-

ISPS-VETA - Crew Psychologist-Psychiatrist
-
-
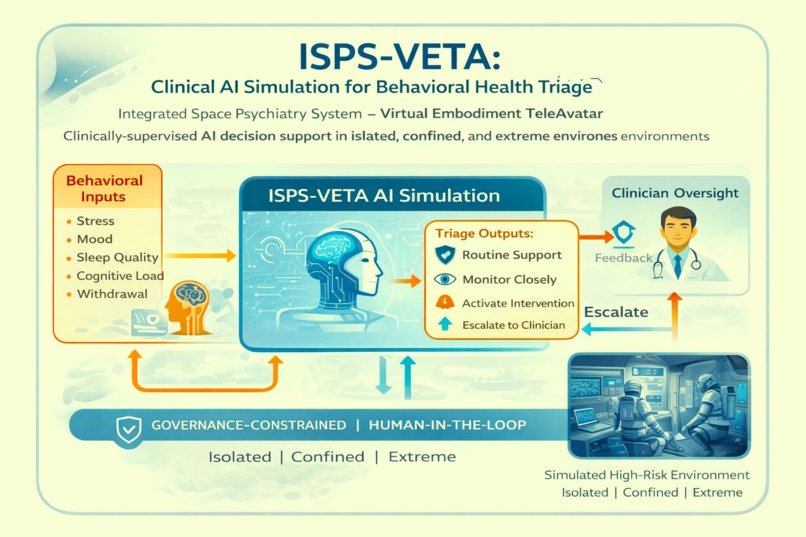

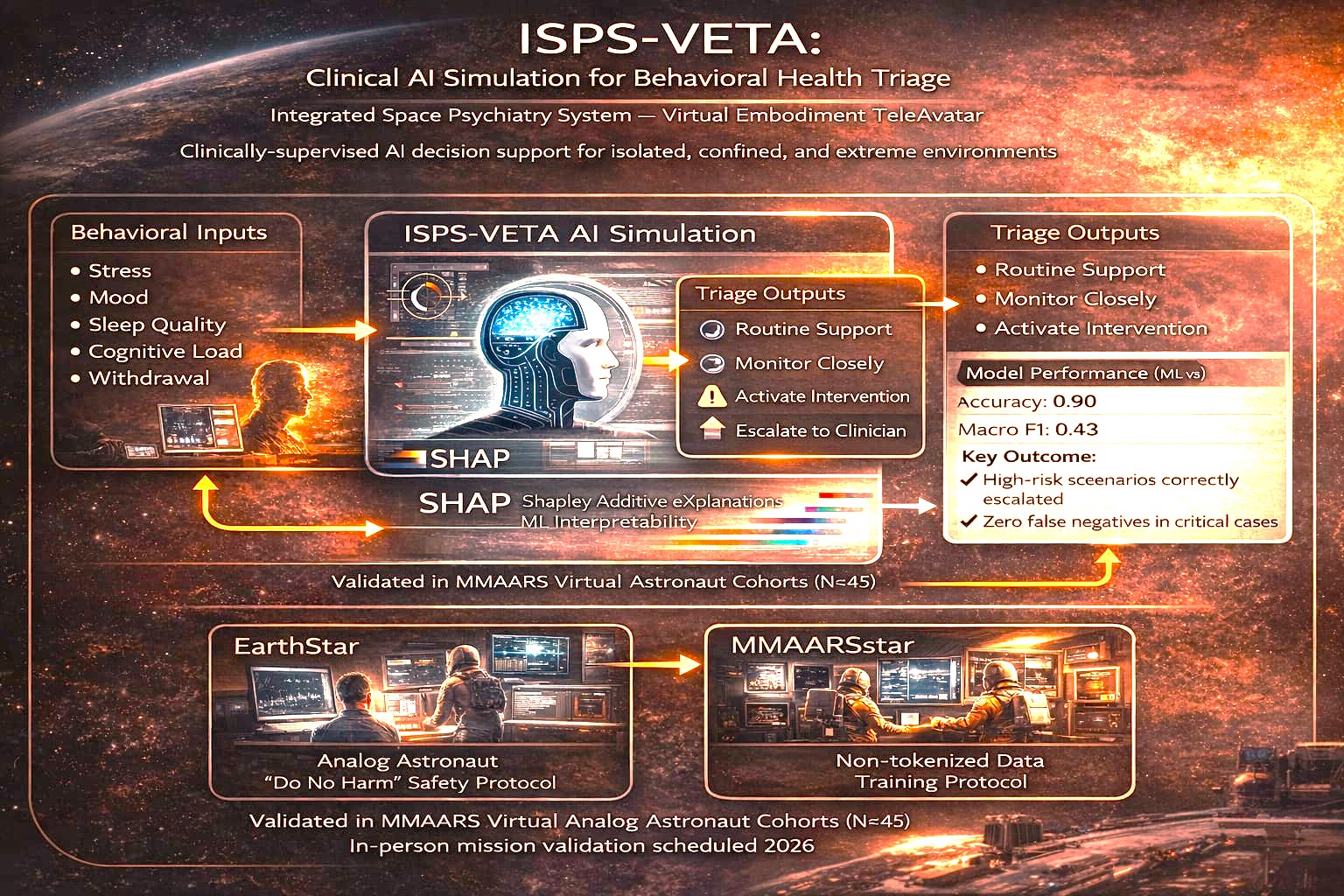
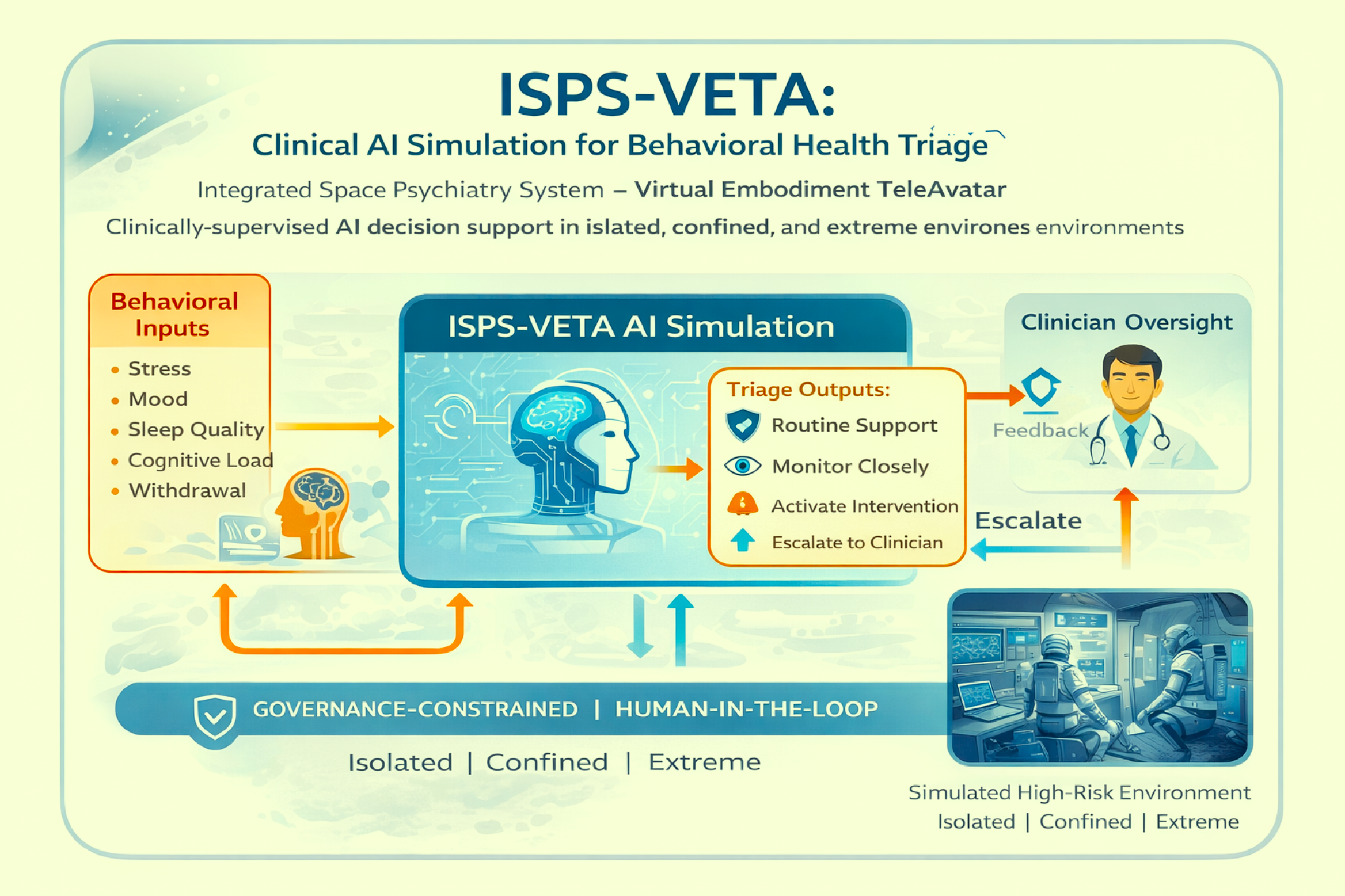
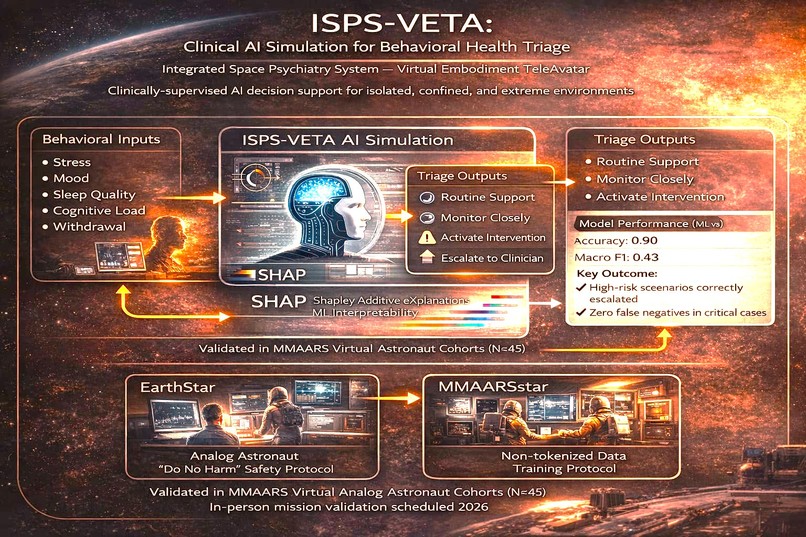
WHAT IT DOES: ISPS-VETA (Integrated Space Psychiatry System – Virtual Embodiment TeleAvatar) is a pilot clinical AI simulation that explores how structured behavioral and cognitive inputs can be used to support safe triage decisions in high-risk environments. The system is designed to detect potential distress patterns and map them to bounded support actions such as:
- routine support
- close monitoring
- activation of supportive intervention
- escalation to a human clinician It is intended for future application in analog astronaut missions, remote austere environments, and other settings where access to immediate behavioral health support may be limited. Importantly, ISPS-VETA is not a diagnostic tool, not an autonomous clinical system, and not a replacement for licensed clinicians. It is a simulation-based decision-support prototype built around governance constraints, explainability, and human oversight.
INSPIRATION: My work in analog astronautics, space medicine, and behavioral health has made it clear that high-risk environments require more than general-purpose AI assistance. They require systems that are carefully bounded, interpretable, and designed to escalate uncertainty rather than hide it. ISPS-VETA was inspired by the growing need for safe and responsible clinical support systems in isolated, confined, and extreme environments, especially where long-duration missions or remote settings create barriers to real-time human care. The project extends the governance-first AI safety philosophy developed in MAGSBHO into the clinical behavioral health domain.
HOW WE BUILT IT: ISPS-VETA was built as a simulation-based machine learning (ML) pilot using structured scenario data. The initial model uses behavioral and cognitive features such as:
- stress
- mood
- sleep quality
- cognitive load
- repeated distress signals
- social withdrawal These inputs are mapped to four triage outputs:
A. ROUTINE_SUPPORT B. MONITOR_CLOSELY C. ACTIVATE_INTERVENTION D. ESCALATE_TO_HUMAN_CLINICIAN
The pilot includes:
- a multi-class machine learning workflow
- structured scenario testing
- comparison of simple classifiers
- safety-oriented interpretation of outputs The model was developed within a controlled simulation environment and is framed strictly as a decision-support layer. Final judgment remains with governance logic and human clinical oversight.
This work is aligned with the GitHub repository: ISPS-VETA-Clinical-AI-Simulation
MACHINE LEARNING (ML) EXTENSION We implemented a preliminary simulation-based machine learning pilot to support behavioral health triage decisions under structured high-risk conditions.
The ML component includes:
- a multi-class classification framework for clinical triage actions
- structured scenario inputs based on behavioral and cognitive state
- comparison of lightweight models for interpretability and early feasibility testing
The system was evaluated not only for overall performance, but for safety-relevant behavior, especially the ability to recognize situations that should be escalated to a human clinician. Because this is a safety-critical application, the project prioritizes minimizing missed high-risk cases over optimizing raw accuracy alone. The ML output is used strictly as a bounded decision-support signal and does not function as an autonomous decision-maker.
As shown in the model results, the pilot demonstrates early feasibility for translating structured behavioral features into explainable triage recommendations within a governance-constrained AI framework.
MODEL EVALUATION RESULTS: The pilot model was tested on structured scenario data and generated triage predictions across simulated clinical situations. Results showed that high-risk cases could be mapped to escalation outputs while lower-risk cases remained within support or monitoring categories. The strongest model behavior was its sensitivity to escalation scenarios, which is especially important in safety-critical settings where missing a serious behavioral health signal could cause harm.
See image: ML v3 results: safety-aligned escalation and triage predictions
We extended ISPS-VETA to a Stage 2 interpretable clinical triage simulation by expanding the scenario dataset, adding temporal and frequency-based features, and comparing Decision Tree and Random Forest models. The upgraded model predicts four bounded triage actions: routine support, monitor closely, activate intervention, and escalate to a human clinician. To improve transparency, we added SHAP (Shapley Additive exPlanations), which shows which features most influenced each triage recommendation. This allows the system to provide not only a prediction, but also an interpretable rationale for escalation or intervention. This is especially important in behavioral health and safety-critical settings, where minimizing missed high-risk cases and supporting clinician oversight are more important than maximizing raw accuracy alone.
We implemented a Stage 2 interpretable machine learning model for behavioral health triage using an expanded dataset and structured feature set (stress, mood, sleep quality, cognitive load, repeated distress, social withdrawal, stress trend, and distress frequency).
The model predicts four bounded clinical actions:
- Routine Support
- Monitor Closely
- Activate Intervention
- Escalate to Human Clinician
In evaluation scenarios, the system demonstrated appropriate risk stratification:
- High-risk scenarios correctly triggered escalation to a human clinician
- Moderate-risk scenarios triggered intervention or monitoring
- Low-risk scenarios remained within routine support
We prioritized safety over raw accuracy, specifically minimizing false negatives in escalation cases. To improve transparency, we integrated SHAP (Shapley Additive exPlanations), allowing the model to provide interpretable reasoning for each triage decision. This enables clinician oversight and aligns with governance-constrained, human-in-the-loop AI safety principles.
CHALLENGES WE RAN INTO:
- One of the main challenges was balancing simplicity, safety, and credibility. Because ISPS-VETA relates to behavioral health and future clinical support, it was important not to overstate the capability of the model or imply autonomous medical decision-making.
- Another challenge was designing a pilot that was technically meaningful while remaining clearly simulation-based. We addressed this by using structured scenario data, bounded output classes, and explicit safety framing around human oversight, interpretability, and future IRB-based validation.
- A third challenge was ensuring that the project aligned with the broader MAGSBHO architecture without prematurely integrating a clinical system into the main governance framework. This is why ISPS-VETA is currently maintained as a separate pilot system.
ACCOMPLISHMENT WE ARE PROUD OF: We are proud that ISPS-VETA:
- extends our governance-constrained AI safety approach into the clinical behavioral health domain clearly separates clinical decision support from general wellness or operational support
- demonstrates a simulation-based machine learning pilot with safety-oriented framing aligns with the broader MAGSBHO QUARTET architecture as a future fourth agent
- maintains a strong “Do No Harm” philosophy and human-in-the-loop design
- We are also proud that the project is being developed with future IRB alignment and medical team oversight in mind, rather than treating clinical AI as something that should be deployed casually.
WHAT WE LEARNED: We learned that, in clinical and behavioral health settings, it is insufficient for an AI model to be accurate in general. It must also be bounded, interpretable, and able to trigger escalation when the risk is uncertain or increasing. We also learned that separating clinical support from non-clinical wellness and operational systems improves architectural clarity and safety. This reinforced our decision to develop ISPS-VETA as a separate pilot before future integration into the MAGSBHO QUARTET architecture. Finally, we learned that even simple machine learning models can be useful when framed correctly, as decision-support tools rather than autonomous authorities.
WHAT'S NEXT FOR ISPS-VETA: Next steps include:
- expanding the scenario dataset
- improving model evaluation and calibration
- incorporating temporal and physiological features
- clinician-guided labeling of simulated cases
- future IRB-aligned validation with medical oversight
- integration into the broader MAGSBHO QUARTET architecture as the fourth agent
In the long term, ISPS-VETA is intended to function as a clinician-supervised clinical support layer within a larger, governance-constrained AI ecosystem for high-risk environments.
VIDEO PRESENTATION LINK: https://youtu.be/FgAwKZ4fLDk
ALIGNMENT WITH GITHUB REPOSITORY: ISPS-VETA is intentionally aligned with the GitHub repository version of the project and is being presented as the same simulation-based clinical AI pilot system, with consistent architecture, safety framing, and machine learning scope across both platforms. (see github link below)
Built With
- ai-safety
- behavioral
- clinical-ai
- health
- human-in-the-loop
- machine-learning
- pandas
- python
- scikit-learn
- simulation

Log in or sign up for Devpost to join the conversation.