-
logo
-
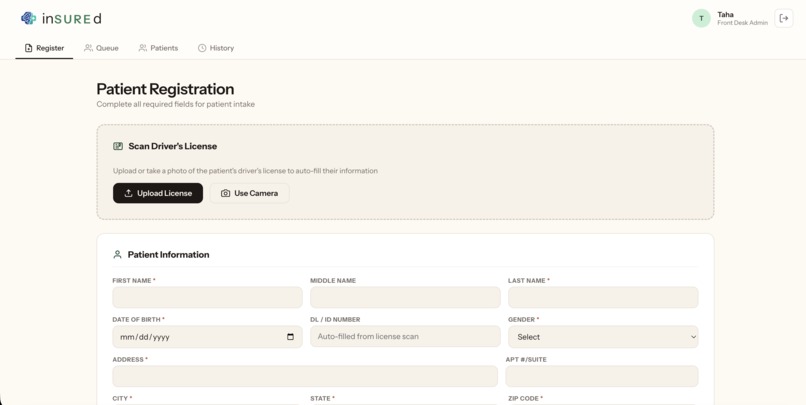
patients registration page
-
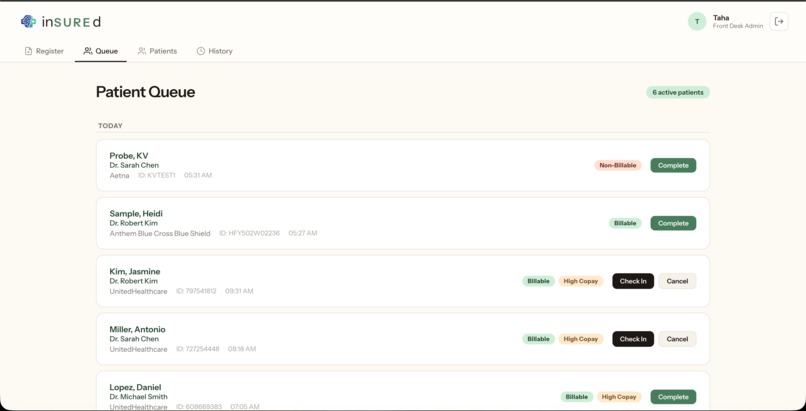
patients queue page
-
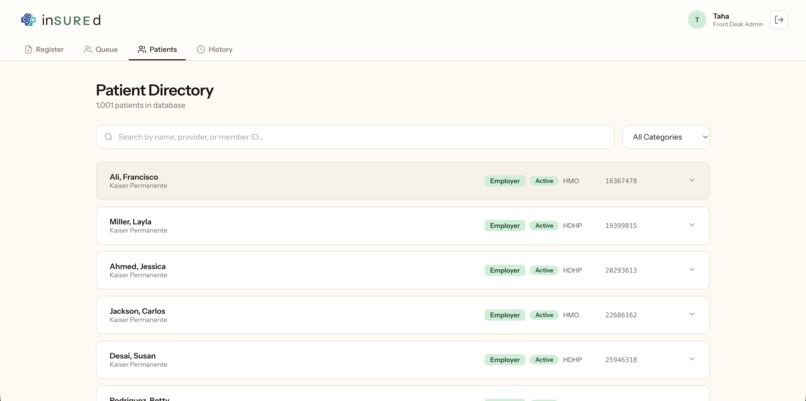
patients page
-
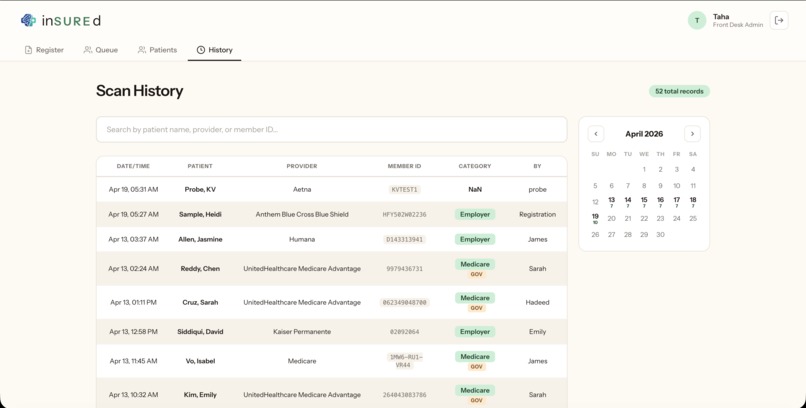
patients history page
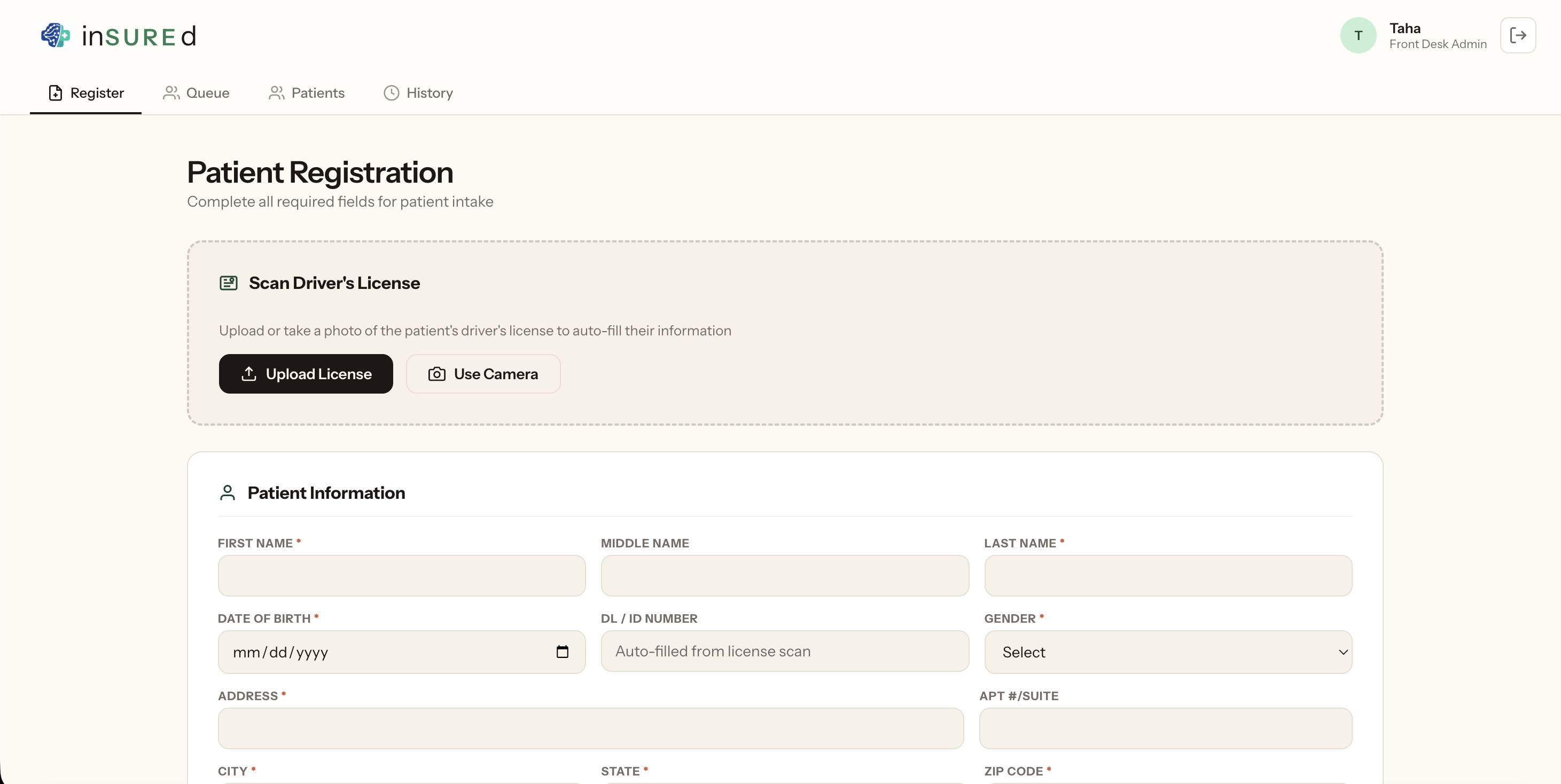
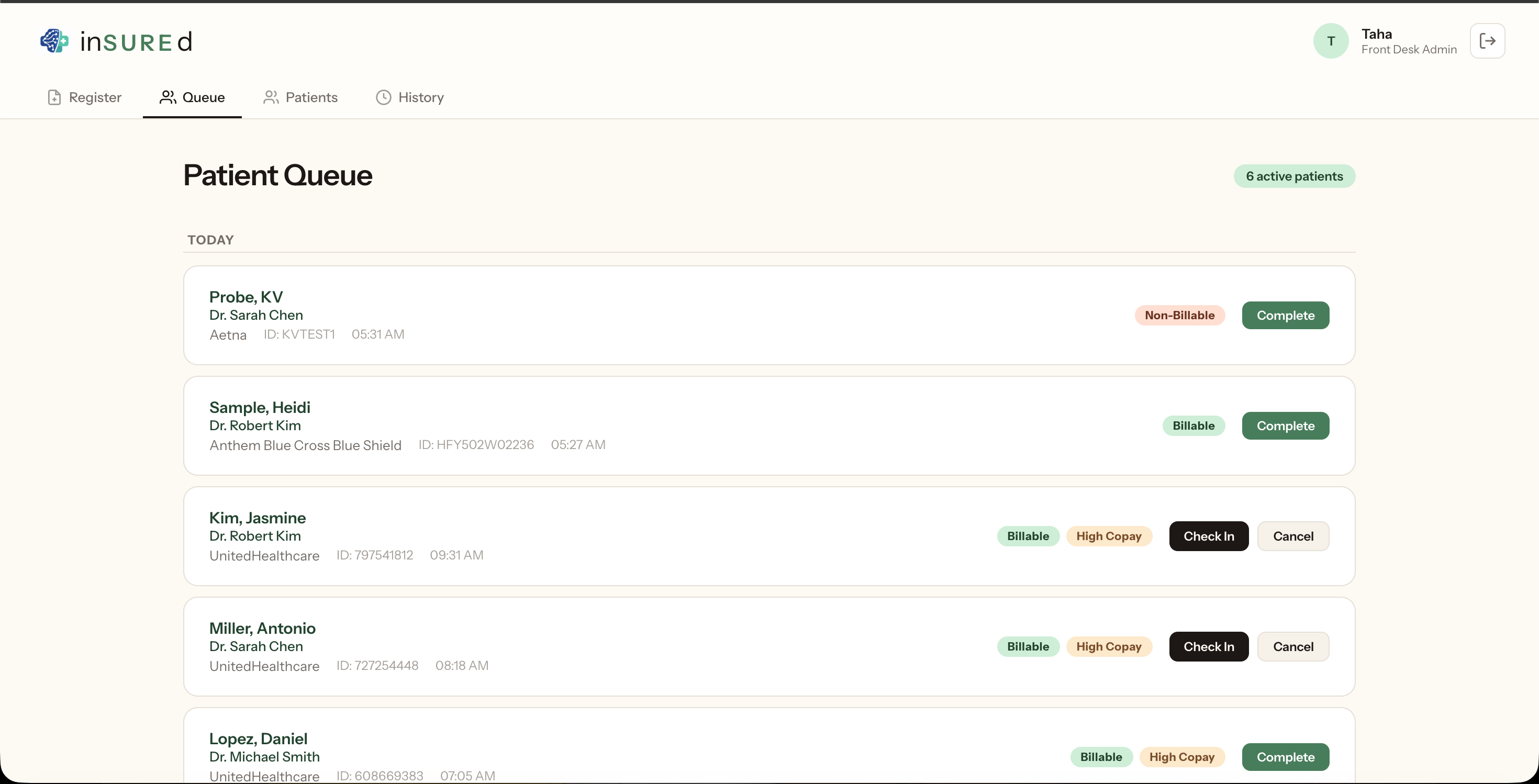
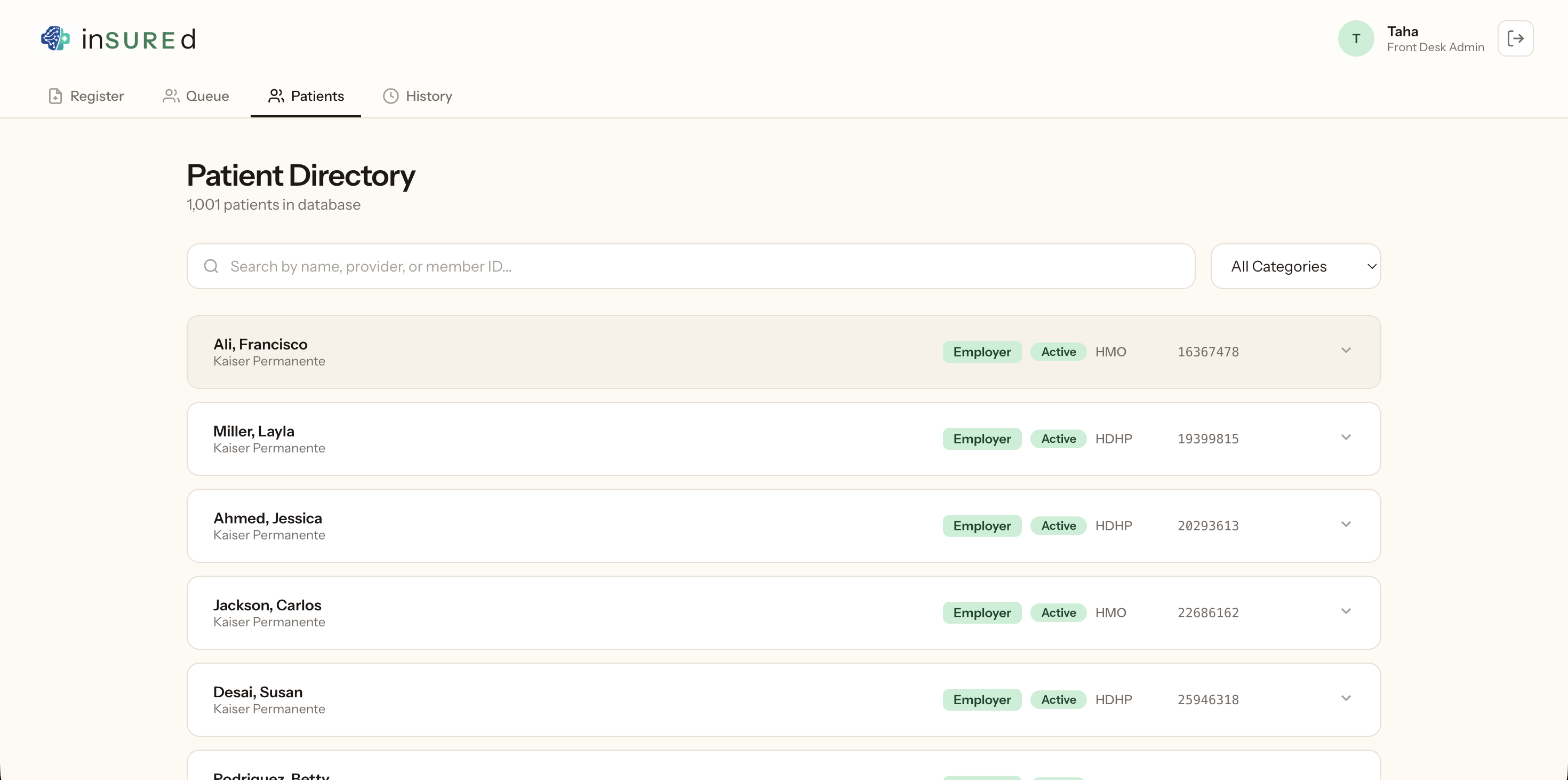
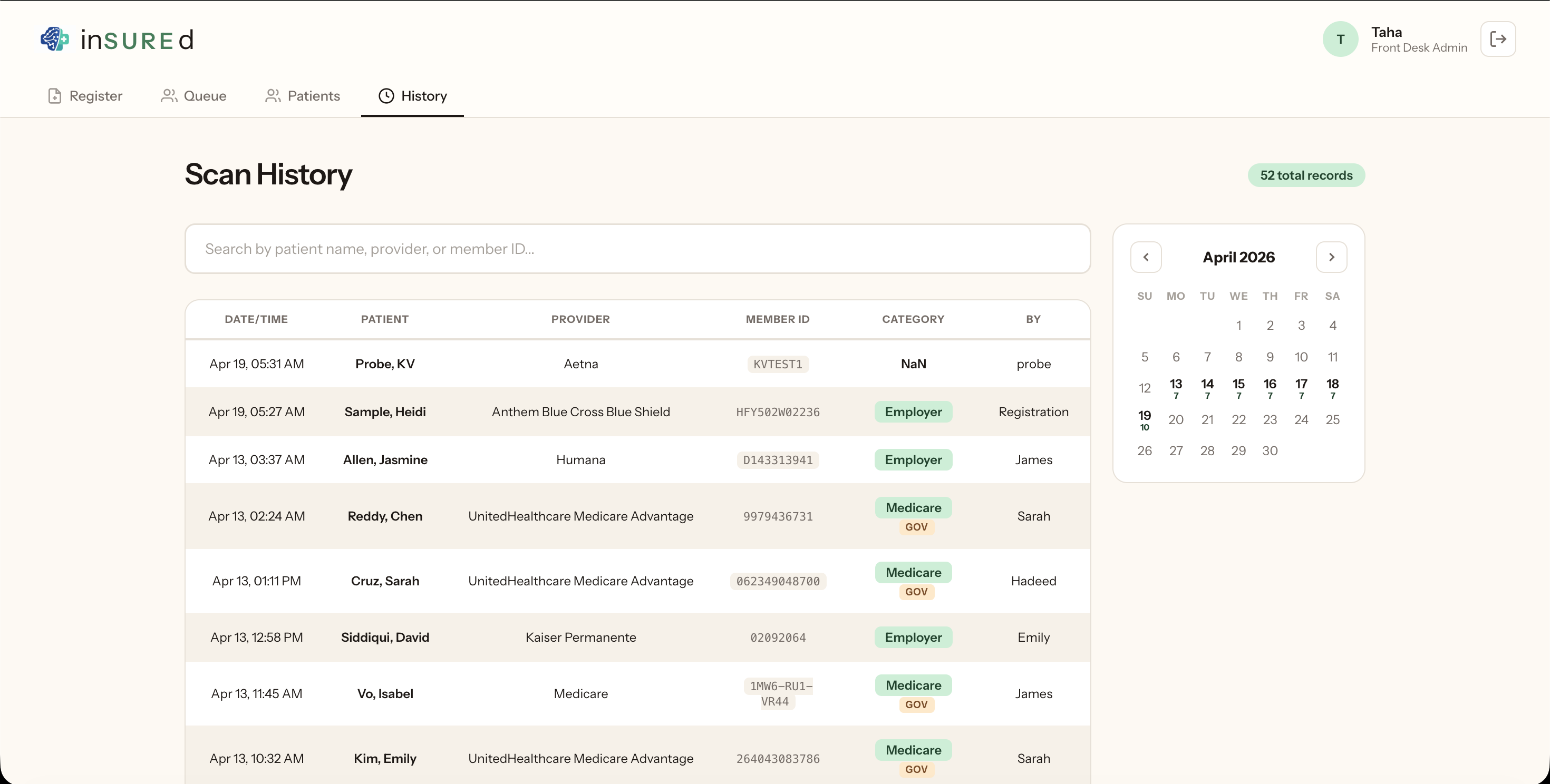
Ten minutes. That's how long the average ER nurse spends on hold with an insurance company for a single patient — reading group numbers into a phone, waiting on a human to look up benefits, scribbling copays on a sticky note — while the patient in bay 4 is asking a question nobody can answer yet: how much is this going to cost me? We watched a family member pace an ER hallway for 45 minutes last year waiting for someone to tell them whether a CT scan was $200 or $20,000; they left without the scan, and that moment — where paperwork becomes a medical decision — is what inSUREd is built to erase. inSUREd turns a phone camera into a benefits-verification engine: point it at any US insurance card (employer, Marketplace, Medicare, Medicaid, Tricare) and Claude extracts the member ID, group, plan type, and payer in under two seconds, then the same flow works for a driver's license using AAMVA field numbers and auto-rotation so a single photo populates the entire patient registration, and the moment the card matches, the front desk sees ER copay, coinsurance, deductible remaining, out-of-pocket max, in-network status, and whether a prior auth is required — every plan rated good, caution, or bad, with the traps called out explicitly: EPOs with no out-of-network coverage, HMOs that need PCP referrals, limited-benefit plans that won't actually pay for the ER visit, even a same-day-discount script the front desk can read word-for-word, and return visits auto-detected with an insurance-change diff flagged before anyone asks. We built the whole thing inside Replit — the browser-based IDE meant we could pair-code from anywhere without wrestling with local environments, spin up the dev server in one click, and iterate on prompts and UI changes side-by-side with a teammate watching the same terminal; from Replit we shipped to React 19 and Vite on the frontend, a single Vercel serverless Express function on the backend, Claude Opus 4.7 for license OCR (the AAMVA field-number trick cut hallucination massively) and Claude Sonnet for card extraction, sharp to bake EXIF orientation into pixels and rotate portrait captures before the model ever sees them, a 1,000-card synthetic insurance database covering every major Texas payer plus Medicare and Medicaid MCOs with realistic deductibles and prior-auth lists, Upstash Redis for the scan history, queue, registrations, and audit log, and HIPAA-grade audit breadcrumbs from day one logging every scan, status change, and failed login with the acting user and role. The challenges were real — Claude auto-completing uncommon names to common ones until we told it the AAMVA field numbers were labels not values, every phone capture landing sideways until we baked orientation into pixels and detected portrait aspect ratio, our first Vercel deploy silently losing half the queue between Lambda instances until we migrated every piece of state to Redis behind a thin abstraction, and "BCBS," "Blue Cross," "Anthem," and "Blue Shield of Texas" all resolving to the same issuer forcing us to build an alias table with a payer-name fallback — but the payoff is under 3 seconds from tapping the camera to seeing the ER copay on screen, a coverage engine that isn't a wrapper around a GPT call but a real benefits model with deductibles and prior-auth rules, role-aware access and a real audit trail from day one, and warnings with taste — we don't just show the plan, we tell the staff what's going to bite them about it. What we learned is that models are shockingly good at structured extraction when you stop treating them like OCR and start treating them like a domain expert with a camera, that healthcare UIs are judged on speed not polish because every second of spinner is a second the nurse goes back to the phone, that "just use in-memory state for the demo" is how demos die at the worst possible moment, that a browser-based dev environment like Replit removes an entire category of "works on my machine" bugs before they happen, and that the boring parts — audit logs, role gates, insurance-change detection — are what separate a hackathon toy from something a clinic might actually run. What's next is real benefits APIs (Availity, pVerify, Change Healthcare) replacing the synthetic DB, plan-aware ordering that shows the physician the patient's cost for a CT vs. ultrasound vs. observation before the order is placed, prior-auth automation kicked off from the same scan, expansion beyond the ER to outpatient, urgent care, and specialty offices facing the same ten-minute call, and a patient-facing QR code they can scan on their own phone to see their own estimate in plain English while
Built With
- claude-sonnet
- css3
- express.js
- git
- heic2any
- html5
- javascript
- multer
- node.js
- openrouter
- react
- react-router
- replet
- sharp
- tesseract.js
- upstash-redis
- vercel
- vite

Log in or sign up for Devpost to join the conversation.