
Inspiration
In Rural areas its hard to find medical facilities on demand in crucial times, I had saw people dying as the health facilities are too poor in remote areas.
What it does
Our project connect remote people through mobile phone just by dialling their area pin code which could map their nearby local NGOs and Hospitals which would then connect to each other and immediate Medicare would be provided to them.
How I built it
I built this by using exotel APIs really these services are very helpful where internet facilities are difficult to reach for this we will just require a mobile phone and mobile network.
Challenges I ran into
Segregate all NGOs on the basis of their area pincode as well as the services which they provide to people
Accomplishments that I'm proud of
It can connect to the whole India even when the internet is out of reach to some parts.
What I learned
How telephonic services at the back-end works, thanx to Exotel guys, they make me learn a lot. Now I cant say that i had not learn anything from INOUT
Abstract
Mobile technologies are increasingly growing in developing countries like India. There have been several new researches and developments in this space. Nowadays mobile is becoming an important ICT tool not only in urban regions but also in remote and rural areas. The rapid advancement in the technologies, ease of use and the falling costs of devices, make the mobile an appropriate and adaptable tool to bridge the digital divide. Mobile phone ownership in India is growing rapidly, six million new mobile subscriptions are added each month and one in five Indian's will own a phone by the end of 2007. By the end of 2008, three quarters of India's population will be covered by a mobile network. Many of these new "mobile citizens" live in poorer and more rural areas with scarce infrastructure and facilities, high illiteracy levels, low PC and internet penetration. The availability of low-cost mobile phones and the already broad coverage of GSM networks in India is a huge opportunity to provide services that would trigger development and improve people’s lives. This paper explores the present status of Mobile based Health Care systems in different countries, shortfalls in Primary Health Care Management in rural India, and the potential solution to fill it with the enabling of Mobile Web technologies for Primary Health Care management.
Introduction
According to the ITU, the total number of mobile users worldwide as of late 2006 was about 2.7 billion and the number of Internet users was just above 1.1 billion. This means that at least there is 23.6% of world population (and at least 22.2% of developing countries’ population) who already have mobile phones but are not yet using the Internet. Mobile services are quickly emerging as the new frontier in transforming government and making it even more accessible and citizen-centric by extending the benefits of remote delivery of government services and information to those who are unable or unwilling to access public services through the Internet or who simply prefer to use mobile devices. In theory, many government services can be now made available on a 24x7x365 basis at any place in the world covered by mobile networks, which today means almost everywhere. Approximately 50%–60% of government services including Primary Health Management can be delivered via mobile channel.
Primary Health Care Services using Mobile Devices ensures improved access to primary healthcare and its gate-keeping function leads to less hospitalisation, and less chance of patients being subjected to inappropriate health interventions.
Objective
The objective of this paper is to bring out status of mobile devices based Health care management systems in the world particularly in India and present the details of Mobile based Primary Health Care Management System under development by CDAC, Electronics City for deployment in the PHCs in rural India.Mobile technology for Health Care
Amongst the many ICT options available to govt to improve the efficiency& effectiveness of its delivery process of primary health care, mobile & wireless technologies offer some exciting opportunities for a low cost, high reach service. There is strong evidence that mobile technologies could be instrumental in addressing slow response rates of govt to citizen requests, poor access to services, particularly for low-income and marginalised populations in under-serviced rural areas. In addition, mobile technologies offer significant opportunities for improving the back-office operations of govt. In addition, many primary healthcare clinics located in the rural areas do not have any electronic systems at all & continue to operate paper- based systems, resulting in patient records being kept by patients themselves. The impact of the use of multiple systems is that it is difficult& costly to develop a national overview of patient statistics. On a more basic level, it is extremely difficult for idividual institutions within the healthcare sector to share information between each other. One of the clearest examples of this is to be found in the sharing of patient laboratory results. Currently in most instances, this only takes place through manual exchange. Many vendors of Cellular phones started to embed a variety of e-health services in Mobiles
Systems in India.
A number of Organisations have been working on various projects for enhancing the role of ICT in Health care. UK-based Loughborough University's engineers have entered upon a partnership with experts of India to develop a unique mobile phone health monitoring system. The system, which was first unveiled in 2005, uses a mobile phone to transmit a person's vital signs, including the complex electrocardiogram (ECG) heart signal, to a hospital or clinic anywhere in the world. Professor Bryan Woodward and Dr Fadlee Rasid from the Department of Electronic and Electrical Engineering at the Loughborough University have developed this mobile phone monitoring system. Presently the system can transfer the signals pertaining to the ECG, blood pressure, oxygen saturation and blood glucose level. Now the UK-India Education and Research Initiative (UKIERI) has awarded Professor Woodward a grant to further develop this mobile phone monitoring system. They have tied up with the Indian Institute of Technology Delhi (IIT Delhi), the All India Institute of Medical Sciences and Aligarh Muslim University and London's Kingston University, to further develop the system.
The research team is aiming to miniaturise the system, through designing sensors and mini-processors that are small enough to be carried by patients, and at the same time procure biomedical data. The network of sensors would be linked through a modem to mobile networks and the Internet, and to a hospital computer. Then, doctors can use this device to remotely monitor patients suffering from chronic diseases, like heart disease and diabetes, which plagues millions across the world. The UK government will promote the device to improvethe efficiency of healthcare delivery. In India, the project will link clinics and regional hospitals in remote areas to centres of excellence. The clinical trials of the system will take place in the UK and India in the next three years.
- Sehat Saathi, a rural telemedicine system is being developed at Media Lab Asia research hub at IIT Kanpur. It can be used to extend medical care to patients in the remote parts of the country. The model provides for front-end contact through a suitably trained non-medical professional; back end support from doctors, pathologists and other health professionals for diagnosis and treatment; use of digital technology to achieve objects; and dissemination of information on health and disease through digital means. MLAsia has taken up a project with AIIMS for use of handheld computers (palm-tops) for healthcare data collection and planning.
Primary Health Care
The Vancouver Island Health Authority defines Primary Health Care as the range of services individuals and communities receive on a regular, ongoing basis in order to stay healthy, get better, manage ongoing illness or disease, and cope with end of life. In India, Primary Health Centers (PHCs) are the cornerstone of rural healthcare; a first port of call for the sick and an effective referral system; in addition to being the main focus of social and economic development of the community. It forms the first level of contact and a link between individuals and the national health system; bringing healthcare delivery as close as possible to where people live and work.
Primary healthcare services substantially affects the general health of a population, however many factors undermine the quality and efficiency of primary healthcare services in developing countries. The World Health Organisation (WHO) specifically points out that to some extent, the deterioration in health status in developing countries is attributed to inadequacies in PHC implementation, neglecting the wider factors that have been responsible for this deterioration such as lack of commitment, inadequate allocation of financial resources to PHCs and community participation [2].
Primary Health care in India. In India, although there are many reasons for poor PHC performance, accessibility is one of the major obstacles. The public health system is managed and overseen by District Health Officers. Although thre are qualified doctors, PHCs have barely able to utilize due to non-usage of IT and Mobile access. The rural primary public health Infrastructure has recorded an impressive development during the last 50 years of independence. The network consists of 1,45,000 sub-centres, 23,109 primary health centres and 3222 community health centres, catering to a population of 5000, 30,000 and 1,00,000 respectively (and 3000, 20,000 and 80,000 population in tribal and desert areas)[3]. Each PHC is targeted to cover a population of approximately 25,000 and is charged with providing promotive, preventive, curative and rehabilitative care. This implies offering a wide range of services such as health education, promotion of nutrition, basic sanitation, the provision of mother and child family welfare services, immunisation, disease control and appropriate treatment for illness and injury. The PHCs are hubs for 5-6 sub-centres that cover 3-4 villages and are operated by an Auxiliary Nurse Midwife (ANM). These facilities are a part of the three tier healthcare system; the PHCs act as referral centers for the Community Health Centres (CHCs), 30-bed hospitals and higher order public hospitals at the taluka and district levels. Mobile based Primary Health Care Management System
CDAC, Electronics City, Bangalore has initiated the development of “Mobile based Primary Health Care Management System” for deployment in the PHCs for betterment of management of Primary Health Care specifically in the rural and urban slums of India. The system will capture of complete information related to an individual patient treated by a PHC. The Software components under development are Patient Database management, Interaction between doctor and a patient, capture of Medical data acquisition- such as ECG, images of heart & lung, eye etc and Scheduling management. The project involves development of the following: (a) A Web based Information system for Management of Primary healthcare. (b) SMS interface for integrating SMS messages from the patients using 2nd Generation mobile systems (GSM/CDMA) with the Information system. (c) Development of Localization Support to National and other Indian languages in mobiles by providing interface for translation.
System Overview
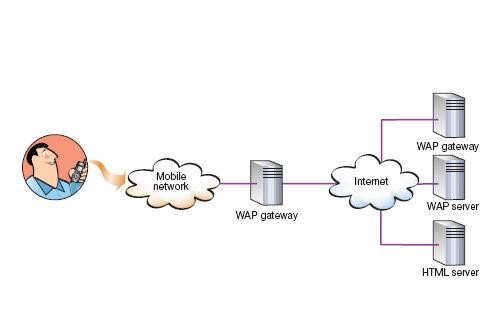
A Central repository of Primary Health Center management System with a Web interface is proposed to be developed in an Open source database. An SMS based interface to the Web is planned to be added for integrating with 2G (GSM/CDMA) telephones, since Mobiles have penetrated overwhelmingly in rural India. A WAP web Gate way will be developed for integrating with a GPRS/3G mobile devices, which are expected to be used by Doctors and Health Assistants. In case of GPRS/3G systems, the Web request from the phone is first served by the WAP Gateway Server. The gateway server translates mobile phone requests (WAP) into HTTP requests and sends them to Web server. The Web server processes the request, and sends WML to gateway server, which in turn sends the WML to phone in the binary compressed WML format.






Log in or sign up for Devpost to join the conversation.