-
-
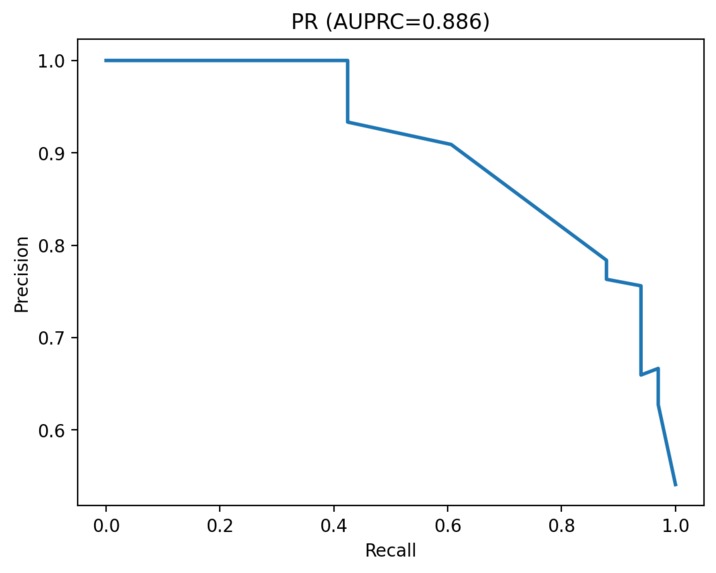
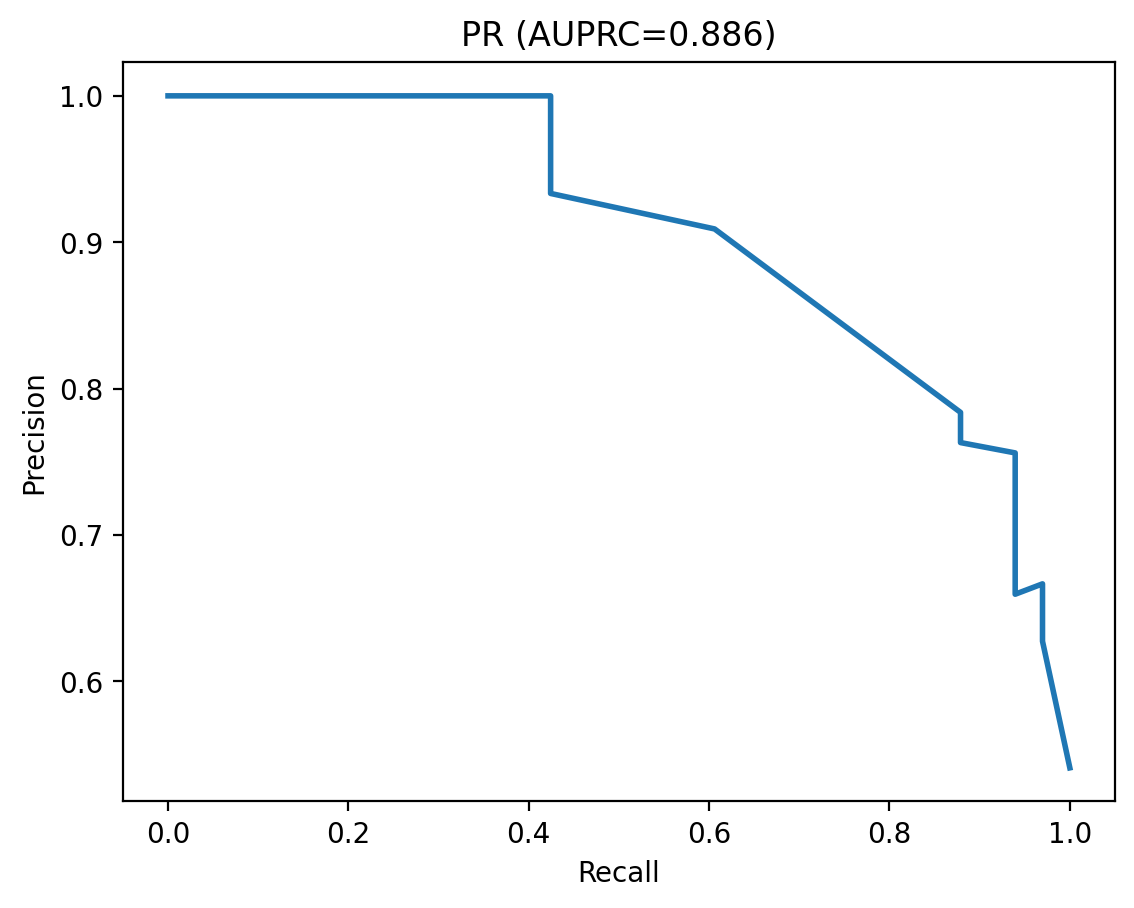
Precision-Recall Curve
-
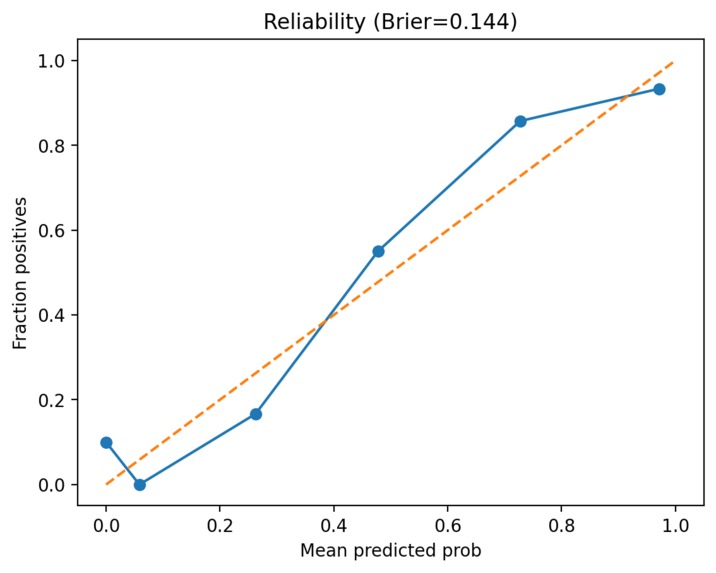
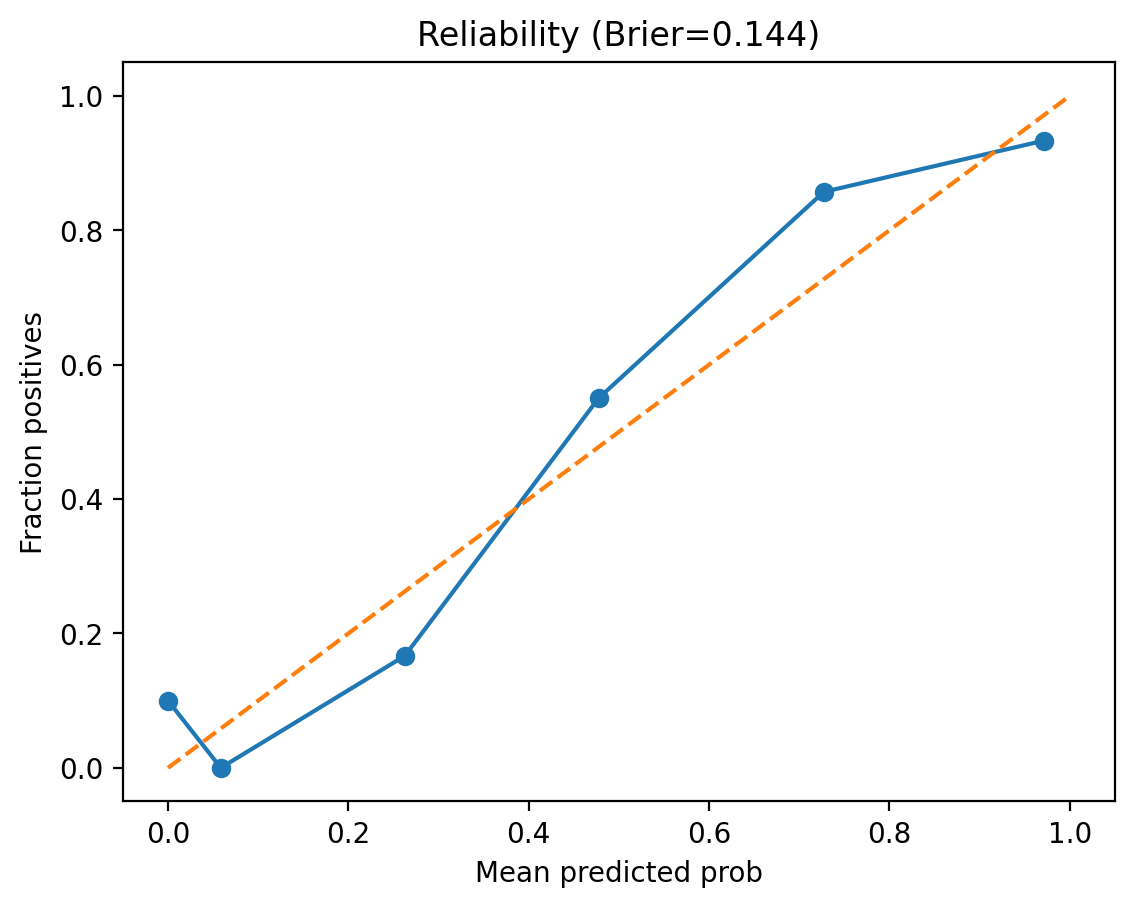
Reliability Curve
-
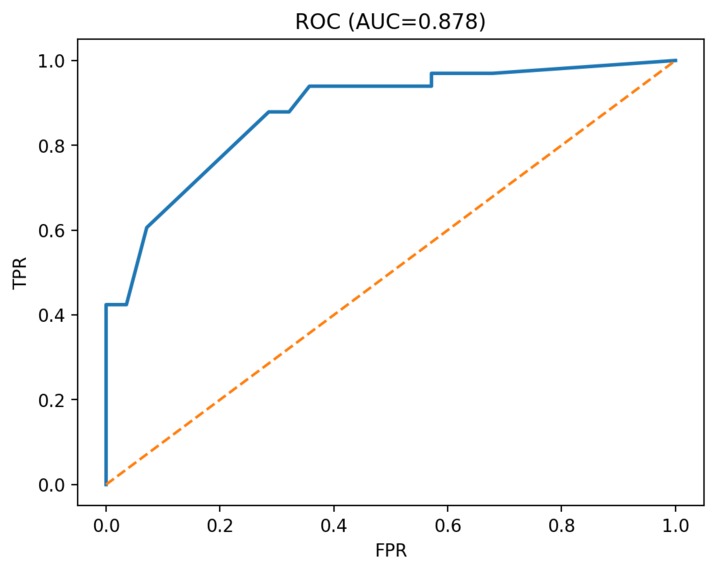
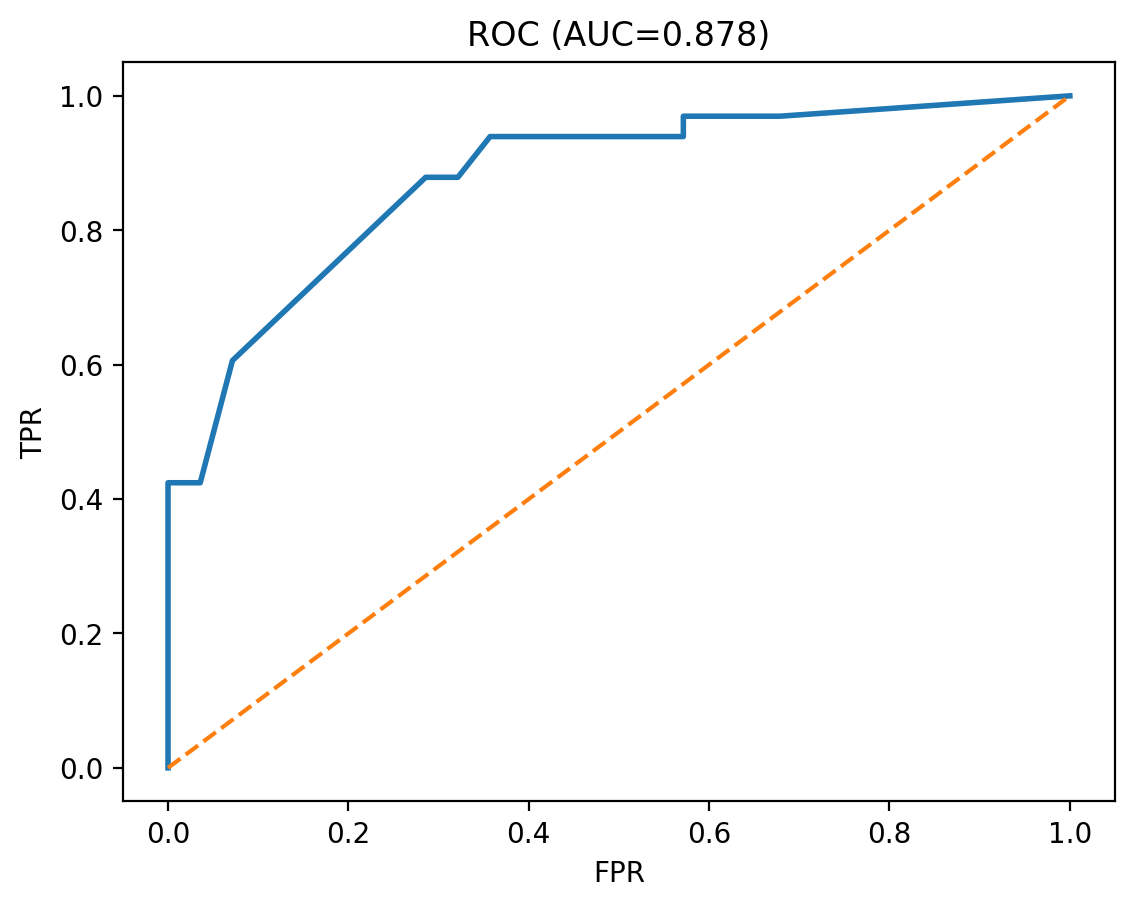
Area Under Curve
-
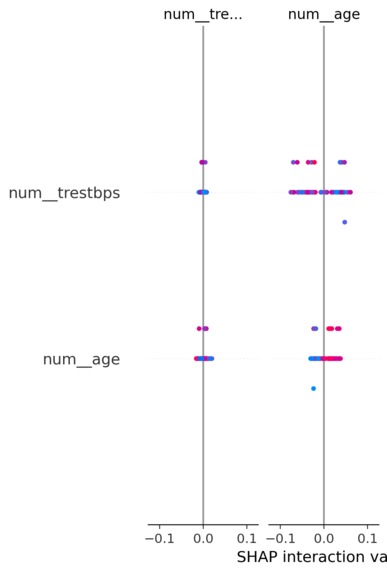
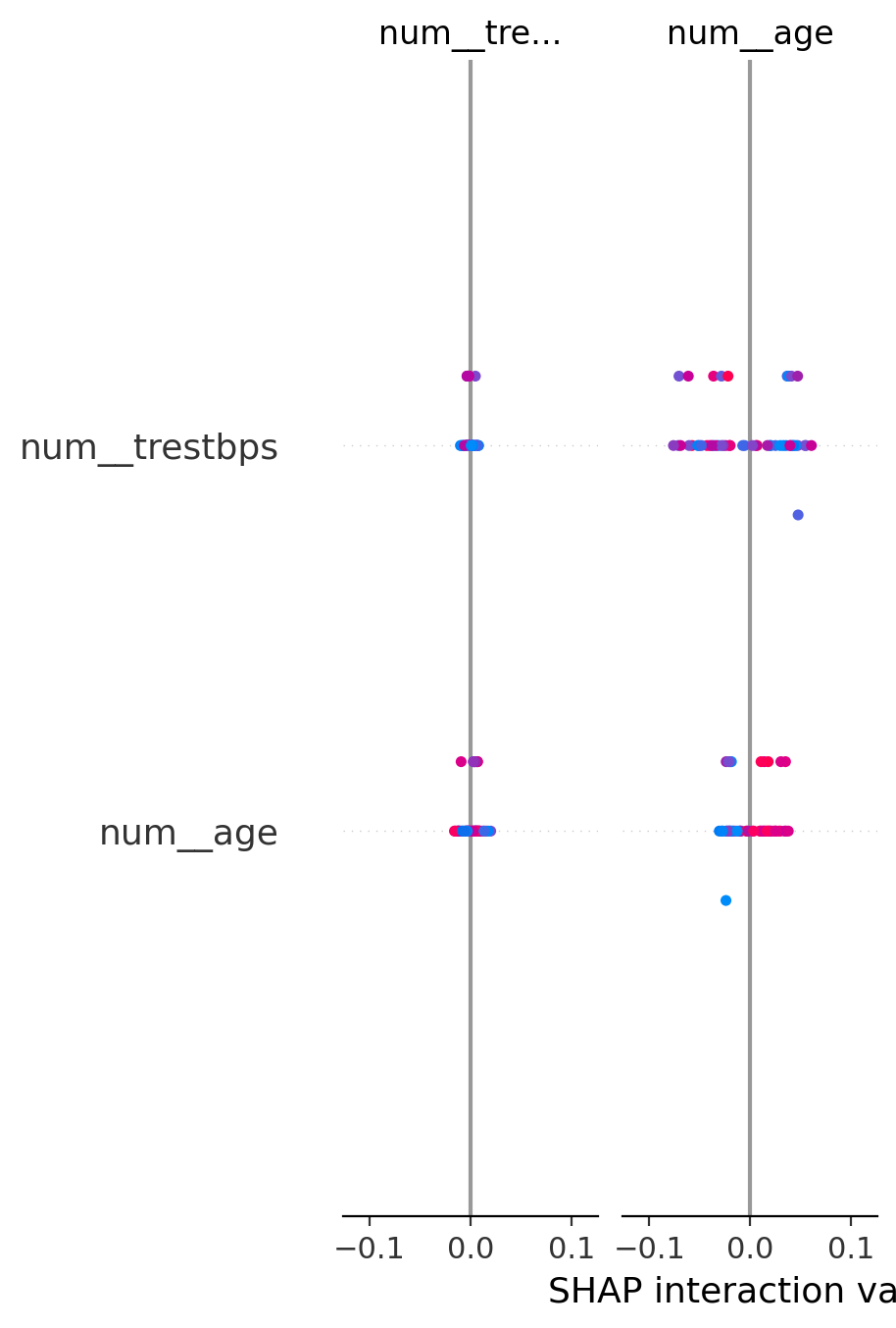
SHAP Explainability Plot
Inspiration
Crowded triage lines, limited cardiology slots, and inconsistent risk estimates. I wanted a tiny, transparent tool that provides clinicians with a calibrated probability (not just a score), explains why the prediction occurred, and highlights fairness gaps - so they can route patients more efficiently and safely.
What it does
- Predicts a calibrated probability that heart disease is present from 13 routine inputs.
- Maps probability into Low / Medium / High bands using a documented demo policy (Low < 7%, High ≥ 35%).
- Explains each decision (SHAP or robust fallbacks) with signed bars.
- Monitors fairness via simple slice AUCs (sex, age buckets, chest‐pain type).
- Shows model quality (ROC, PR, calibration curve, AUC 95% CI).
- Scores uploaded CSVs in batch and lets you push any dataset row directly into Triage.
How we built it
- Data: Kaggle Heart Disease dataset; I deduplicated to 302 rows to avoid leakage/duplicates.
- Modeling: ColumnTransformer (scale numeric + one-hot categoricals) → Random Forest (final) and Logistic Regression (baseline) → isotonic calibration with CalibratedClassifierCV on a held-out fold → 20% test evaluation.
- Explainability: shap.TreeExplainer for RF, shap.LinearExplainer for LR, with coefficient/importance or directional ablation fallbacks.
- App: Streamlit multipage UI (Triage, Explanations, Fairness, Model Quality, Data Explorer, Batch Scoring).
- Thresholds: I documented a principled selection method (capacity/PPV for High, miss-rate/NPV for Low) and used 7% / 35% as sensible demo defaults.
Challenges we ran into
- Tiny dataset → risk of overfitting; required restrained RF tuning and held-out calibration.
- Explaining calibrated models → I had to unwrap CalibratedClassifierCV to explain the underlying estimator cleanly.
- UI clarity → making calibration/bands and “per-100 patients” interpretation obvious to non-ML users.
- Data hygiene → removing duplicates so train/validation/test splits were honest.
Accomplishments that we're proud of
- End-to-end, reproducible pipeline with artifacts and a clean demo app.
- Calibrated probabilities that make thresholds meaningful, not arbitrary.
- Clear, signed local explanations and quick fairness slices that surface operational watchpoints.
- Lightweight app that runs anywhere without PHI.
What we learned
- Calibration changes the conversation: 30% means ~30/100, which clinicians understand.
- Thresholds must be tied to capacity, PPV/NPV, and miss tolerance, not gut feel.
- SHAP with calibrated models requires care; transparency beats raw accuracy in triage tools.
- Small UX choices (vertical bars, per-100 wording) dramatically improve comprehension.
What's next for HeartRisk Assist - Cardiac Risk Triage (Medi-Hack 2025)
- Train on-site EHR cohorts (e.g., MIMIC-IV/PhysioNet) with IRB/governance.
- Add an auto-threshold finder (capacity/PPV and miss-rate/NPV rules, decision curves) and cohort-specific bands.
- Prospective A/B tests, drift/bias monitoring, and clinician-in-the-loop feedback.
- Expand features (labs/meds), improve accessibility, and package for hospital deployment.
Team
Solo: Sweety Seelam
Built With
- altair
- github
- joblib
- jupyternotebook
- kaggle
- machine-learning
- matplotlib
- numpy
- pandas
- python
- scikit-learn
- shap
- streamlit

Log in or sign up for Devpost to join the conversation.