-
-

-

-

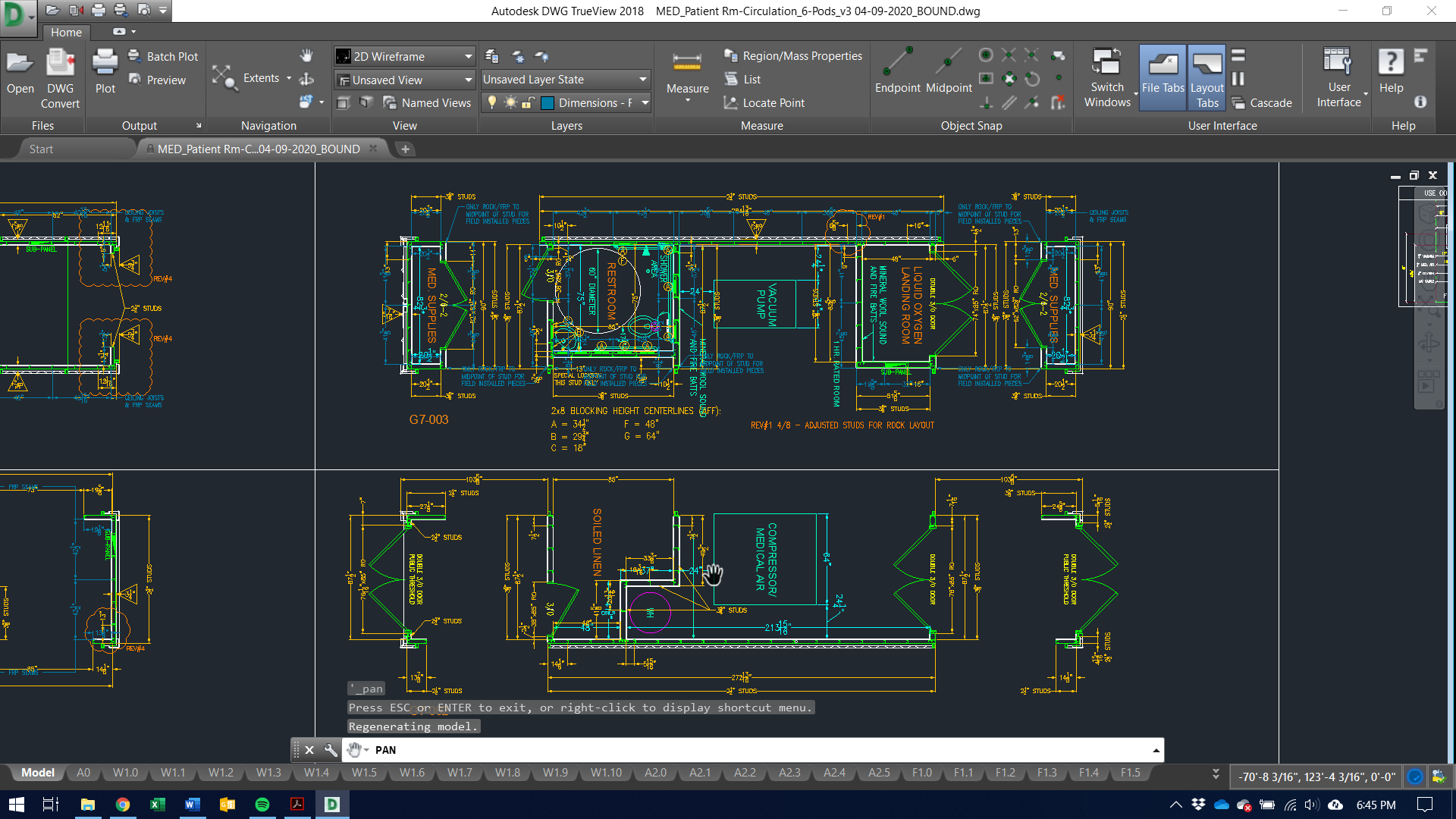
General_Layout_view
-

-

-






Inspiration
The inspiration to deliver a solution to the healthcare facilities shortage crisis was prompted by a report by the United States Army Corps of Engineers (USACE) that urgently requested aid across the construction technology and manufacturing industry to meet the demand for add-on medical facilities amid the COVID-19 Epidemic. Solutions that would typically take months to deploy now need to meet a 2-3 Week delivery timeline & the entire industry had moved to combine efforts surrounding automation technology, manufacturing configurations, engineering, supply chain, and medical delivery solutions. - the rush of conversations left me feeling that concepts that could be combined/optimized/improved were being overlooked. The hackathon and this project had a serendipitous alignment with the abstract I wish to submit for the Ph.D. program at Stevens in August.
What it does
The systems design developed by the team allows emergency services, local and federal agencies, and private hospital systems to deploy additional emergency facilities to overcrowded healthcare facilities. This prevents infection, isolates and allows for technology-enabled treatment for the massive patient flux in recent months. This directly addresses the healthcare facilities shortage nationwide.
How WE built it
Between the several industry peers that participated, the combined concepts led to a solution that would be greater than the parts. As part of the project, we held calls with The CEO of Module, the President of BMarko Structures, and the Executive officer of the Modular Building Institute and discussed with them the different approaches to supplemental care unit (SCU) solutions. It was clear that there was an opportunity to integrate facility configurations and deliver a scalable and cohesive design.
Challenges I ran into
- Sanitary air ventilation across isolation vs. intensive care units. Mechanicals were underpowered by design and if stacked, would be less mobile. We needed more output and less footprint
- Roll-off vs. slab mounted foundation footings. Needed a solution that would not require as much site preparation or cost in order to be scalable.
- Needed to avoid losing structural integrity when designing vent systems to circulate 'medical air' throughout the units. Sourced alternate materials, truss systems, and committed to steel superstructures
- Integrating personnel facilities that did not conflict with patient areas and avoiding structural overhangs that would extend install time
Accomplishments that I'm proud of
- I am proud of the fact that all of the team members were so quick to act despite having full-time endeavors and activities in the field supporting the Covid-19 healthcare systems. I am proud of the team for coming together on such short notice.
What I learned
- I had always heard that crisis is a hotbed for innovation. However, never have I had so many people in positions with such access, across the nation, get back to me overnight. I realize now that it is not just that crisis is a catalyst for innovation but rather that it is a total equalizer when it comes to communication. The healthcare and housing production industries are hyper-competitive and conversations about design across different nodes take months-years-decades. In times of crisis, you can reach conceptualization in weeks.
What's next for ICU Patient Rooms JIT/On-Demand
- The different partners have their concepts actively supplying the Army Corps, GEMA (Georgia Emergency Management). Most recently I was speaking with someone from Momentum Consulting and the Modular mobilization commission and made contact with a Purchasing agent at the USA General Services Administration. I believe the solution fits some of their recent RFPs.
Built With
- autocad


Log in or sign up for Devpost to join the conversation.