-
front page of DOODLE
-
more
-
drugs
-
final screen

Inspiration
Globally, there are approximately 1 million new curable STIs every single day. Here in the U.S., gonorrhea rates have jumped 45% and syphilis is up 52% since 2016. Through my clinical rotations and nursing coursework, I've seen firsthand how fragmented the system can be, relying heavily on a "one-size-fits-all" approach where every patient gets the exact same antibiotic regardless of their body composition, genetics, or social context. Compounding this clinical blind spot is the fact that social determinants of health create major barriers to follow-up and severe alert fatigue causes providers to override 46-96% of clinical decision support (CDS) alerts. We wanted to build a solution that addresses both the biological and systemic failures of modern STI treatment.
What it does
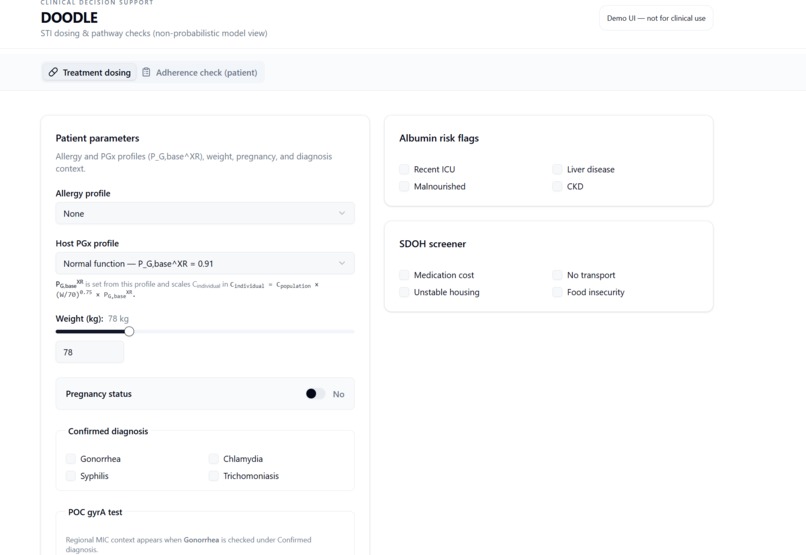
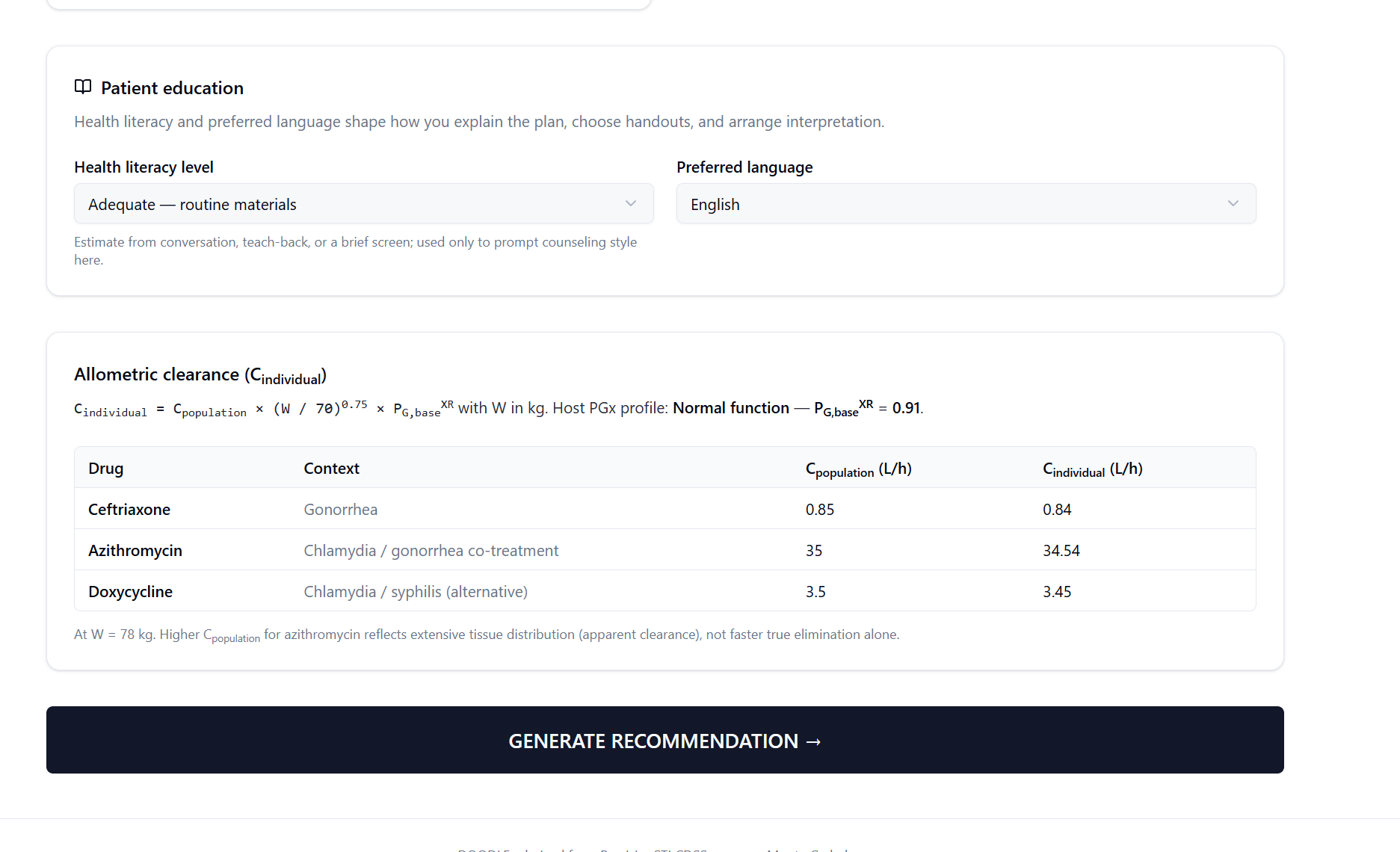
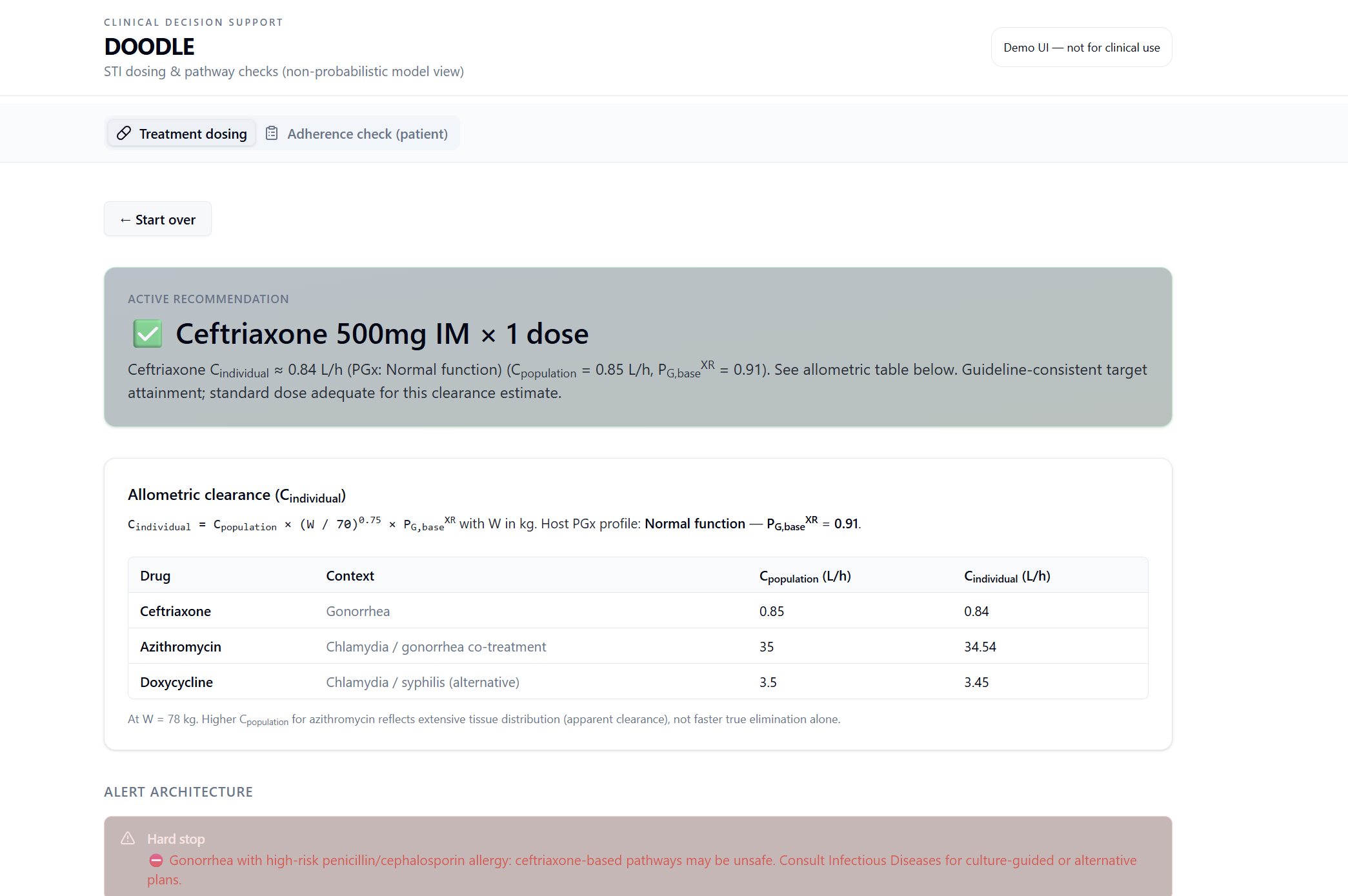
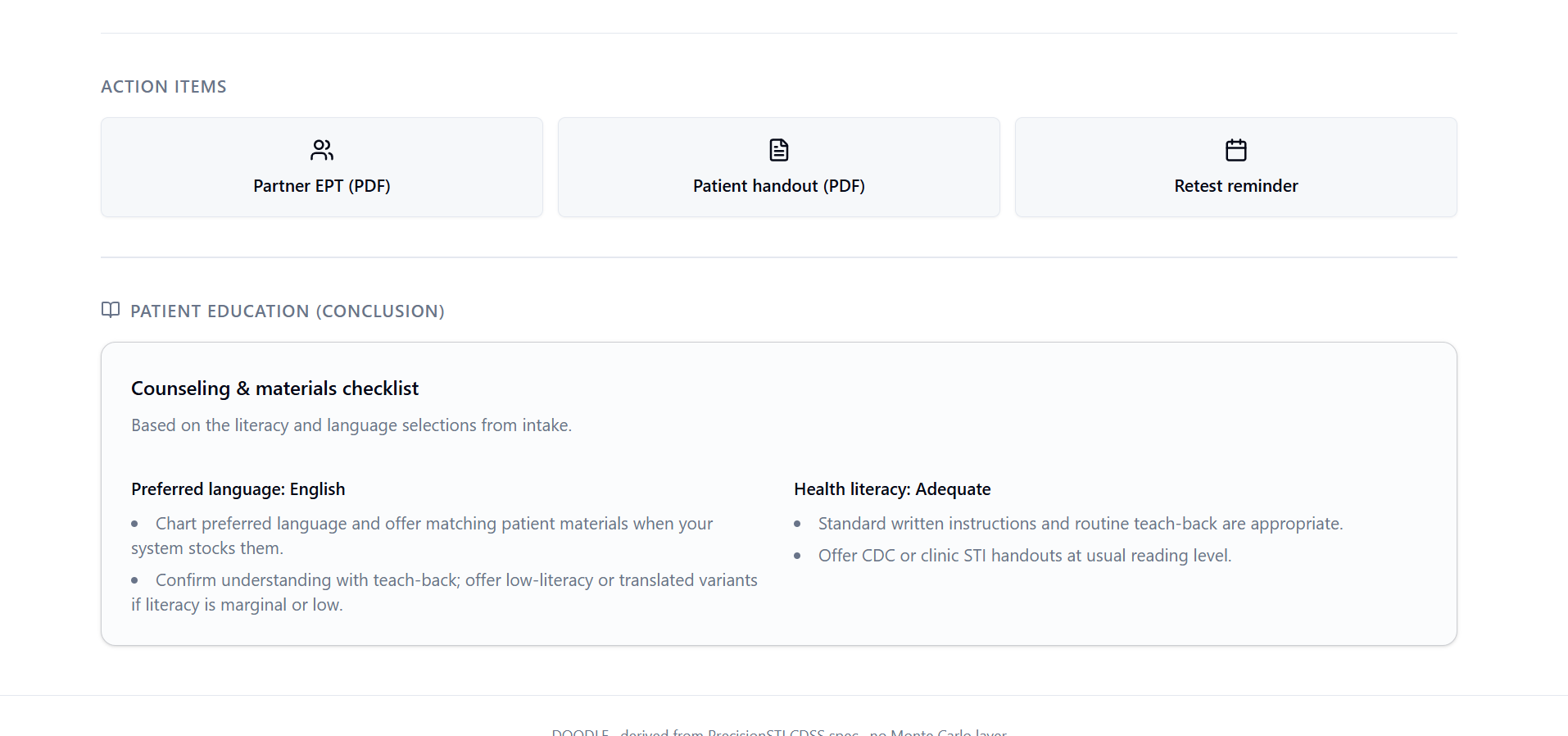
DOODLE (Dynamic Optimization Of Dosing & Local Epidemiology) is a same-day, dual-DNA clinical decision support tool designed for point-of-care use. Within 60 seconds, it processes 5 triage-speed inputs: weight, pregnancy status, allergy profile, host genotype, and albumin risk. It runs these inputs through a Population Pharmacokinetic (PopPK) dosing engine and a Monte Carlo simulation engine to calculate mathematically exact, guideline-concordant antibiotic recommendations. Beyond just picking the right drug and dose, DOODLE wraps the entire recommendation in an alert fatigue-proof architecture, generates literacy-calibrated patient education materials, and triggers an adherence risk feedback loop before the patient even leaves the clinic.
How we built it
We built the frontend clinical UI using React and Tailwind CSS for a clean, responsive experience. The backend decision engine, written in Python FastAPI/Node.js, executes our clinical rules alongside the PopPK math and the Monte Carlo engine. We pulled in free, open data sources, including the CDC GISP for regional antimicrobial resistance (AMR) profiles and PharmGKB/CPIC for drug-gene interactions.
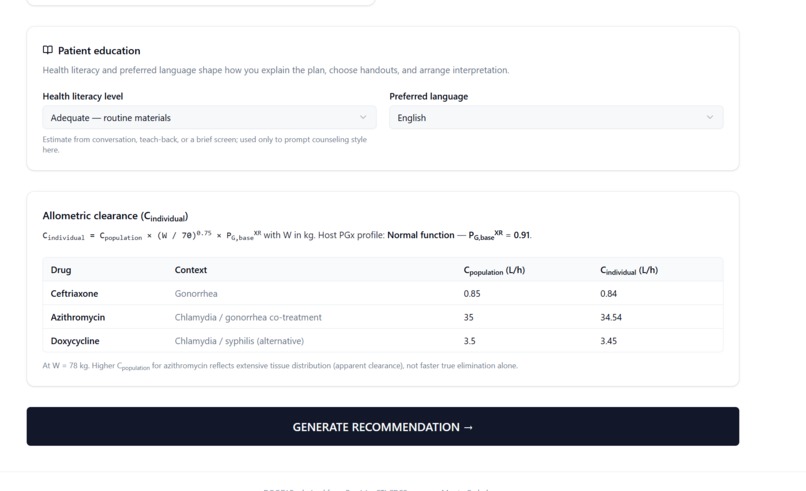
For the PopPK layer, we used allometric scaling to adjust drug clearance, using the universally accepted formula: $CL_individual = CL_pop \times (WT/70)^{0.75} \times PGx_factor \times Albumin_factor$. To power our treatment rankings, we built a Monte Carlo simulation engine that runs $N=10,000$ virtual patients to calculate the probability of target attainment (PTA) for different regimens.
Challenges we ran into
Our core design constraint was that a triage nurse had to collect all inputs in 60 seconds without drawing blood. However, the primary drug for gonorrhea, ceftriaxone, binds heavily (83-96%) to serum albumin, meaning changes in albumin drastically alter the drug's effectiveness. To solve this without a venipuncture, we created a surrogate risk-stratification checklist that flags patients likely to have clinically significant hypoalbuminemia based on their medical history.
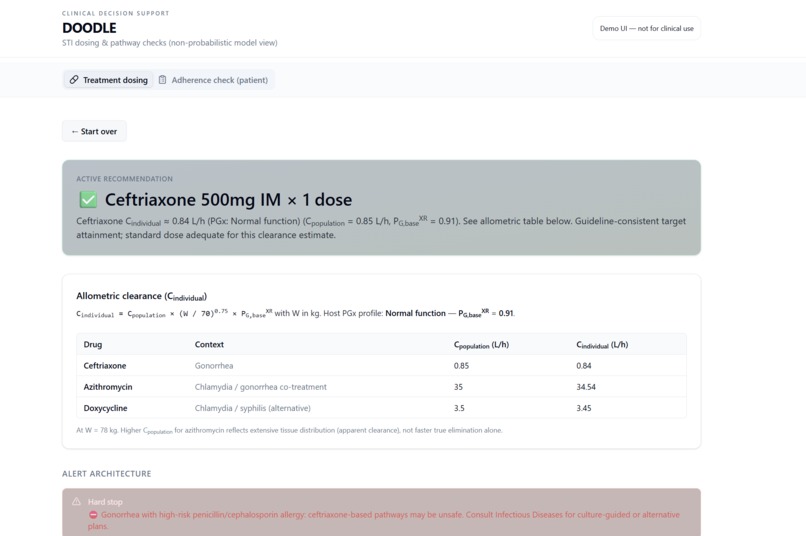
Another major challenge was alert fatigue. We had to carefully design a 3-tier alert system (Hard Stops, Soft Stops, and Passive alerts) to ensure clinicians wouldn't just blindly click past critical safety warnings, keeping the total alerts to fewer than 2 per encounter.
Accomplishments that we're proud of
We are incredibly proud of the "Dual-DNA" concept, which allows DOODLE to simultaneously analyze both the pathogen's resistance markers and the human's pharmacogenomics, like the ABCB1 genotype for azithromycin transport. We also successfully implemented the exact same 10,000-patient Monte Carlo probabilistic modeling framework used by major FDA-compliant dosing platforms into a functional hackathon MVP. Additionally, we successfully integrated a PRAPARE-based SDOH screening module that instantly translates patient barriers (like lack of transportation) into clinical actions (like preferring single-dose therapy).
What we learned
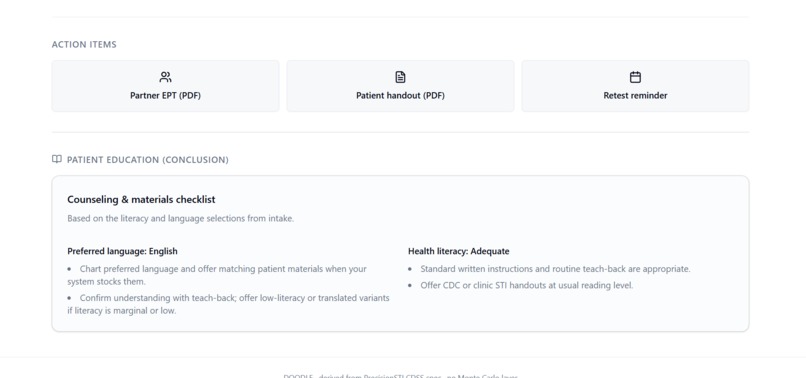
We learned a massive amount about pharmacokinetics, specifically that human drug metabolism doesn't scale linearly with weight, which is why the 0.75 allometric exponent is the gold standard. We also learned about the unintended consequences of guideline shifts; for instance, when the CDC shifted from single-dose azithromycin to a 7-day doxycycline course for chlamydia, it created a massive adherence gap that providers struggle to manage. Finally, diving deep into health literacy revealed that sexual health literacy is strongly tied to treatment adherence, underscoring the need for the visual pill calendars and teach-back prompts we built.
What's next for DOODLE
Our immediate next steps involve expanding DOODLE's logic beyond the initial modules to comprehensively cover all STIs. From a technical standpoint, the next major milestone is building out SMART on FHIR compatibility. This will allow DOODLE to be a true plug-and-play solution that seamlessly integrates directly into major EHR ecosystems like Epic and Cerner for widespread scalability.
Built With
- 211api
- arman
- cpic
- javascript
- pharmgkb
- python
- react
- smart-on-fhir
- tailwind

Log in or sign up for Devpost to join the conversation.