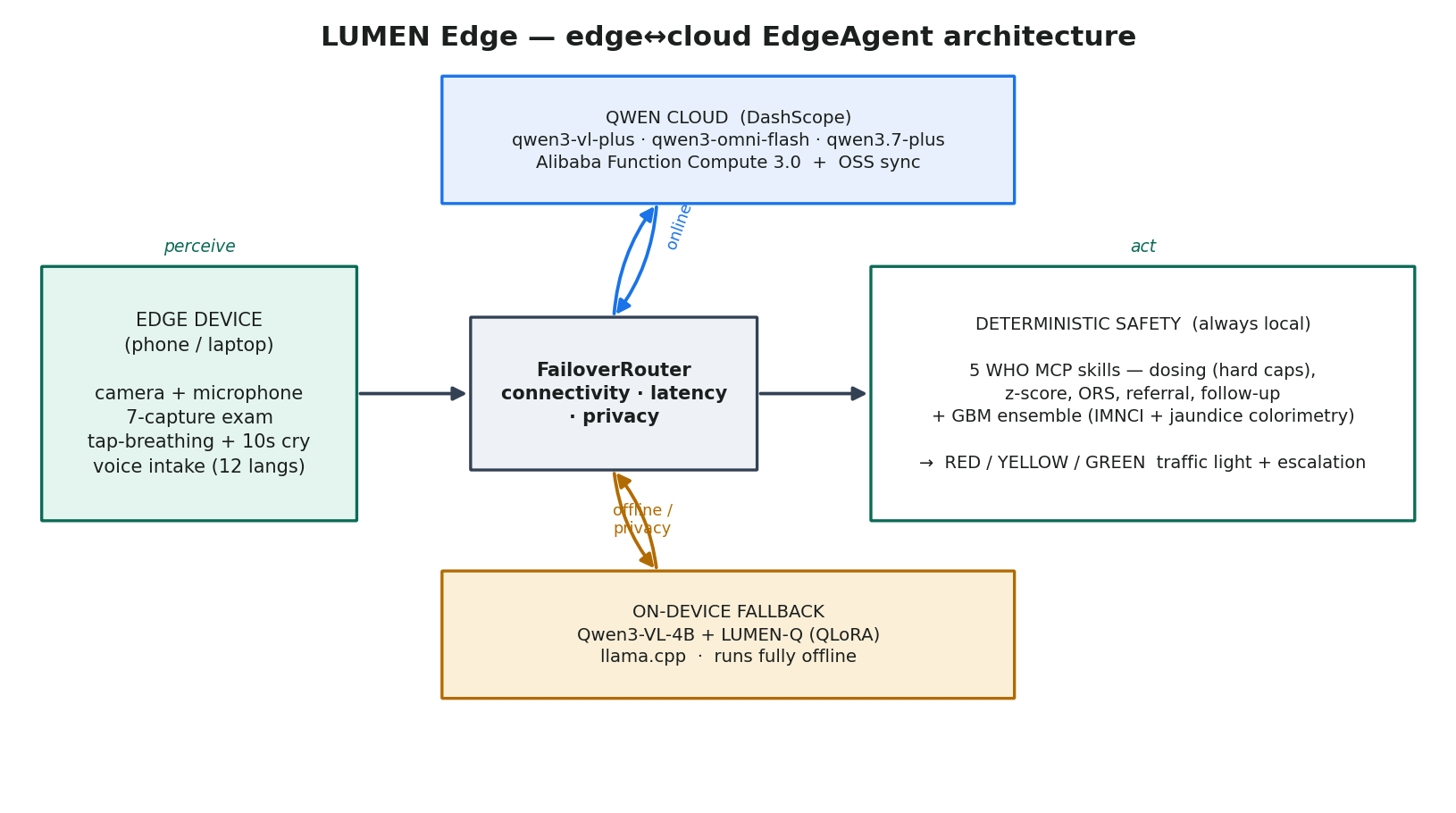
Cloud reasoning uses the best-fit Qwen flagship per stage through DashScope: qwen3-vl-plus for the visual exam, qwen3-omni-flash for native cry-audio understanding, and qwen3.7-plus for agentic synthesis. The assessment runs as a small society of specialist agents — Visual, Audio, Classifier, Triage, plus a MemoryAgent that recalls prior visits — orchestrated with Qwen-Agent. The five deterministic WHO skills (dosing with hard caps, weight-for-age z-score, ORS volume, referral letter, follow-up) are exposed over MCP, so the model decides which tool to call and the tool decides the number.
The offline brain is Qwen3-VL-4B-Instruct, fine-tuned with QLoRA on a single RTX 4070 into LUMEN-Q — a two-stage recipe (text IMNCI, then vision jaundice/skin-tone) over the same neonatal corpus the cloud path is calibrated against — then exported to a quantized GGUF and run through llama.cpp's multimodal mtmd API. A calibrated LightGBM ensemble (an IMNCI head + a CIE-Lab jaundice-colorimetry head) supplies the safety-critical traffic light in both modes.
The same FastAPI image deploys to Alibaba Function Compute 3.0, with encounters synced to OSS; a native Android build runs the identical edge↔cloud logic on a phone, with on-device inference through a C++/JNI llama.cpp bridge.
Challenges we ran into
- The offline model had to be clinically trustworthy, not just present. A stock 4B vision model is unreliable on neonatal imagery, so fine-tuning wasn't optional — it was the EdgeAgent thesis. Getting the two-stage QLoRA recipe to run on 12 GB (and fixing a real dataset-pipeline bug along the way) took the most iteration.
- Class imbalance is dangerous here. Severe jaundice is ~1% of the data, and the fine-tuned model still under-grades the rarest, most critical cases. Rather than hide that, I made the deterministic IMNCI rules + jaundice colorimetry, not the LLM, own the safety-critical decision.
- Cloud and local have to behave identically or failover isn't safe — so both share one tested streaming/tool-call core, and the traffic light is decided the same way in every path.
- A hallucinated paediatric dose can kill. Designing the MCP boundary so the model never writes a number — only requests a tool — was a deliberate constraint, not an afterthought.
- Porting to a real standalone Android app (native llama.cpp
mtmdfor Qwen3-VL, edge↔cloud routing, an in-app Qwen-API option) on top of the laptop build.
Accomplishments that we're proud of
- A working edge↔cloud failover, not a slide: the same encounter completes on Qwen Cloud or on-device, with an honest badge showing which ran.
- Safety by construction — every dose hard-capped in code, "when in doubt, refer," an explicit disclaimer on every output, and supervisor escalation.
- It really runs offline and on a phone: a fine-tuned multimodal Qwen3-VL in a quantized GGUF, plus a standalone native Android app, in 12 languages.
What we learned
- A small, targeted fine-tune buys enormous reliability even when it doesn't ace every class — going from 65% to 100% parseable clinical answers matters more in the field than a few accuracy points.
- But a fine-tune won't fix a rare class on its own; the lesson reinforced is that the trustworthy design is hybrid — the LLM reasons and explains, deterministic code decides anything that can hurt a baby.
- Designing for cloud↔local parity from day one (one provider interface, one streaming core) is what makes graceful degradation actually graceful.
- Qwen3-VL runs genuinely well on-device through llama.cpp
mtmd, which makes the offline half of an EdgeAgent realistic rather than aspirational.
What's next for Lumen - AI neonatal specialist
- Field pilots on low-cost Android with CHW partners, and the Qwen-ecosystem-native MNN runtime as a second on-device engine.
- Extend the same edge↔cloud pattern across childhood IMNCI — pneumonia, malnutrition, dehydration, and malaria — since the architecture is condition-agnostic.
- Clinical validation toward a real deployment. The code is open and the weights are published, because these babies can't wait.

Log in or sign up for Devpost to join the conversation.