-
-

LOGIN screen
-
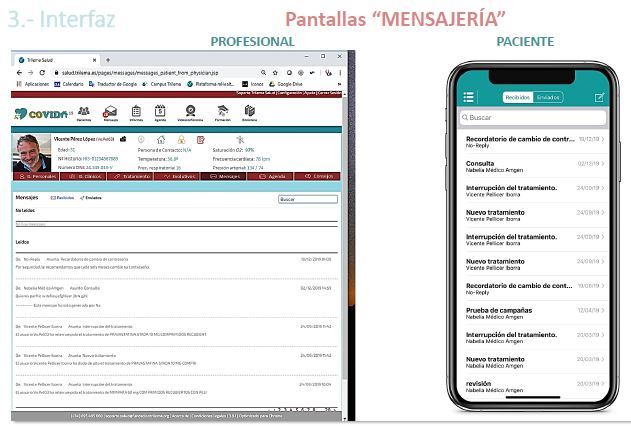
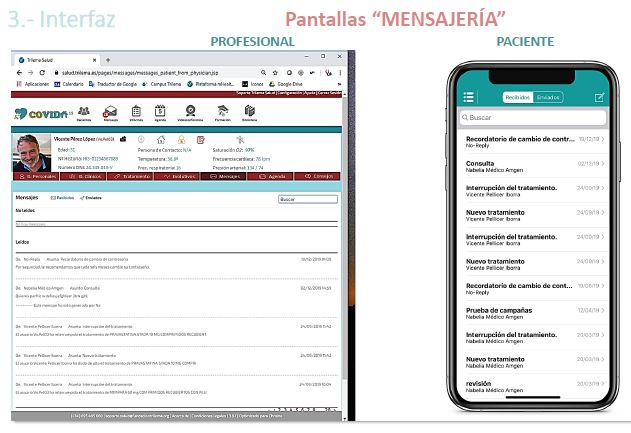
"MESSAGE" screens
-
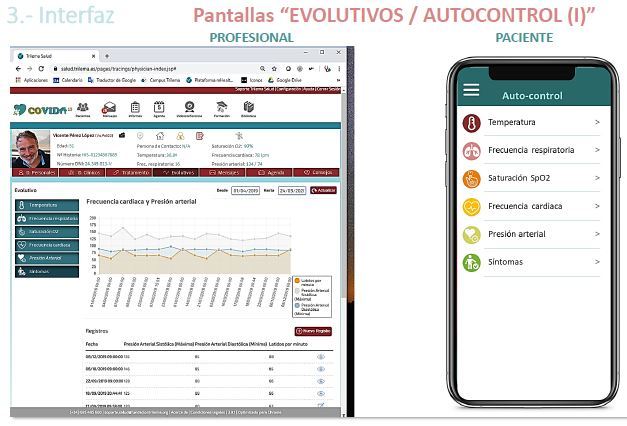
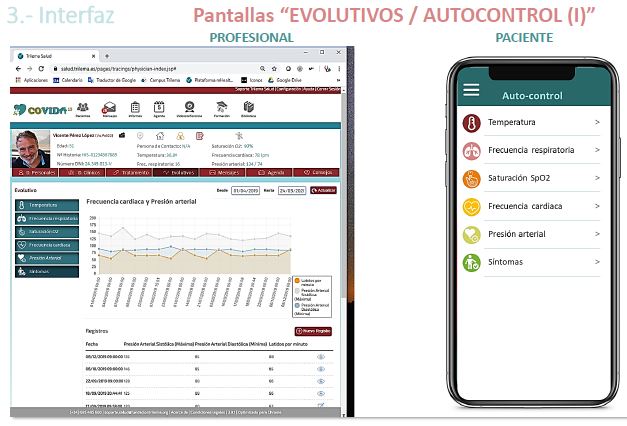
Screens "EVOLUTE / SELF-CONTROL (I)"
-
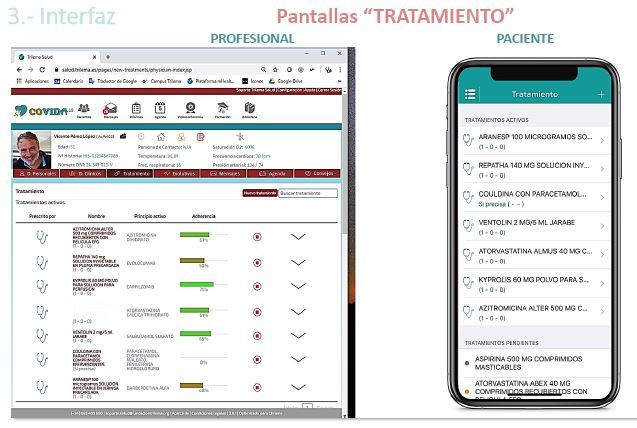
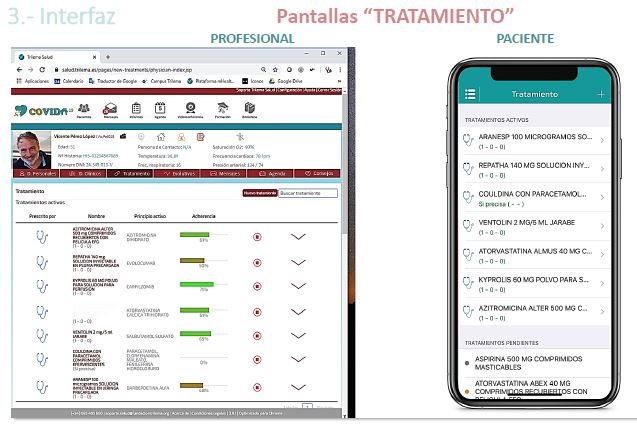
Screens "TREATMENT"
-

Screens "EVOLUTE / SELF-CONTROL (Ii)"
-
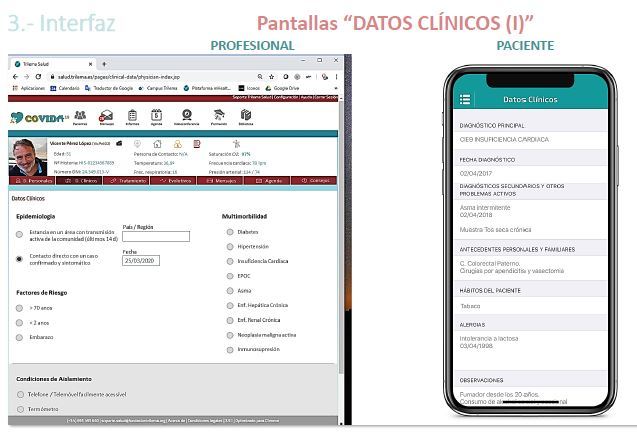
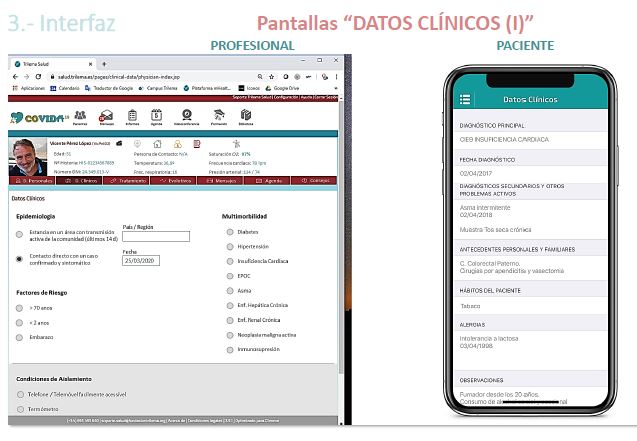
Screens "CLINICAL DATA (I)"
-
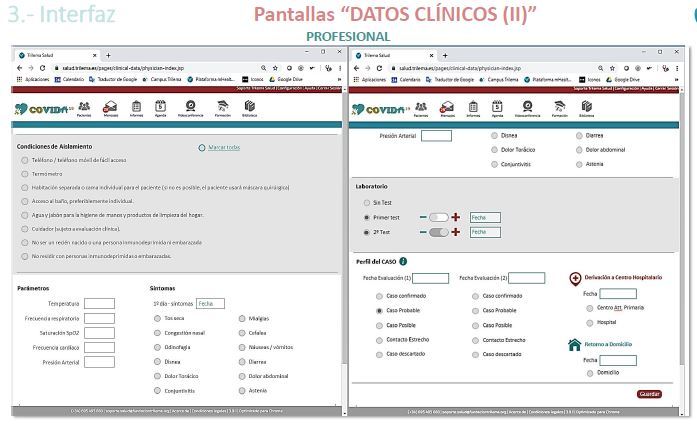
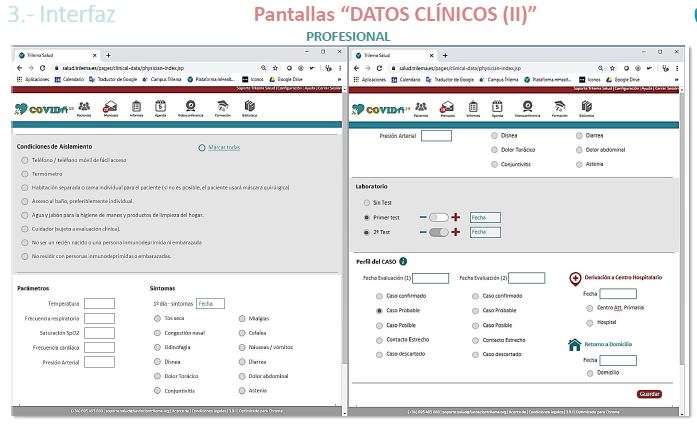
Screens "CLINICAL DATA (II)"
-
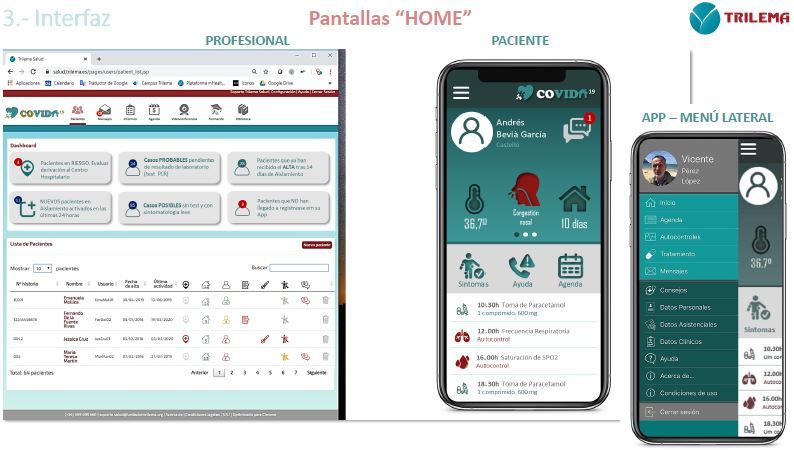
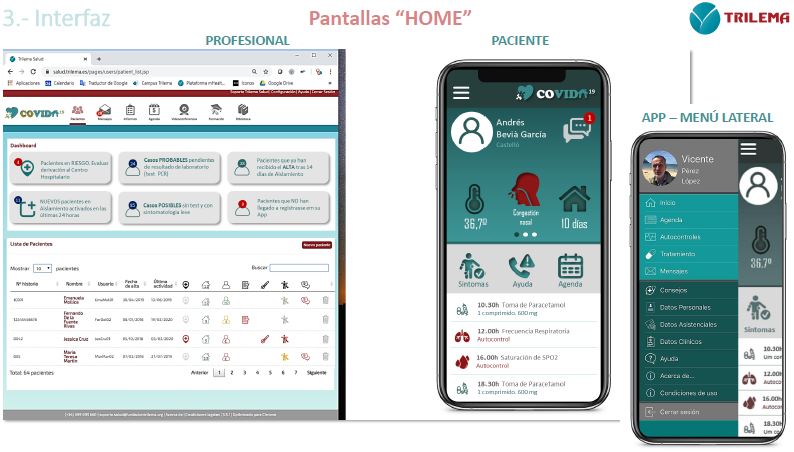
HOME screens
-
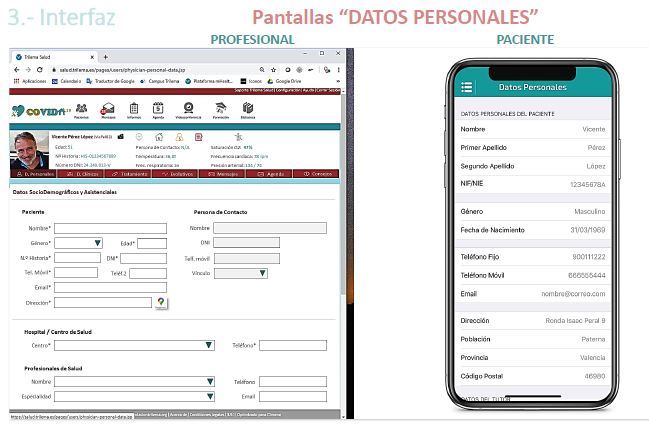
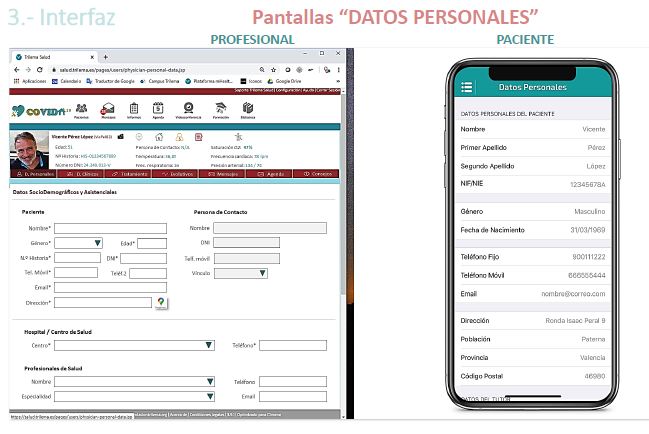
screens "PERSONAL DATA"


Inspiration
On the night of Friday, March 20, our friend and collaborator Antonio Cunha, Executive Director at the Pedro Nunes Institute in Coimbra (Portugal), called us, proposing to adapt to COVID-19 our oncological patient management platform that we already work with. "We do not have financing yet," he told us, "but it would be a very valuable initiative for Portugal and to reduce the burden on hospitals and health centers ... Furthermore, we have already discussed this with the Ministry, and they are very excited ..." Antonio was responsible for lighting the wick for this project. At same call we made a commitment to them to do it in two weeks. We felt useful in the pandemic, excited and proud to add, to contribute a very positive grain of sand to alleviate this situation. The entire technology team worked tirelessly for two weeks, including nights, Saturdays and Sundays. The scientific and public health team of the Ministry and the Coimbra Hospital met us every morning to review the protocol, the risk criteria, the list of symptoms and, of course, the translation into Portuguese of everything in a new care environment that we were building.
What it does
Most of cases of COVID-19 start with mild symptoms and go to the ER with fever and some symptoms like a flu-like process. Currently, home care and monitoring is the preferred option for the evolutionary control of possible cases or confirmed asymptomatic cases that lack other important comorbidities and present a stable clinical situation. For this, it must be ensured that the home environment is adequate for the health care of the case and that minimum requirements are met.
The objective of this proposal is the immediate implementation of a technological platform that allows the development of a safe and effective remote home care model, and that guarantees the protection of the sick and their families. The initiative reduces the on-site care burden at hospital centers and the physical presence of healthcare workers, thus helping to prevent the transmission of the disease in professionals and to decongest the public care system.
The project proposes the implementation of a telematic platform, perfectly adapted to the COVID19 protocol, which allows the patient to participate through an App and at the same time remote daily monitoring from Primary Care. It is designed for the control of patients in home isolation and / or in quarantine. The technology developed enjoys clinical validation in various trials and currently has thousands of chronic patients under remote surveillance.
How it works
The project proposes the implementation of a HealthCare platform, resident in the cloud, where professionals (doctors, nurses and primary care assistants) and patients will interact in real time. Health professionals will use the computers in their consultations and patients will use their mobile phones with the new App developed for this project and which we have called: "Health at home". Once evaluated by the primary care or specialty care doctors of what the CASE profile is (Possible, Probable, Confirmed, Discarded or Close Contact) the patient will be activated in the COVID19 program from the health center and sent home informing him/her that he/she is going into isolation, quarantine or control, depending on the profile. In the next 24 hours, the support team will contact the patient to explain the steps to follow during their isolation, evaluate their digital capacity and, if necessary, guide them in downloading the application and its management. In the following 24 hours, our support team will contact the patient to explain the steps to follow during their isolation, their digital capacity will be evaluated and, where appropriate, they will be guided in the application download and handling. The average time we will dedicate per patient is about 30 to 45 minutes
SELF-CONTROL (PATIENTS) The patient will use an App where daily and for a minimum of two weeks he will record the data of temperature, blood pressure, heart rate, respiratory rate, oxygen saturation and also select those symptoms that are active from the list established in the WHO protocol for COVID19 (headache, muscle or joint pain, sore throat, chest pain, weakness, fatigue, dry cough, coughing up blood, rhinitis, nasal congestion, shortness of breath, choking, bluish skin or mucous membrane discoloration, disorientation, severe confusion or lethargy, persistent vomiting, severe diarrhea, or conjunctivitis). The patient will be supported by a pulse oximeter and a blood pressure monitor to fill in the monitoring data on the mobile application on a daily basis. The application is available in Apple and Google stores.
MONITORING (PROFESSIONALS) Professionals have a control portal that allows daily monitoring of all patients activated in the isolation and quarantine programs. The system offers them 7 follow-up traffic lights that will facilitate control and the actions to be taken:
• Patient at RISK. Meets the criteria for referral to a hospital center • PROFILE. Case type (Possible, Probable, Confirmed, Discarded or Close Contact) • Number of days the patient has been in home isolation • NOTICE OF INACTIVITY. The patient has spent more than 36 hours without registering information on the platform. • HIGH FEVER. Temperature above 38.0ºC • DECOMPENSATION. Indicates the number of active symptoms registered by the patient • Message sent by the patient that has not yet been read by the professional team.
The established protocol for referral to hospital of patients in home care is activated with high fever ≥38.0ºC maintained for more than 48-72 hours (or reappearing after apyrexia) together with compliance with one of the following risk factors:
• Dyspnea at rest or with little effort o Respiratory rate> 30 o Signs of respiratory compromise: cyanosis and use of accessory muscles (Bluish discoloration of the skin or mucous membrane) • O2 saturation <92% • Heart rate> 125 • Hypotension (systolic <90 and diastolic <60) • Altered state of consciousness (disoriented, acute confusion, lethargy) • Hemoptises (Blood expectoration) • Persistent vomiting or severe diarrhea + It is IMPORTANT to point out that remote monitoring services may be activated for doctors and nurses confined in their own homes, either because they are in risk protocols, reserves or suspected contagion. This home scenario -also for the monitoring teams- allows to increase the safety of health personnel and activate health resources, which at this stage are essential.
In addition to the control and alert traffic lights, professionals will be able to access the evolutionary graphs of each patient and evaluate the state and criticality of the patient as well as the degree of compliance with the home protocol. The professional has powerful diagnostic tools on the platform, in addition to non-invasive communication tools with the patient or their family environment: • Baseline clinical data, profile, PCR results, comorbidities, ... • Medication and treatment. Validation of adherence and treatment compliance • Evolutionary monitoring of Biometrics (temperature, respiratory rate, HR, AT, SPO2...) • Evaluation of active symptoms • Access to the Patient Agenda, to incorporate monitoring events • Two-way messaging with patient reading control • The platform also has a section for patient support tips. In this project we incorporated the 18 recommendations of isolation, the requirements of housing adequacy and family protection measures suggested by the Ministry of Health of Spain
How I built it
• The project uses the movisalud technology developed by Grupo Trilema (www.movisalud.es) and has been fully funded by its Foundation. • The ARSC (Administração Regional de Saúde do Centro) of the Portuguese National Health System has participated in the scientific design, led by the prestigious Dr. Jose Luis Sacadura Biscaia Silva Pinto, who coordinates the "Primary Health Care" area in the Ministry of Health. • The clinical working group has also been joined by the management team of the CHUC (Centro Hospitalar e Universitário de Coimbra). The coordination of the project in Portugal is led by Sergio Sousa, Researcher & Project Manager at the IPN (Instituto Pedro Nunes) in Portugal. • It has been translated into Spanish and readapted for use by the Catalan Institute of Oncology in infected cancer patients
Challenges I ran into
When we started developing the app, we still didn't have much information about COVID-19. As COVID-19 is a virus whose treatment is unknown, we have had to change the protocol many times during the development of the application, so we have had to make a very dynamic application to facilitate the protocol change quickly.
Accomplishments that I'm proud of
We will have to remotely monitor - from the health centres - hundreds of citizens in their homes for at least 14 days. The profiles are different, we will have non-severe positive patients who are discharged from hospital and sent home to maintain this evolutionary control in isolation, we will also follow "suspicious" patients or probable cases that are waiting for the results of the evaluation tests, but with symptoms that do not justify their admission and, finally, we will have the largest group, patients with symptoms associated with lung infection whose severity does not fall within the criteria for the use of CRP, from the laboratory test, are the possible cases. The initial launch in Portugal has been scheduled for the Central Zone where 3 health centres in the Coimbra area have been selected. A care team of 7 doctors and 3 nurses has been formed to attend an initial group of 300 patients. We have also trained a small care and support team from the Pedro Nunes Institute to be able to solve the technical doubts of the patients, especially in the handling of the apps, mobile phones or medical devices. In addition, there are plans to incorporate the home care team of the Coimbra University Hospital, whose managing director, Dr. Alexandre Lourenço, has been an active participant in the project's scientific design committee. In Spain, we are also starting this week with the follow-up of the first 50 patients, in this case with an oncological profile, from ICO Barcelona (Catalan Institute of Oncology). The project is coordinated by Dr. Alberto Mussetti, immersed in the OncoHematology service of ICO, which is directed by Dr. Anna Sureda, and has the participation of a powerful multidisciplinary team that also includes psycho-oncology services from the unit of Dr. Cristian Ochoa. A gradual weekly growth in the number of patients in both regions is expected.
implementation schedule
Since we are already working in the Arnau de Vilanova - Llíria health department, we propose that this be the area for piloting the initial deployment. We have doctors, physiotherapists and nursing resources from this Centre already familiar with a very similar environment of our platform. They will be able to strengthen and facilitate our initial training for the primary care teams of the entire department. We also have close collaboration with the information systems team of this centre to activate all the health centres and professionals in the department's database.
STEP 1. Training of Professionals After the pilot, we will address the horizontal deployment in the Community using virtual training by videoconference to selected nursing staff of health centers (ideal to train two people from each health center). Users will also have downloadable training guides and video-demos to support the use of the platform. The handling is intuitive, and the interface is friendly, as shown in the slides above. Once the case has been categorized (type of profile) and it has been decided to move it to the home care model, the primary care nurses will be in charge of activating the patient in the system. An average time of between 6 and 8 minutes is estimated for activating a patient on the platform, with the registration of their basic personal data and their baseline clinical data - as required by the public health protocol - (epidemiology, risk factors, multimorbidity, validation of isolation conditions, parameters, symptoms, PCR laboratory and case profile).
Step 2. Patient Training In TRILEMA we currently have a call center service for the attention and technical support to patients who use our platforms. This is a technical care service, not clinical, where we educate users in the handling of technology and solve their doubts and incidents, especially related to their mobile phones. It is not an assistance service but a technical and pedagogical support. We train our patients through phone calls. The initial training of a "non-digital" patient takes 30 to 40 minutes. The "digital" patients are autonomous in the use of the App. In the TRILEMA group we have the ownership of educational centres in the communities of Madrid, Valencia and Castilla León. In some of our centres we provide professional training for nursing assistants. For this project, our students and ex-students of the health FP's will be able to reinforce a predictable and massive demand for services, both for patient training, and for support and incident care.
Step 3. Activation of Isolation Once the professional teams are trained, the primary nurses will activate the patients on the platform and send them home under an isolation or quarantine scenario for 14 days along with a kit of two devices, a pulse oximeter and a blood pressure monitor. The patient who meets "digital culture" criteria or who has family members who can take care of self-care on the mobile phone will start their home self-care plan according to the protocol.
Step 4. Report Dump in the Ambulatory History (ABUCASIS - SPAIN) It is probably easier to upload reports from our platform to the clinical history of Abucasis than to create the COVID19 protocol, with patient self-monitoring parameters, in the corporate systems of the Ministry of Health, especially if it has to be done in record time. In addition, the technological models of architecture where thousands of users outside the GVA attack from their mobile phones to the internet ports of the GVA network itself is practically unthinkable in terms of security. That is why our proposal will be to dump in the history of the patient a complete report that includes the complete episode of the 14 days with all the information entered, the evolutionary graphs, the pharmacological treatments, compliance, symptomatology and decompensation, parameters of Biomedidas, etc. We will propose a complete model report for the approval of the Regional Ministry. Currently we are already publishing HL7 reports of Personal Health Folder in HC3, the Shared Clinical History of Catalonia, through integration with the SAP of the Hospital Sant Pau in Barcelona. We are also finalizing the connection with Diraya and the corporate health systems of the Junta de Andalucía. The TRILEMA platform is designed under semantic interoperability standards that facilitate this type of integration.
Schedule. An "express" launch
Week 01 • Closing of agreement, conditions, requirements, final functionality and award. • Purchase of the first 2,000 medical devices (blood pressure and pulse oximeters) Week 02 • Technological adaptation of the platform, professional access and patient access. • Preparation of Manuals, Cards and Video Guides. • Reception of medical devices and distribution by department Week 03 • Publication of Apps and Usage Tests • Training for Arnau de Vilanova teams Week 04 • Launch of the Arnau-Lliria Department Week 05 • Launching of the rest of the Departments according to the Plan drawn up by the Regional Ministry
Team
To achieve the committed deadlines we count on a great asset, our Health SW development team, a human group committed to work at 200% for this initiative: • Vicente Pellicer (Area Director, functional manager) • Fernando de la Fuente (Analyst and Department Head) • David Fernandez (Architecture, Quality and Integration) • Eduardo Castellanos (Back End Development) • Micael Fernandez (Back End Development) • Adrian Bonilla (Front End Development) • Jaddou Nasra (Front End Development) • Angel Martin (Mobile Development) • Ivan Alvarez (Mobile Development) • Olga Espino (Web Design and Development) • Victoria Martínez (Project manager)
The protocol and the advice to all the staff of our support team (call center) that attends and trains the patients oversees our colleagues of the teaching area specialized in assistance: • Gemma Ferrer (Pharmacist) • Inés Gómez (Nurse) • Carmen Moyano (Nurse) • Lluís Faus (Nurse) • Martin Varela Pavón (Spanish in clinical psychology)
What I learned
During the development of Health at Home we have learned to develop an application that is fully configurable. Establishing a development base, being able to add controls and evolutions to the patient's protocol without having to modify the application code. The API gets all the protocol and controls from the database, so it is very easy to add or remove controls, clinical data, personal data or questionnaires to the protocol.
What's next for HEALTH AT HOME
We firmly believe that the movisalud technology adapted to the COVID-19 is a great assistance asset at this time and should not be limited to two regions, we are very interested in opening up the technology and offering it to ALL hospitals and health providers that decide to make use of it. We think this pandemic will be the turning point towards a new model of care more focused on the patient, more home-based, more technological and, of course, more human
Built With
- amazon-web-services
- android
- hibernate
- hibernate-persistent-layer
- ios
- java8
- jquery
- objective-c
- spring-4.5
- using-the-spring-4.5-framework.-?-hibernate-for-the-persistence-layer.-?-for-the-web



Log in or sign up for Devpost to join the conversation.