Carego International is pleased to submit our Early Detection and Prevention System (EDPS) in the Application for Development Competition. We have a best in class system that will enable Community Health Workers to go out into poor rural areas and diagnose illness from the EDPS program of 300 diseases. Included in our submission is the following: - Carego International EDPS Summary - Video Tutorial - We used the following data sets for diagnosing malnutrition in our application
- Prevalence of child malnutrition is the percentage of children under age 5 whose height for age (stunting) is more than two standard deviations below the median for the international reference population ages 0-59 months. For children up to two years old height is measured by recumbent length. For older children height is measured by stature while standing. The data are based on the WHO's new child growth standards released in 2006.
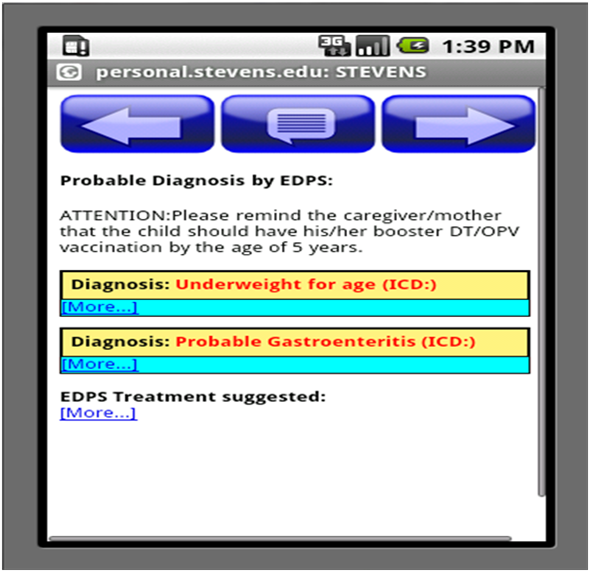
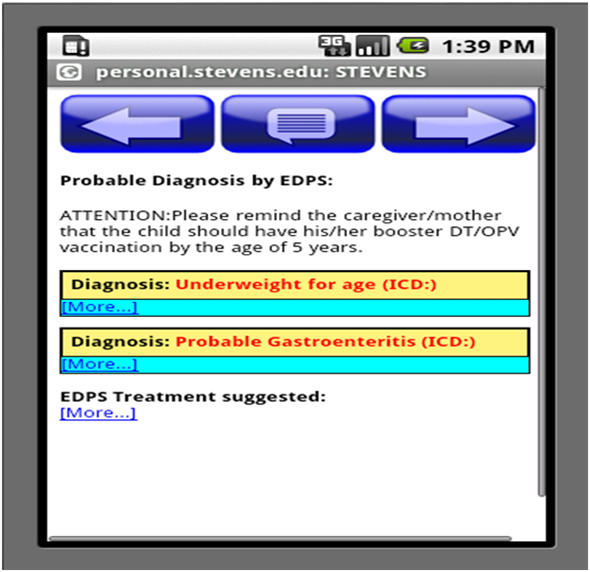
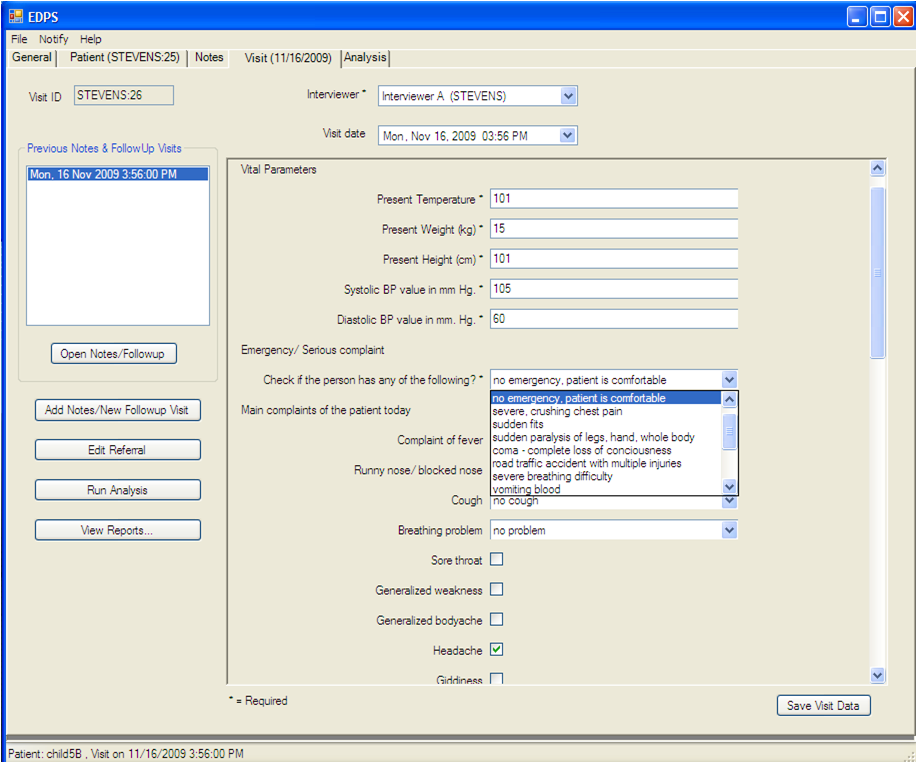
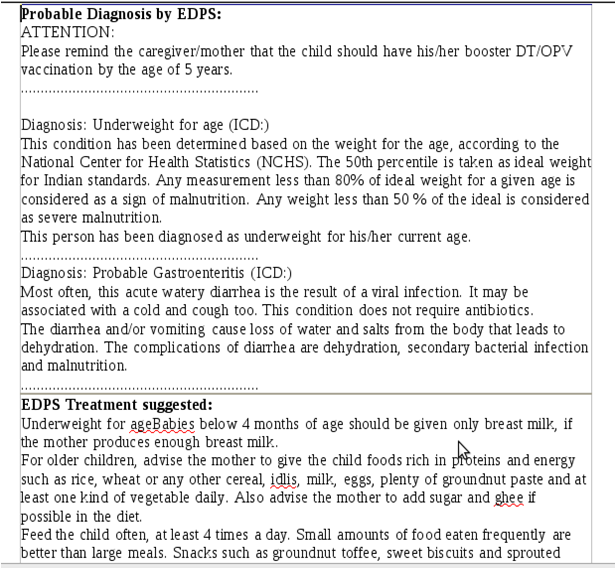
- Prevalence of child malnutrition is the percentage of children under age 5 whose weight for age is more than two standard deviations below the median for the international reference population ages 0-59 months. The data are based on the WHO's new child growth standards released in 2006 EDPS is not currently a web based system so we are unable to provide a link to the application at this time, however, we are available to conduct a web based presentation of the application for the judges or a representative of your choosing. Please contact Steve Landman (415) 297-4106 for a demonstration of the application. We feel this application is going to have an incredible impact in many areas of the Millennium Development goals and are excited about gaining visibility to the application. It is ground breaking and an important component of gathering data for the World Bank and achievement of the Millennium Development Goals. EDPS is the perfect healthcare application to impact the Millennium Development Goals in multiple categories because it captures on the ground data in poor areas where healthcare is not available or readily accessible. EDPS is currently being deployed in a unique self sustaining healthcare delivery system at LiveWell Clinics in Africa. LiveWell Clinics is creating a unique hub and spoke medical clinic model to reach out into rural communities utilizing mobile clinics, community healthcare workers and the EDPS application. This model has been identified by USAID as one of the most likely sustaining healthcare models to succeed out of 450 studied under the SHOPS Project. To learn more about Carego International and LiveWell Clinics please visit our website at: www.caregointl.com . What is EDPS 2000? EDPS stands for Early Detection and Prevention System; it is a computer software system designed to support a new approach to providing quality health care to the rural poor throughout the world. It aims at enabling early detection of diseases and nutritional deficiencies, even in the absence of a physician, as well as to assist the medical personnel assigned to PHCs in their daily tasks. The objective is to increase the rural population’s access to quality healthcare by identifying those individuals who need prompt attention by qualified physicians, and treating those who have minor illnesses who can be safely cared for even in the absence of a doctor. EDPS2000 is therefore designed to provide a probable diagnosis of disease, based on symptoms and signs presented by the patients. It should be understood that it does not aim to give a confirmatory diagnosis. It mainly functions as a first line of intervention whereby the patient, equipped with a probable diagnosis, can then go to the next level – referral to a physician, conduct a lab test, or safe home treatment, as appropriate. The system provides several reports that assist the field workers in the field, meet internal and external reporting requirements, and streamline the workflow at the PHC facility. Rural Health Initiative Steve Landman, the Co-founder of our organization, recognized the acute need for adequate primary healthcare in rural regions of developing countries for many years and initiated a partnership with the George Foundation. The mission statement of this partnership is to demonstrate a model of rural primary health care services deliver y providing universal access to high quality personal ambulatory care services at a reasonable cost. Functionalities In order to provide complete and efficient personal ambulatory care, EDPS2000 contains several functions and databases including the following: ü A database of disease characteristics & diagnostic logic for diagnosis and early detection of common conditions prevalent in India, as well as many other diseases common in other parts of the world. The list of approximately 300 diseases presently covered by the software can be found in Annex A. ü A database of corresponding prevention, curative and referral recommendations that are strictly based on established protocols and practices relevant to the provision of primary care in the developing world. ü Automated patient records allowing reliable analysis of patient conditions as well as adequate follow up. ü Report-generating capabilities to assist staff with field based issues, such as reminders for required shots, administrative reports and other requirements. ü A statistical section enabling provision of essential public health services such as screening, follow up and epidemiological surveillance. Ambulatory primary healthcare services The patients visit healthcare clinics or have community healthcare workers go out into the rural areas, are first seen by the EDPS2000 team. The steps followed for every patient include: (1) Taking their vital signs (BP and temperature), as well as their weight and Height. (2) Creating their personal file, with a unique ID for each person, by registering their socio-demographic information, life style patterns and past medical history in the EDPS2000 database, (3) Obtaining the history related to their present problem, including main complaint, associated symptoms and physical signs obtained from simple examination techniques. This information is then used to formulate a report that contains their probable diagnosis (with the corresponding curative and preventive advices). This report is printed and given to patients who can then be seen by a physician for confirmation of treatment and final action. It has been found that patients' satisfaction is high regarding the provision of care given by the EDPS2000 team, partly because of the time spent with patients (6 to 10 minutes), as well as the fact that a written report is provided to them to keep as their own. Moreover, the fact that the information is computerized has also allowed us to record useful statistics regarding the population utilizing our service, as well as regarding the nature of problems most commonly seen. EDPS2000 at Bagalur PHC In August 2000, the government of Tamil Nadu implemented EDPS at a clinic in Bagalur, a village in Tamil Nadu, using the Bagalur PHC is a busy clinic, serving more than 100 villages in an area of about 50 KM sq in rural Tamil Nadu, and covering a population of more than 80,000 people. The main aim of this second stage of implementation of EDPS2000 was to test the system in a real rural outpatient setting. Since August 2000, EDPS2000 has been used in Bagalur PHC with excellent results: more than 40,000 patients are now registered in our database and we have received more than 17,000 patient visits thus far. Non-personal health care services Screening and early intervention in maternal child health EDPS2000 aims at providing all aspects of high quality personal health care services and includes, over and above the disease and treatment specific information, a public health section containing the epidemiology and surveillance information relevant to the rural Indian population. The information recorded in the statistics section of the system also covers all aspects of maternal child health, (antenatal, delivery and postpartum care reports), as well as immunization and nutritional status of children under 5 years of age. These functions are not only important from a surveillance point of view, but they also contribute to support the work of the Village Health Nurse/ Auxiliary Nurse Midwife (VHN's/ANM's) in 3 important ways: 1. Increasing the efficiency of the primary and secondary prevention interventions which are under their responsibility, making sure they are performed in due time, without forgetting anybody. 2. Allowing for follow up of trends in some of the main vital statistics obtained (such as birth rates, infant death rates, etc., which are now done by hand), especially now that we have denominators available. 3. Reducing the field workers’ (VHN/ANM) bookkeeping time, since 8 of their 15 regular registers can be replaced by the filling of the AN and Child care forms. Epidemiological surveillance and evaluation of health system performance EDPS2000 statistical functions and reports have tremendous potential for tracking disease epidemics (of either reportable diseases or any other diseases listed in the system), hence initiating early investigations and interventions when required. Another area of current strategic interest is the use of such technology for assessment of population health profiles, including morbidity and mortality figures, as well as risk factors prevalence and measures of inequalities in health status among the poor and other vulnerable groups. One can easily see how EDPS2000, when extended to other sites, has the potential to become key in allowing governments at all levels (local, regional or national) to assess and monitor the performance of their health system, hence facilitating planning. Concluding comments EDPS2000, by contributing to the prevention, screening, diagnosis and treatment of common conditions in rural India, represents tremendous potential for improvement of the health status of rural populations throughout the world. It will greatly improve the accessibility of primary care to the rural populations and also tremendously enhance the quality of care that is being provided. Indeed, EDPS2000 has the potential to assist in providing quality healthcare for all in the following century. It provides essential health care services that are both of high quality and acceptable to individuals and families of the rural community in India, at a cost that can be supported by the society. By addressing the issues of diseases and cures, and emphasizing prevention and the measurement of the non-medical determinants of health, EDPS2000 can help make information technology a crucial tool in building a global strategy of health promotion and disease prevention in the developing world. Early Detection and Prevention System frequently asked questions The following is a list of questions most commonly asked by the medical community regarding the implementation of EDPS2000 at Bagalur PHC. It takes more than 5 to 6 years to fully train medical doctors in this country; 1. How can EDPS2000 be operated by non-medical personnel and hope to replace the quality of services which can be provided by a fully trained doctor? As mentioned in this brochure, EDPS2000 does not aim at replacing the services provided by doctors. It simply provides services to assist doctors and offers medical care where no doctor is available. Many services provided by fully trained medical doctors cannot be provided through EDPS2000 (such as the provision of a detailed physical examination, for example). However, what EDPS can do is to help the operator, through simple questions, to distinguish patients who need the services of a medical doctor (and to refer them accordingly), from those who have minor ailments, which can be taken care of at home with safe non-pharmaceutical measures (such as common colds, simple skin rashes, malnutrition). In these cases, preventive and symptom relieving advices can be provided safely and effectively, bringing significant improvement of the patient's condition, while increasing the efficiency of the medical services provided at the PHC. 2. If EDPS2000 is aimed at providing essential primary care services in the absence of a medical doctor, why is it implemented and operated in a PHC where medical officers are available? EDPS2000 is not limited to early diagnosis of diseases, which can be done by the doctor present at the PHC. It enables the PHC to have a permanent computerized record for every patient, obtain statistics of all the field services conducted by the PHC, as well as allows the PHC to detect disease trends. For the doctor, EDSP2000 can serve as a screening tool, where patients with simple illnesses or visits for repeat injections etc. can be seen by a nurse, thus giving the doctor enough time to spend with more complex cases. Moreover, EDPS2000 is still in its early implementation phase. The main reason for having EDPS2000 operating in a PHC that are staffed with several medical officers, and hence having the patients seen twice (by both the EDPS2000 team and the PHC physician) is to allow us to further compare the system diagnostic accuracy with the doctors' diagnostic impression. This also permits us to actually test the efficiency of the system in a busy clinical setting, as we believe that safety and efficiency are the most important criteria to ensure that EDPS2000 will enable us to provide high quality of ambulatory care in rural India. Once this implementation phase is completed with success, EDPS2000 will then be ready for expansion to all rural areas, even where no doctors are available, hence providing primary care services to patients who often cannot access any type of formal ambulatory care services. 3. How do patients react to EDPS2000 registration? Do they like it? Yes, indeed, they do. Patients come back to see us and say they are satisfied with the services we are providing them. Part of it is because we take all their vital signs as well as their weight and height, and also because we ask them questions about their present problem in great detail (taking up to 10 minutes per patients). Finally they are given their personal report (containing their diagnosis and treatment recommendation), which they can keep at home. Every patient also receives a unique ID card and number that can be used for repeat visits and follow up. EDPS2000 tends to provide a list of probable diagnoses (or a “differential diagnosis”) instead of a single diagnosis for the patient's condition; 4. How will the operator, in the absence of a medical doctor, use this information to provide care? Because EDPS2000 functions even in the absence of a medical doctor, it has been purposefully designed to be used as a screening tool, allowing the operator to distinguish patients suffering from severe conditions, from those affected with minor ailments. As in the case of any screening instrument, therefore, EDPS2000 needs to be able to identify all possible conditions potentially present, rather than to make a very precise diagnosis of the patient's conditions. In epidemiological terms, EDPS2000 needs to be more sensitive than specific, thus ensuring that no severely affected patients will be missed by the system. Consequently, differential diagnosis lists are sometimes over-inclusive, as well as, at times, including more severe conditions than what an experienced doctor would assess them to be. But this is not a weakness in the system, but rather a quality that is necessary to ensure that no patients are left untreated if they require medical attention. 5. If EDPS2000 is operated in the absence of a doctor, how will you ensure the proper medication is chosen and administered correctly? Isn't this illegal? The treatment advices provided by the system do not include any pharmaceutical intervention for which a doctor's prescription would be required by law. Our advice, therefore, mainly emphasizes prevention, by including advice on how to prevent conditions from getting worse (such as keeping a wound clean and dry), as well as on how some conditions could have been prevented altogether (through immunization, and proper nutrition, for example). When appropriate, safe home remedies are provided to help alleviate some of the patient's symptoms (like steam inhalation for nasal congestion, and cold compresses of minor burns, for example). Consequently, conditions that require the prescription of medication are attached with a recommendation for referral to a physician (either a generalist or a specialist, as the case may be), for confirmation of the diagnosis as well as provision of appropriate pharmaceutical intervention. The ethical imperative of non-malfeasance (“First, do no harm”) is therefore respected, as it should always be when health care services are provided. Often a precise diagnosis can only be made using the results of laboratory investigations. 6. How will this information be made available to the EDPS operator? Like in any PHC setting, some simple laboratory investigations can be made available to the EDPS2000 team, namely evaluation of hemoglobin level for anemia screening, blood smears for the detection of malaria, as well as simple urine and stool analyses for diagnosis of uncontrolled diabetes and gastroenteritis. These tests can therefore be performed onsite and the test results entered in the system to provide a more complete or confirmatory evaluation of the patient's condition. For investigations that are not available on site, patients will be given a laboratory investigation requisition, i.e. a piece of paper stating the tests which are requested, which they could bring to the laboratory of their choice and have the tests done. Once the tests are completed, patients will be asked to bring the results back to the PHC (at the time of their follow up appointment, for example), so that the operator can feed this information into the system and reevaluate the patient's condition in the light of these results. A final diagnosis will therefore be provided, with the corresponding treatment (and/or referral) advices, as required. 7. What will happen when patients do require the services of a medical doctor, (for prescription of antibiotics, or for a consultation with a specialist, for example)? When the patient's condition requires that he/she is to be seen by a physician, the patient will be sent to the nearest facility (hospital, clinic, or other PHC, as required by the type and severity of the conditions). They will be provided with their EDPS2000 report (which clearly states the reason of their referral as well as the severity of their conditions), so that the doctor who sees them next can easily know what needs to be done. When wireless or telephone communication is available at the PHC, EDPS has the ability to instantly contact the physician who may be at another location for further advice. Once the patients have been taken care of appropriately and have returned home, they will be requested to bring us the results of the consultation, diagnosis and interventions done, which should be provided to them by the physician they have been referred to, so that their file can be updated. EDPS2000 patients' files will therefore be a precise and exhaustive record of all their heath related episodes, hence helping to make more adequate evaluation and monitoring of the patients overall state of health. 8. What are the statistical sections available on the system that will be of use to my practice and me? EDPS2000 statistics have been chosen according to the priorities of the health problem of rural India, and therefore covers all areas of maternal child health (including pregnancy, delivery and postpartum care, as well as children under 5 nutritional and immunization status), as well as endemic communicable diseases (namely tuberculosis, malaria, gastroenteritis and respiratory tract infections). Interestingly, these statistics can be related to both the individual patients, as well as compiled for the whole patients' population, thus providing information relevant for epidemiological surveillance. Using EDPS2000 would therefore allow doctors to know more about their patients’ past medical history (whether they had a previous high risk pregnancy, are followed for tuberculosis therapy or have recently suffered from a severe dehydration following an episode of gastroenteritis). It will also allow them to know the most important problems of their region such as the prevalence of high-risk pregnancies, the incidence of malaria or the percentage of young people drinking alcohol, for example. This kind of information is useful to improve the care of individual patients, (by realizing that a specific child is due for vaccination for measles, for example), to detect epidemics at an early stage, and to prevent or treat disease (a rise in goiter cases may need urgent distribution of iodinated salt, for example). EDPS2000, therefore, helps to improve the quality of individual care of patients, as well as tracks the public health needs of our population. With it we can provide more complete and efficient care to improve the overall health status of the population we serve. Annex A List of EDPS2000 diagnoses 1) NUTRITION RELATED CONDITIONS
- Malnutrition* Kwashiorkor
- Marasmus* Vitamin A deficiency
- B Complex deficiency* Scurvy (Vitamin C deficiency)
- Rickets (Vitamin D deficiency)* Iron deficiency anemia
- Iodine deficiency (goiter) 2) INFECTIOUS DISEASES VIRAL
- HIV * Japanese B Encephalitis
- Measles * Dengue fever
- Mumps * Poliomyelitis
- Rubella * Hepatitis A & B
- Chickenpox * Rubella (German measles)
- Influenza * Gastroenteritis
- Rabies * Herpes Zoster BACTERIAL
- Diphtheria * Tuberculosis
- Anthrax * Food poisoning
- Whooping Cough * Tetanus
- Strep. Throat * Leprosy
- Staph. Skin * Dysentery
- Typhoid/paratyphoid * Cholera PROTOZOAL
- Amebiasis * Malaria
- Giardiasis * Kala azar
- Filaria * Worm infestations STD's
- Syphilis* Trichomonas
- Gonorrhea * Chlamydia FUNGAL
- Candidiasis 3) CARDIOVASCULAR DISEASES
- Myocardial infarction (heart attack)* Angina
- Cardiac failure* Rheumatic fever
- Hypertension* Pericarditis
- Congenital heart diseases* Deep vein thrombosis 4) RESPIRATORY DISEASES
- Common cold * Influenza
- Laryngitis * Sinusitis
- Sore Throat * Acute Bronchitis
- Allergic Rhinitis* Pneumonia
- Tuberculosis * Chronic obstructive lung diseases (COPD)
- Asthma * Laryngotracheo bronchitis (Croup) 5) GASTRO-INTESTINAL DISEASES
- Hiatus hernia * Dyspepsia/Acid peptic disease
- Appendicitis * Hepatitis
- Cirrhosis * Bile stones/Gall bladder problem
- Hernia * Cancer stomach
- Lactose intolerance * Alcoholic liver disease 6) RENAL SYSTEM DISEASES
- Urinary Tract infection* Renal stones
- Prostrate hypertrophy* Nephrotic Syndrome 7) TEETH RELATED PROBLEMS
- Caries* Gum problems 8) EYE & EAR PROBLEMS
- Cataract * Blindness
- Conjunctivitis* Deafness
- Refractive errors * Acute/Chronic Otitis Media
- Glaucoma * Earache
- Inner Ear problem 9) ENDOCRINE
- Thyroid problems (hyper/hypo)* Diabetes Mellitus 10) HEMATOLOGY
- Anemia’s * Neutropenia
- Aplastic anemia * Lymphomas
- Thallasemia * Bleeding disorders
- Megaloblastic anemia * Idiopathic thrombocytopenic purpura
- Sickle cell disease * Hemophilia 11) RHEUMATOLOGICAL PROBLEMS
- Rheumatoid arthritis * Osteoporosis
- Ankylosing spondylitis * Gout
- Osteoarthritis * Osteomyelitis
- Cervical spondylosis * Lumbar disc herniation/Sciatica 12) CENTRAL NERVOUS SYSTEM
- Meningitis bacterial/ tuberculosis * Encephalitis
- Cranial nerve damage * Migraine
- Epilepsy * Stroke
- Parkinson's disease * Brain tumors 13) SKIN DISEASES
- Eczema * Psoriasis
- Urticaria * Rash
- Scabies * Burns
- Skin cancers * Warts
- Moles * Molluscum contagiosum
- Acne vulgaris * Neurofibromatosis 14) PSYCHIATRIC
- Depression * Schizophrenia 15) SURGICAL CONDITIONS
- Wounds/ Injuries * Fractures
- Abscess * Piles / Anal fissure
- Lipoma * Fistulas and sinuses
- Lumps in different organs * Varicose veins 16) GENITAL
- Pregnancy related: * Uterine prolapsed anemia & other high risks
- Cancer cervix * Vaginal discharge
- Menstrual disorders * Infertility
- Testicular swellings 17) POISONING
- Organophosphorus poisoning
- Iron poisoning / Kerosene / Sleeping pills


Log in or sign up for Devpost to join the conversation.