-
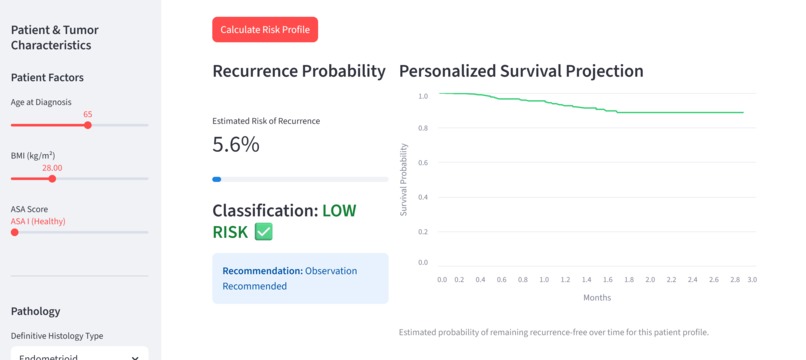
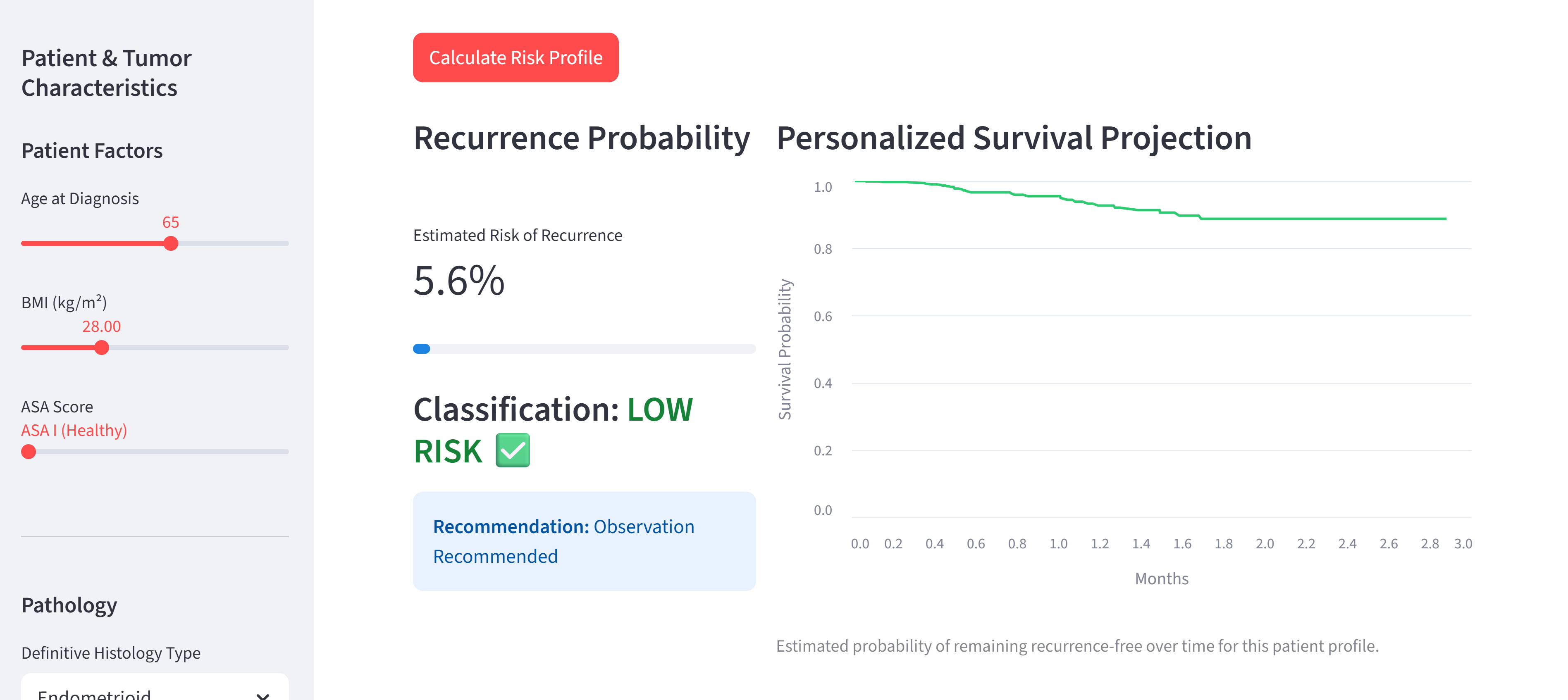
low risk classification example
-
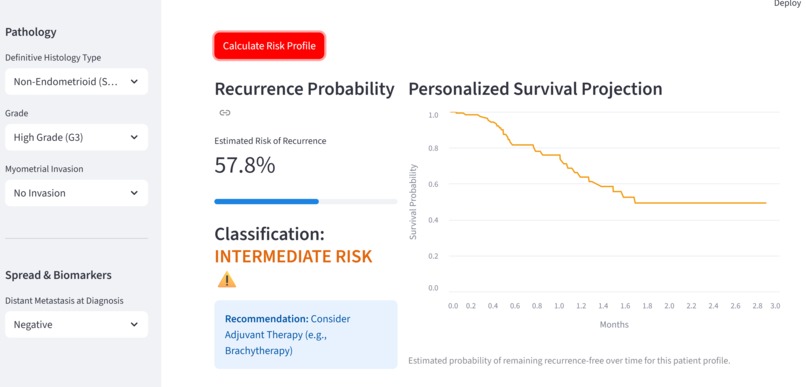
intermediate risk example
-
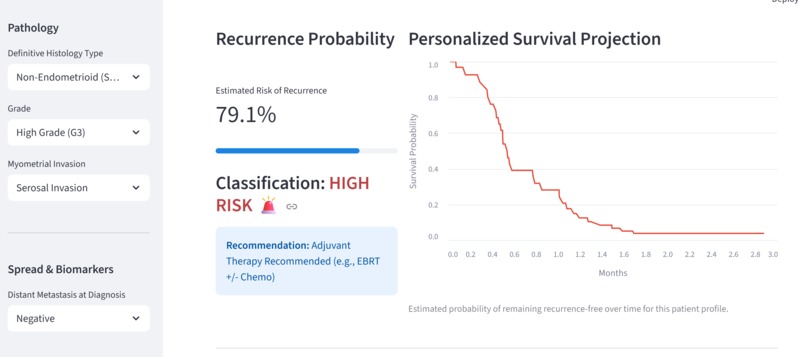
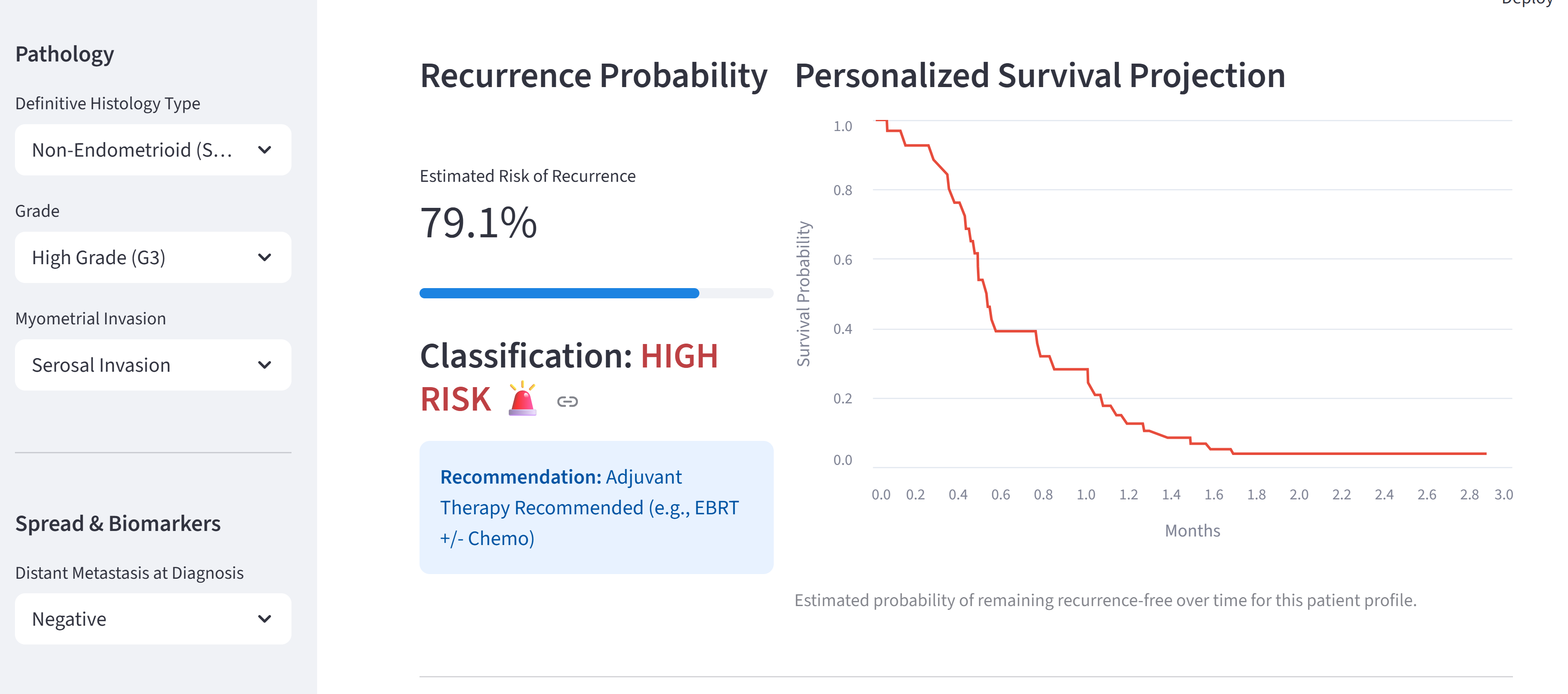
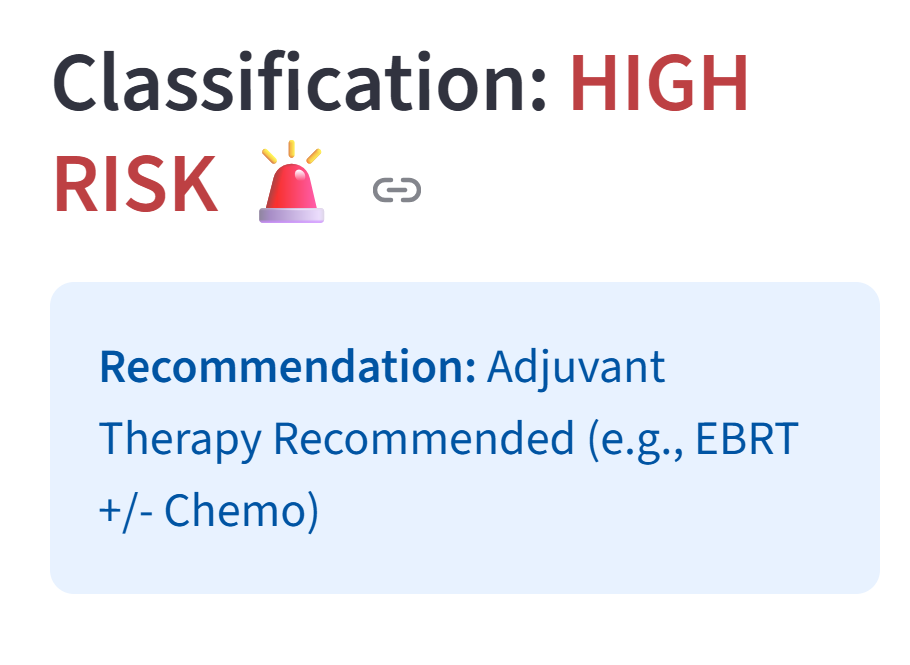
high risk example
-
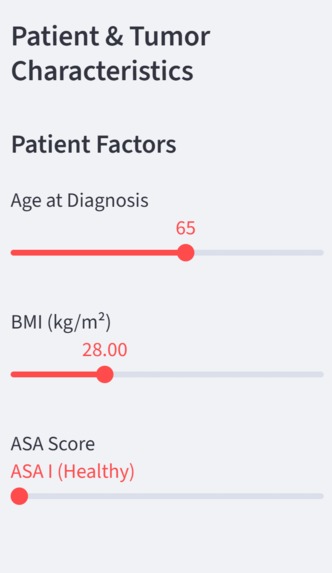
digital calculator features part 1: age, bmi, ASA score
-
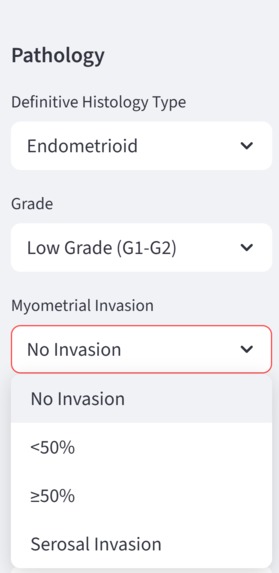
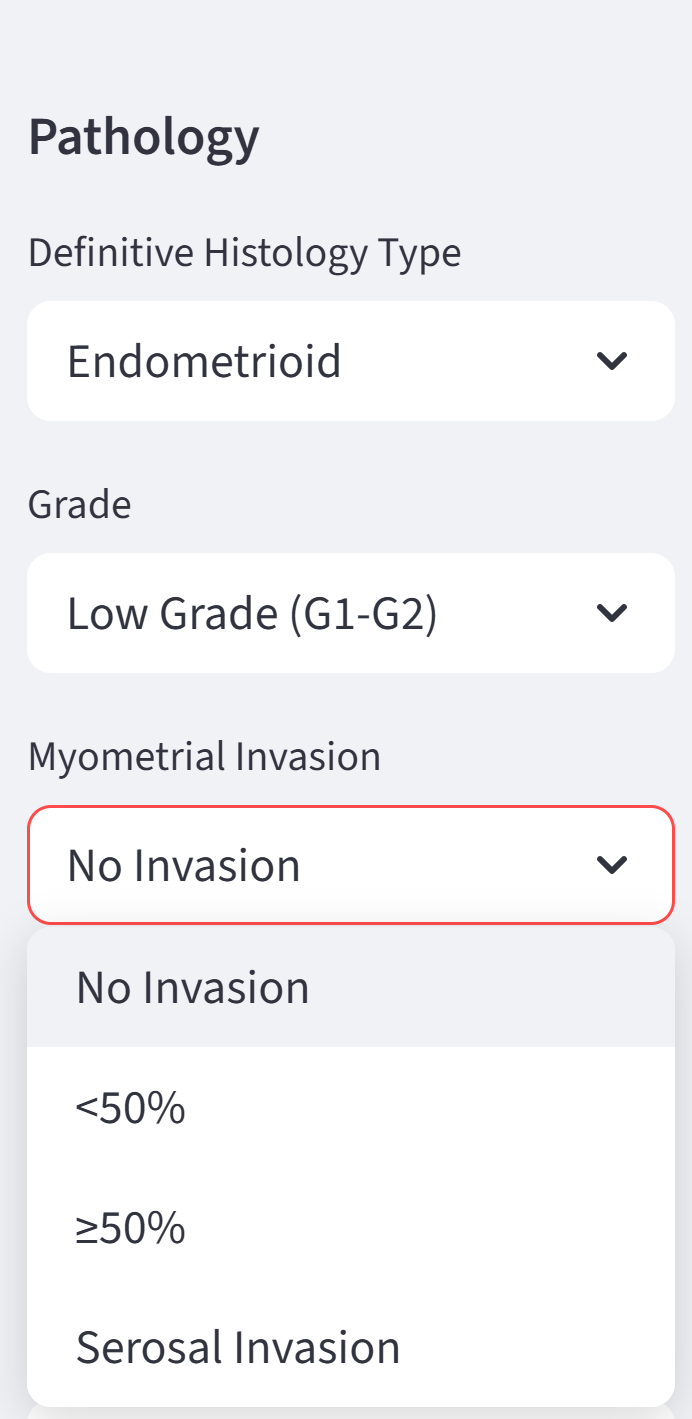
digital calculator features part 2: histology type, grade, myometrial invasion
-
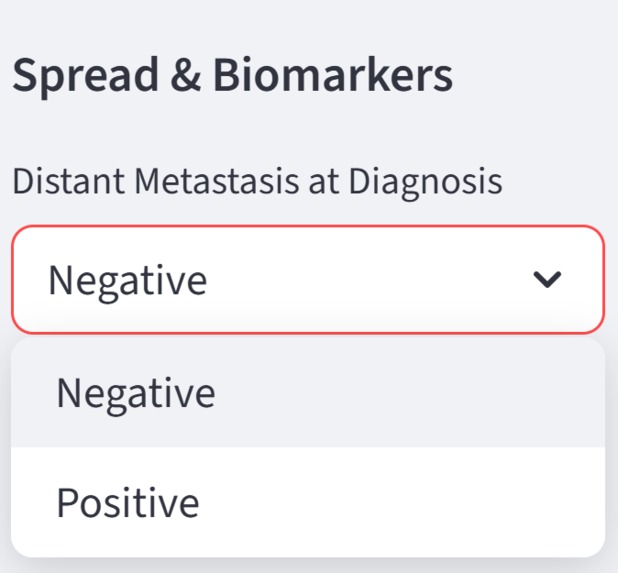
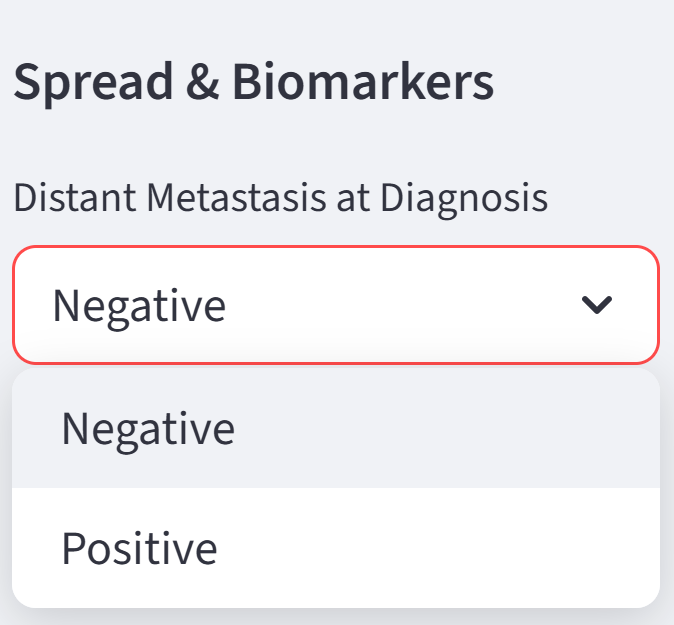
digital calculator features part 3: distant metastasis
-
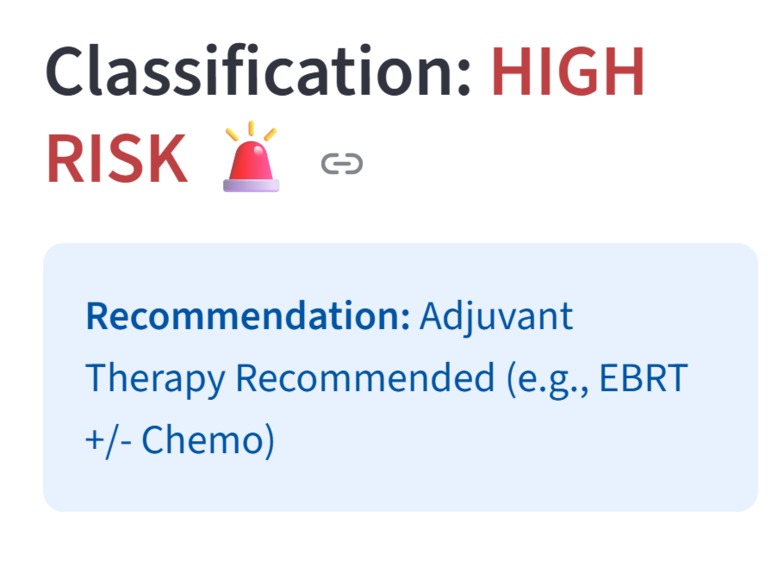
The treatment recommendations are based on the 2023 Oncoguía SEGO guidelines


Project Story — NSMP Endometrial Cancer Risk Calculator
1. The Problem
Endometrial cancer patients with a Non-Specific Molecular Profile (NSMP) represent a large and heterogeneous group. At diagnosis, clinicians must decide how aggressive treatment should be, but current risk stratification is largely post-operative and does not fully leverage all available preoperative clinical information.
This creates two major challenges:
- Potential overtreatment of low-risk patients
- Delayed intensification for patients at high risk of recurrence
2. Our Goal
Our goal was to develop a transparent, data-driven risk stratification tool that:
- Uses information available at the time of diagnosis
- Predicts recurrence risk and recurrence-free survival
- Translates model outputs into clinically interpretable risk groups
- Provides guideline-aligned treatment recommendations
3. The Data
We worked with a real-world clinical dataset of NSMP endometrial cancer patients including:
- Patient factors (age, BMI, ASA)
- Preoperative pathology (histology, grade, myometrial invasion)
- Disease spread indicators (distant metastasis)
- Longitudinal outcomes (recurrence, death, follow-up time)
We carefully:
- Cleaned and harmonized variables
- Handled missing values
- Translated clinical fields into model-ready features
- Restricted features to those available preoperatively
4. Modeling Strategy
We implemented a two-model approach:
🔹 Classification model (Random Forest)
- Outcome: Recurrence / recurrence-related death
- Output: Individual recurrence probability
- Purpose: Assign patients to Low / Intermediate / High risk
🔹 Survival model (Cox proportional hazards)
- Outcome: Recurrence-free survival
- Output: Personalized survival curves
- Purpose: Estimate when recurrence risk accumulates over time
This combination allows both risk ranking and time-to-event interpretation, which is crucial in oncology.
5. Risk Stratification
Patients are grouped into:
- Low risk – very low observed recurrence
- Intermediate risk – moderate recurrence risk
- High risk – substantially higher recurrence rates
We validated the stratification by showing that:
- Observed recurrence rates increase monotonically across groups
- High-risk patients truly experience more events
6. Clinical Interpretability
To ensure clinical trust:
- We examined hazard ratios from the Cox model
Key drivers of recurrence included:
- High tumor grade
- Deep myometrial invasion
- Non-endometrioid histology
These align closely with known clinical risk factors and international guidelines.
7. The Digital Calculator
We translated the models into a web-based Streamlit application that:
- Accepts diagnostic-time inputs only
Outputs:
- Recurrence probability
- Risk group
- Personalized survival curve
Displays clear, guideline-aligned recommendations
Requires no installation and runs in any browser
8. Impact
Our tool:
- Enables earlier risk stratification
- Supports personalized treatment discussions
- Reduces unnecessary treatment for low-risk patients
- Flags high-risk patients earlier for intensified care
This approach bridges machine learning, survival analysis, and clinical decision support in a transparent and practical way.
9. Future Directions
- External validation on multi-center cohorts
- Integration of molecular markers when available
- Prospective evaluation in clinical workflows
Built With
- python
- streamlit

Log in or sign up for Devpost to join the conversation.