-
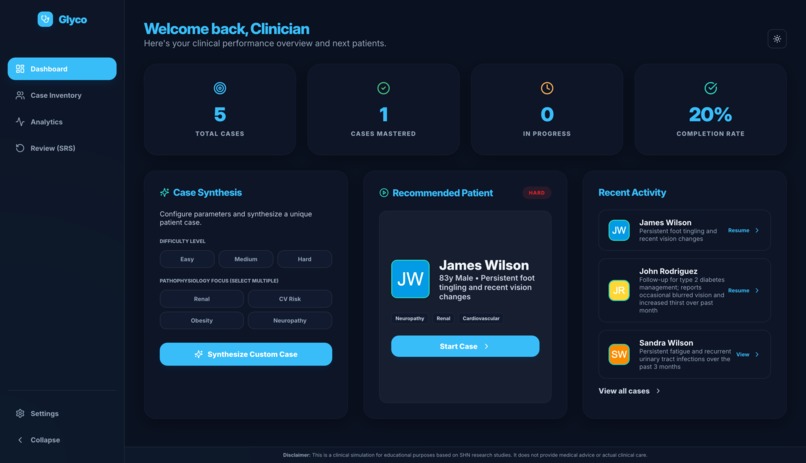
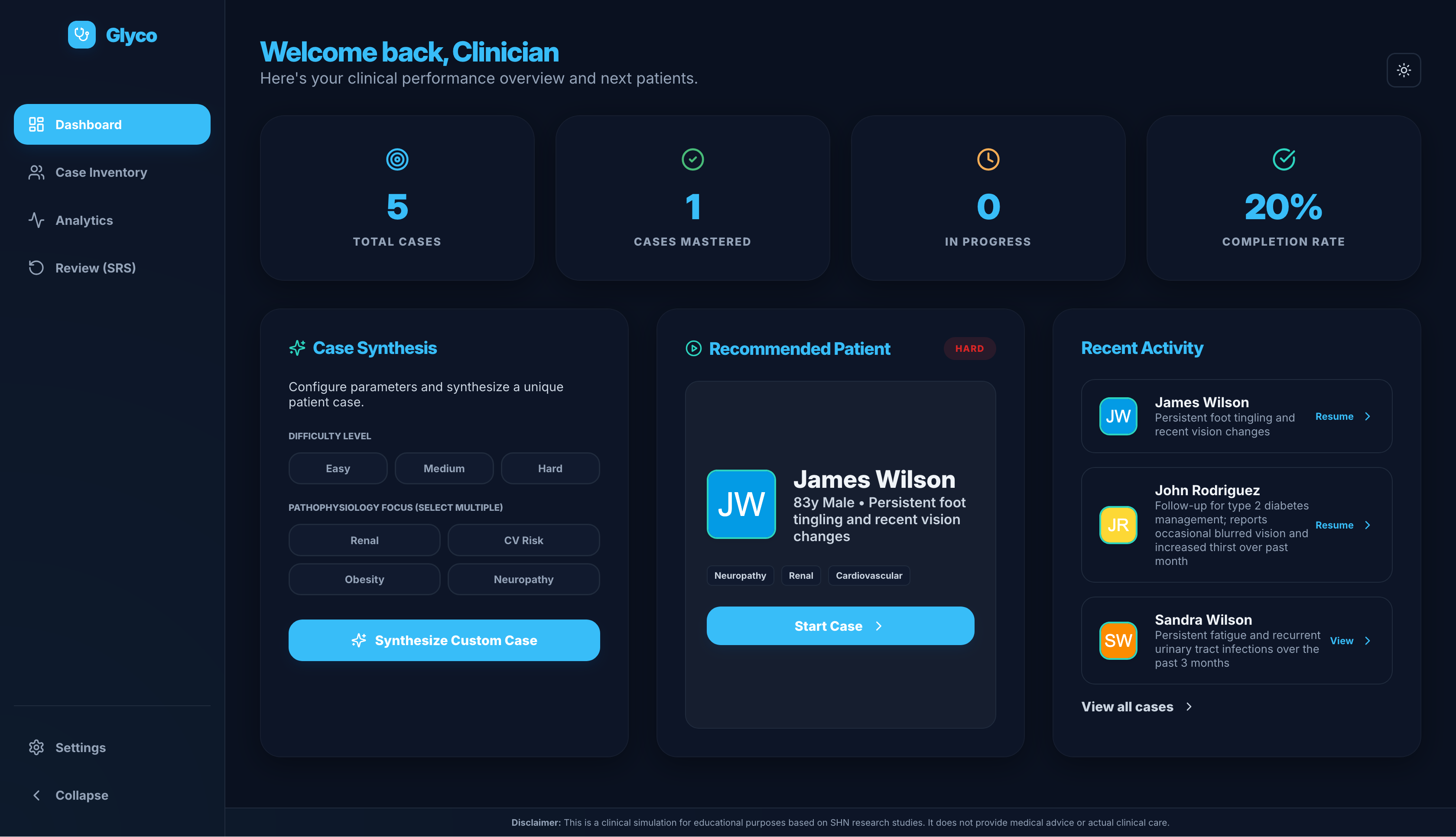
Dashboard view
-
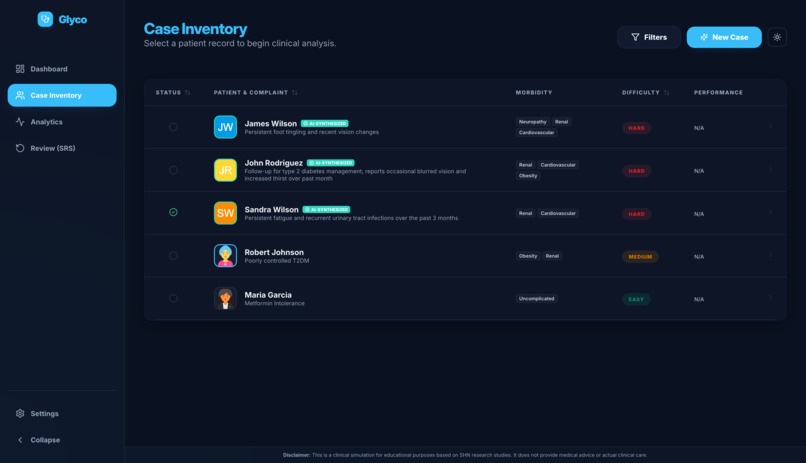
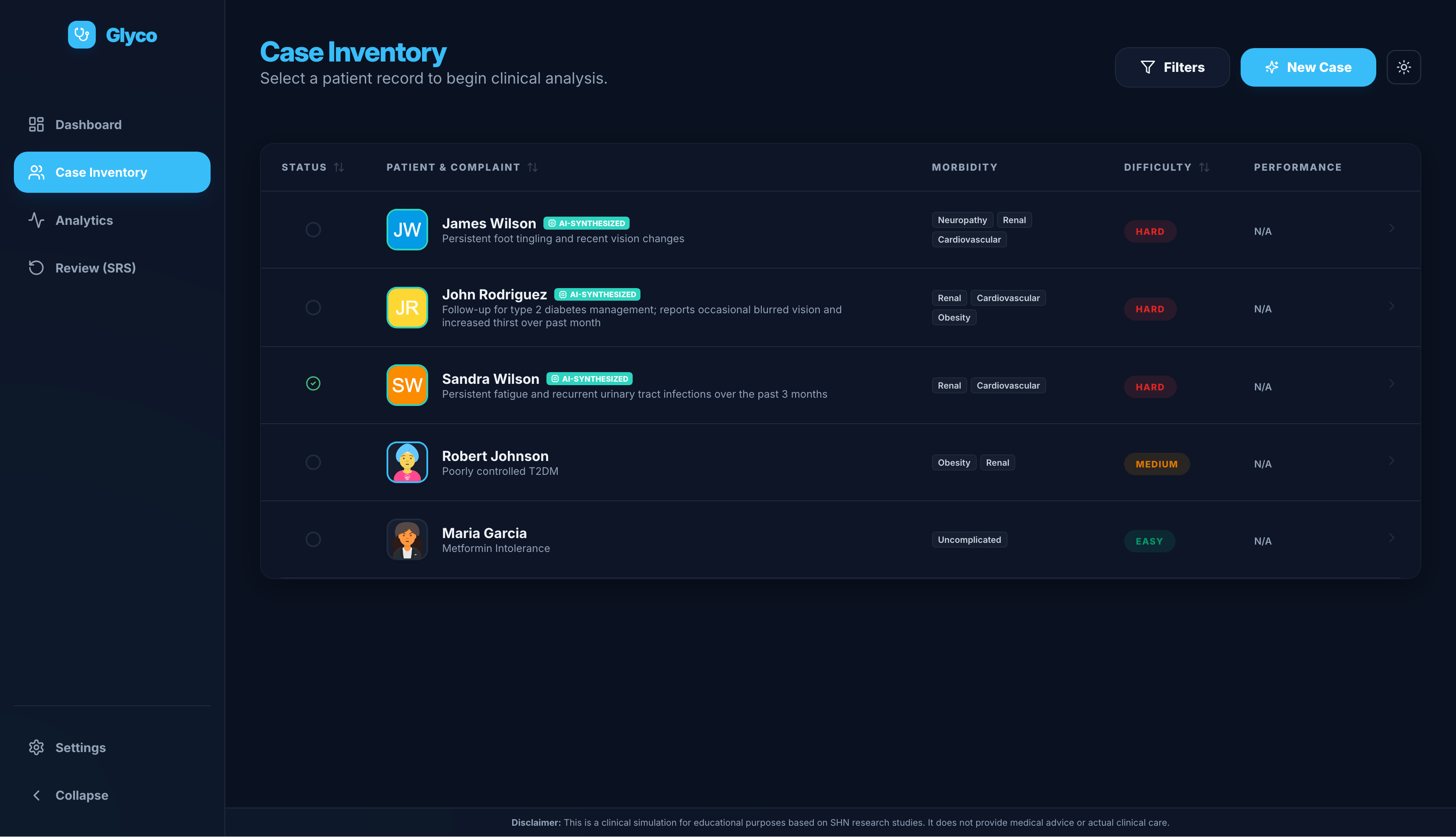
Case inventory
-
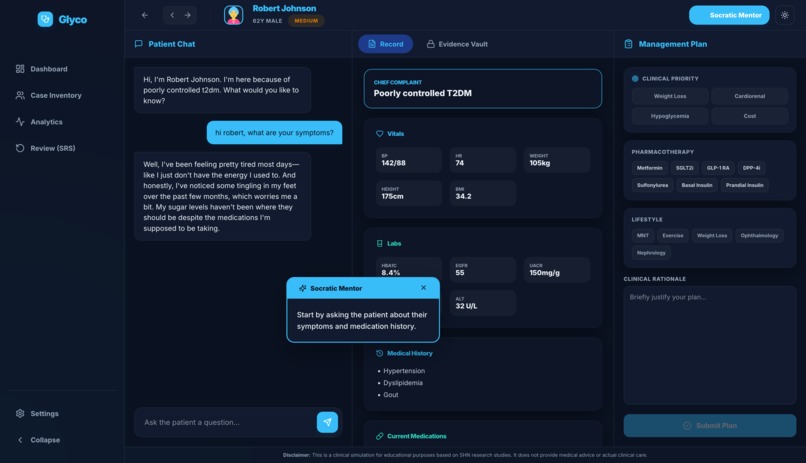
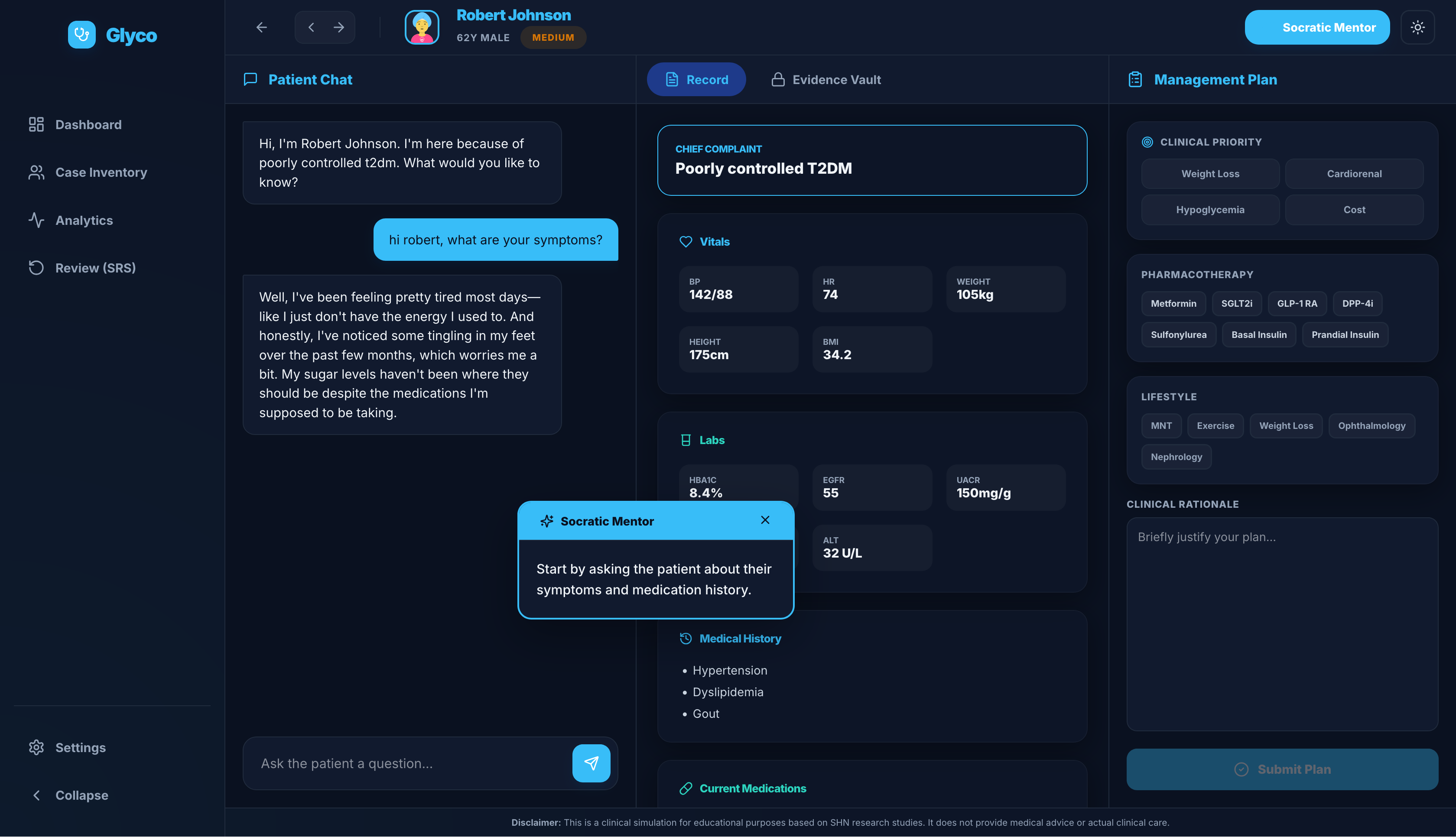
Patient view
-
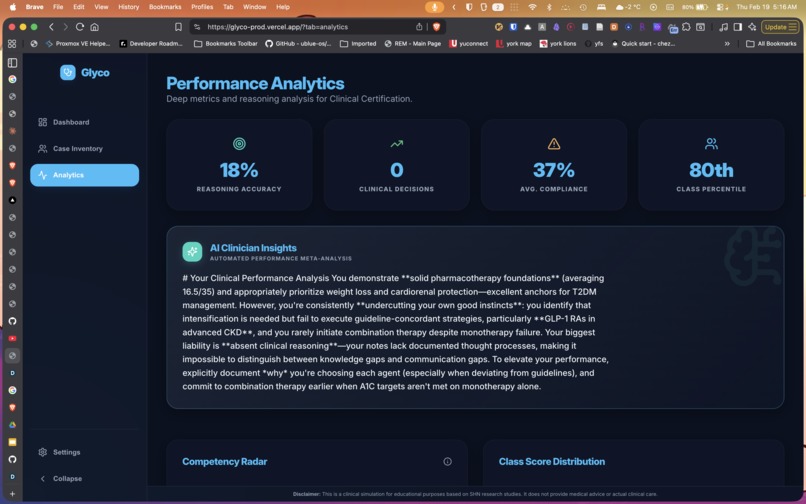
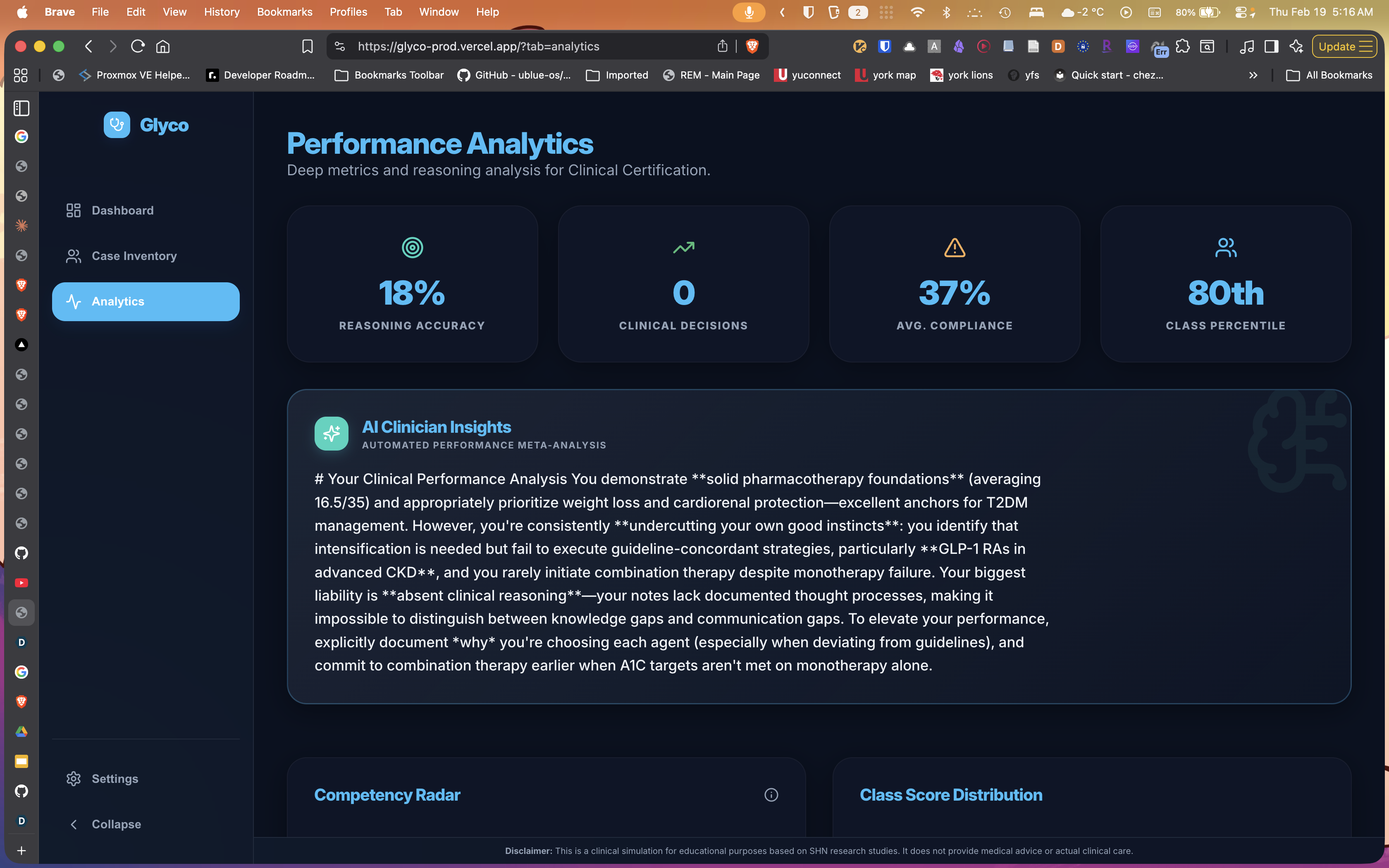
Analytics view
-
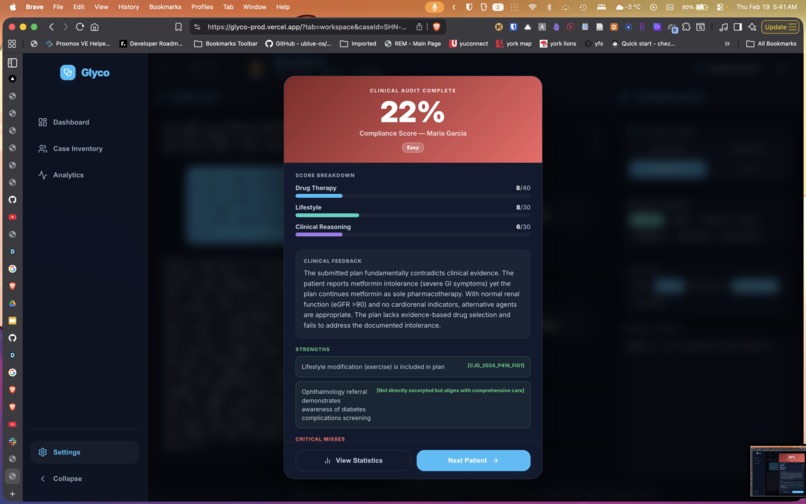
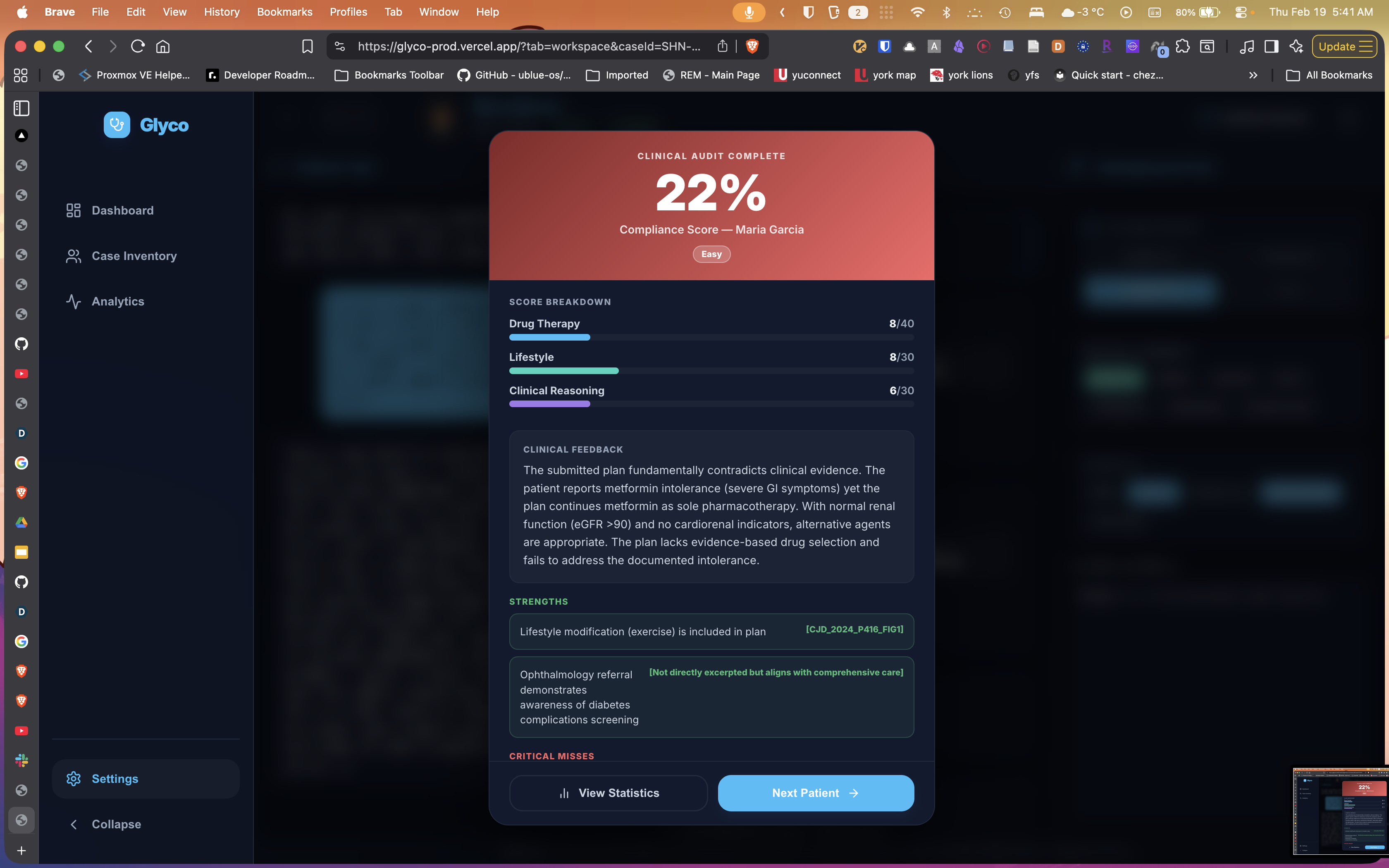
Score view
-
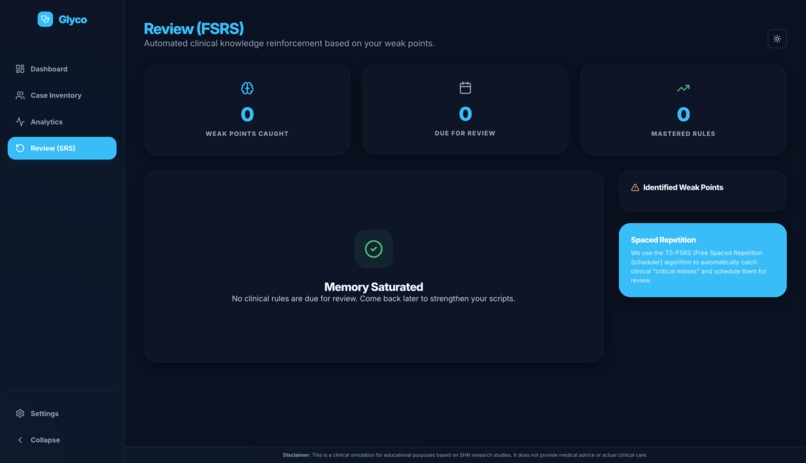
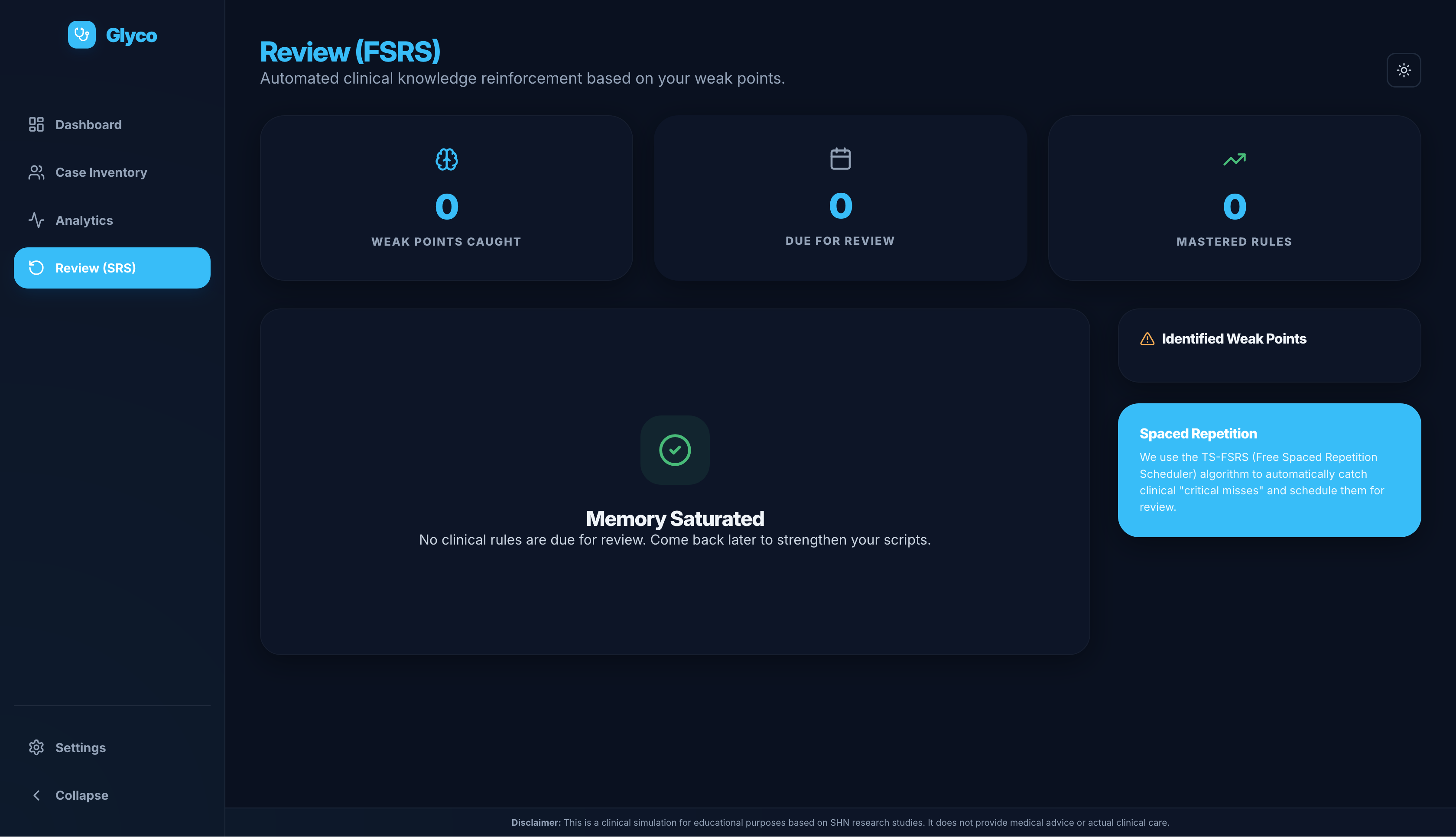
Review view
Glyco: LeetCode for Type 2 Diabetes Clinical Reasoning
Inspiration
Clinical guidelines for Type 2 Diabetes are comprehensive — but static. Medical students often learn by reading PDFs or answering recall-based quiz questions. However, real prescribing requires balancing competing priorities:
- Weight loss
- Hypoglycemia risk
- Cost and access
- Cardiovascular protection
- Kidney disease
- Patient adherence
We noticed a gap: there is no structured, repeatable environment where learners can practice committing to a full treatment plan and receive feedback on their reasoning.
Programming has LeetCode. Clinical reasoning doesn’t.
Glyco was built to change that.
What it does
Glyco is an interactive clinical reasoning simulator for Type 2 Diabetes management. Learners:
- Interview an AI-generated patient
- Review labs, vitals, and comorbidities
- Select clinical priorities (e.g., cardiorenal protection, hypoglycemia avoidance, cost)
- Build a full management plan
- Lifestyle
- Referrals
- Pharmacotherapy
- Lifestyle
- Write a short clinical rationale
- Receive rubric-based grading with:
- Critical misses
- Targeted feedback
Every encounter is grounded in verified excerpts from Diabetes Canada 2024 guidelines. The AI is constrained to these sources and cannot invent rules. Instead of memorizing answers, learners build a repeatable prescribing workflow.
How we built it
We designed Glyco around structured decision-making, not open-ended chat.
Frontend: structured case workflow
We built a modular interface with a guided sequence:
- Dialogue → Record → Evidence Vault → Management Plan
- Clinical priority selector
- Modular pharmacotherapy and lifestyle selection
- Short rationale submission
- Analytics dashboard with competency radar
AI architecture: evidence-first reasoning
We implemented an AI system that is intentionally not a generic chatbot wrapper:
- AI-generated patient cases constrained by dataset-derived rules
- Evidence Vault displaying guideline excerpts with page references
- Rubric-based grading engine that checks:
- Guideline adherence
- Omitted critical steps
- Clinical priority alignment
- Quality of rationale
- Guideline adherence
“Critical misses” are surfaced explicitly to support metacognitive reflection.
We intentionally avoided building a generic chatbot wrapper.
The AI operates within a structured workflow and verified rule set.
Challenges we ran into
1) Grounding AI in real guidelines
We had to ensure the system only used provided guideline excerpts and did not hallucinate medical rules. This required:
- Explicit rule constraints
- Evidence display as the default interface output
2) Designing fair grading
Grading clinical reasoning is complex. We created rubric categories and defined what constitutes a critical miss, including:
- Diagnosis completeness
- Drug choice appropriateness
- Lifestyle and referral steps
- Cardiorenal alignment
- Omission detection
3) Avoiding cognitive overload
Guidelines are dense. We structured the interface into tabs and chunks to reduce cognitive load while preserving realism.
4) Preventing “prompt gaming”
Instead of letting learners “argue” the AI into agreement, we required:
- Structured selections
- A short rationale submission
- Rubric checks that compare the plan against evidence-backed rules
Accomplishments we’re proud of
- Built a fully interactive clinical reasoning workflow
- Implemented explainable rubric-based grading
- Constrained AI to verified guideline excerpts
- Added competency analytics (radar + class distribution)
- Created scalable AI-generated cases with varying difficulty
- Designed around learning science principles:
- Retrieval practice
- Deliberate practice
- Metacognition
- Retrieval practice
Most importantly, we moved from static guidelines to interactive, graded decision training.
What we learned
- Clinical reasoning is a skill that requires deliberate practice
- AI alone is not enough — structure matters
- Grading reasoning requires transparency and explainability
- Constraining AI to evidence improves trust and educational value
- Students learn more when forced to commit to a full plan before seeing feedback
Educational AI tools must be designed around how people learn, not just around what AI can generate.
What’s next for Glyco
Broaden coverage: add more guideline-grounded cases
- ASCVD/HF
- CKD staging
- Insulin initiation
- Hypoglycemia
- Cost/adherence barriers
- ASCVD/HF
Adaptive practice: target cases to a learner’s weak areas using:
- “critical misses”
- competency scores
Stronger realism: expand curveballs
- missed follow-ups
- side effects
- refusal of injections
- insurance/affordability constraints
- missed follow-ups
Instructor tools:
- case builder
- rubric editor
- cohort analytics for teaching and assessment
- case builder
Built With
- anthropic
- css3
- html5
- next.js
- openrouter
- react
- typescript
- vercel

Log in or sign up for Devpost to join the conversation.