The Problem: Reasoning Gets Lost at 2 AM
Every year, critical clinical reasoning is lost during care transitions. A physician writes "will revisit CRP trend" in a progress note at 10 PM by 2 AM, when the patient transfers from ICU to step-down, that intent is gone. No one follows up. The data transfers. The reasoning doesn't.
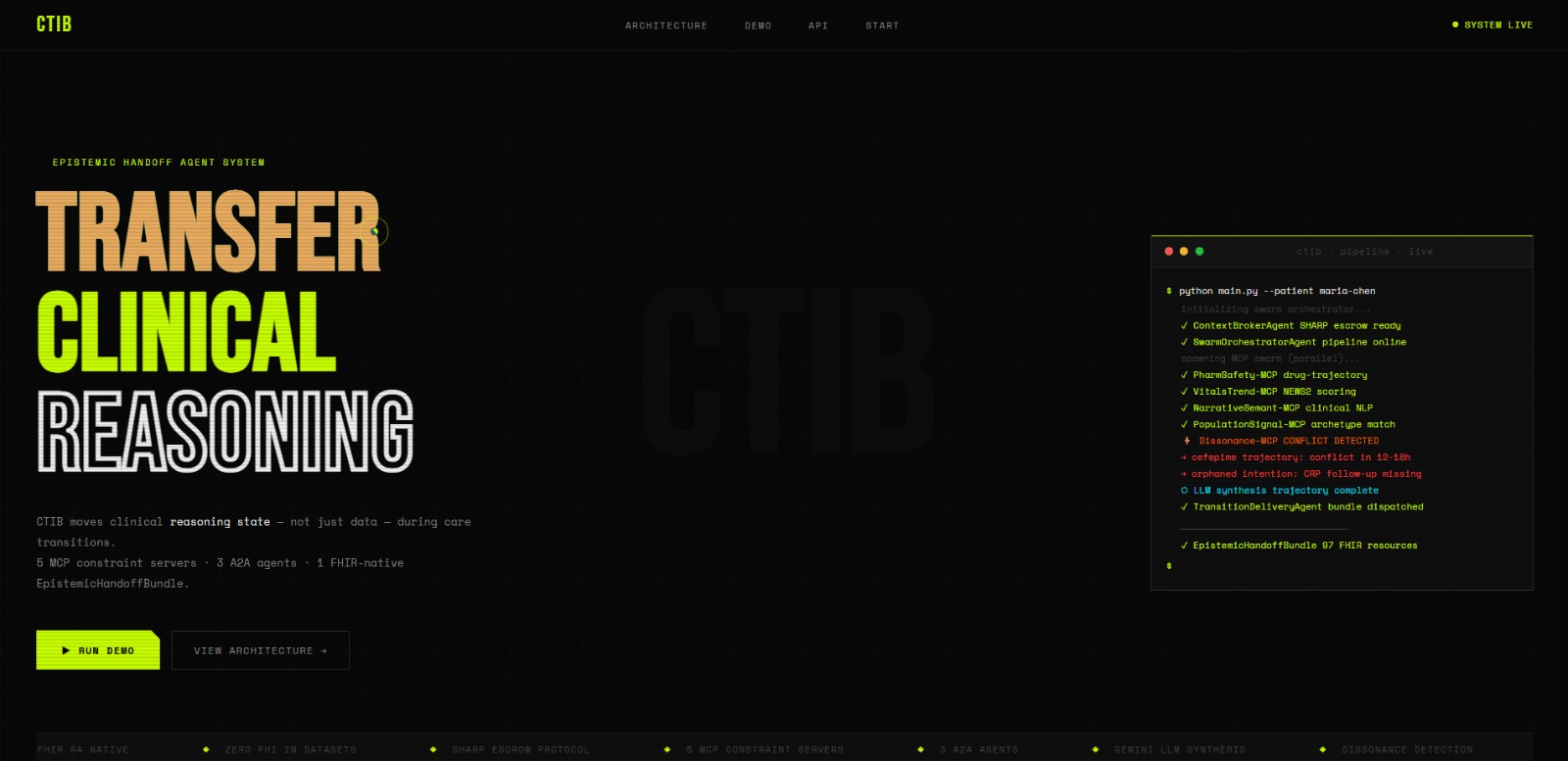
Traditional EHR handoff tools generate static PDF summaries. They move data, not understanding. CTIB solves this by transferring the epistemic state the clinical reasoning, unresolved intentions, and emerging conflicts as a machine-readable, auditable artifact.
What CTIB Does
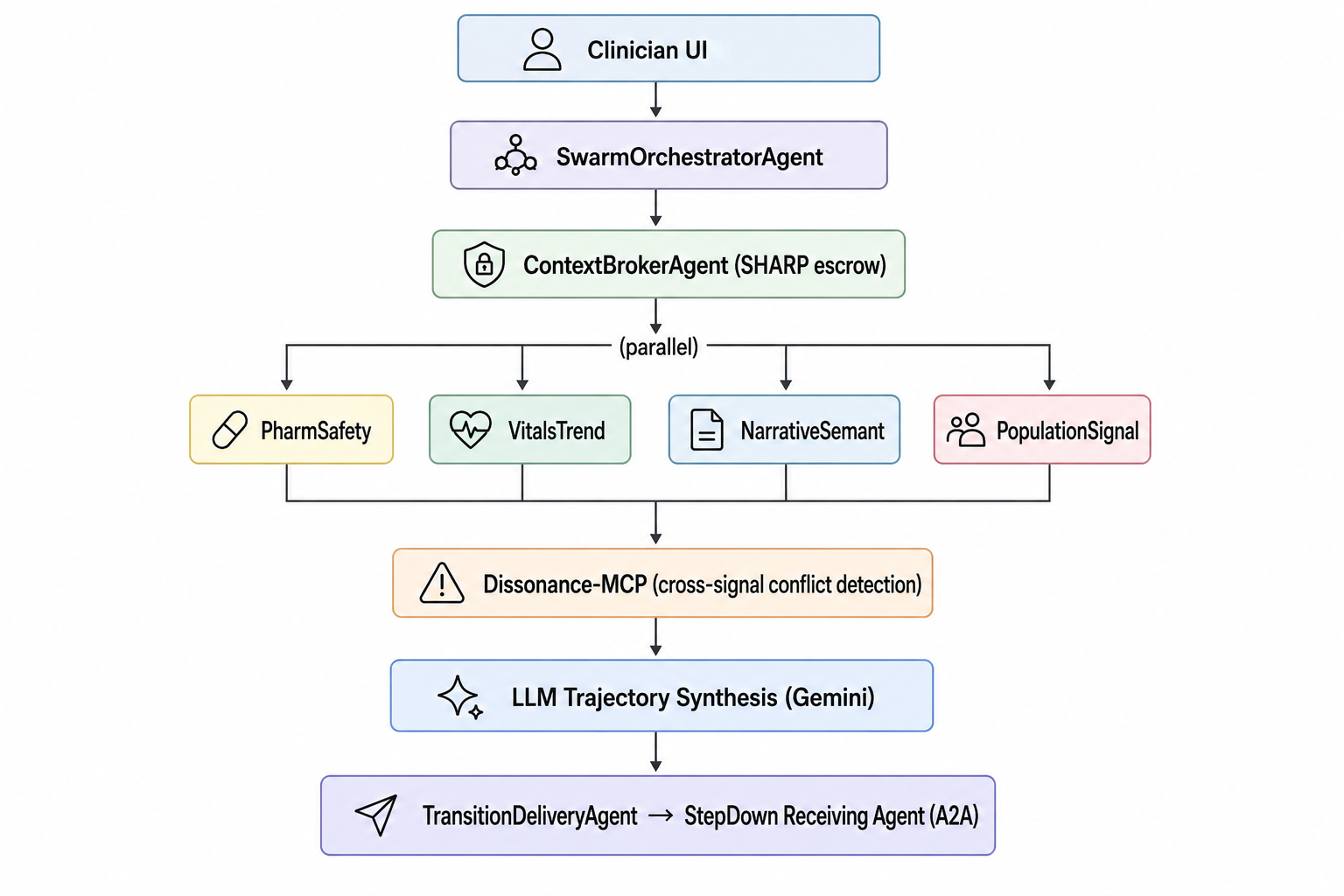
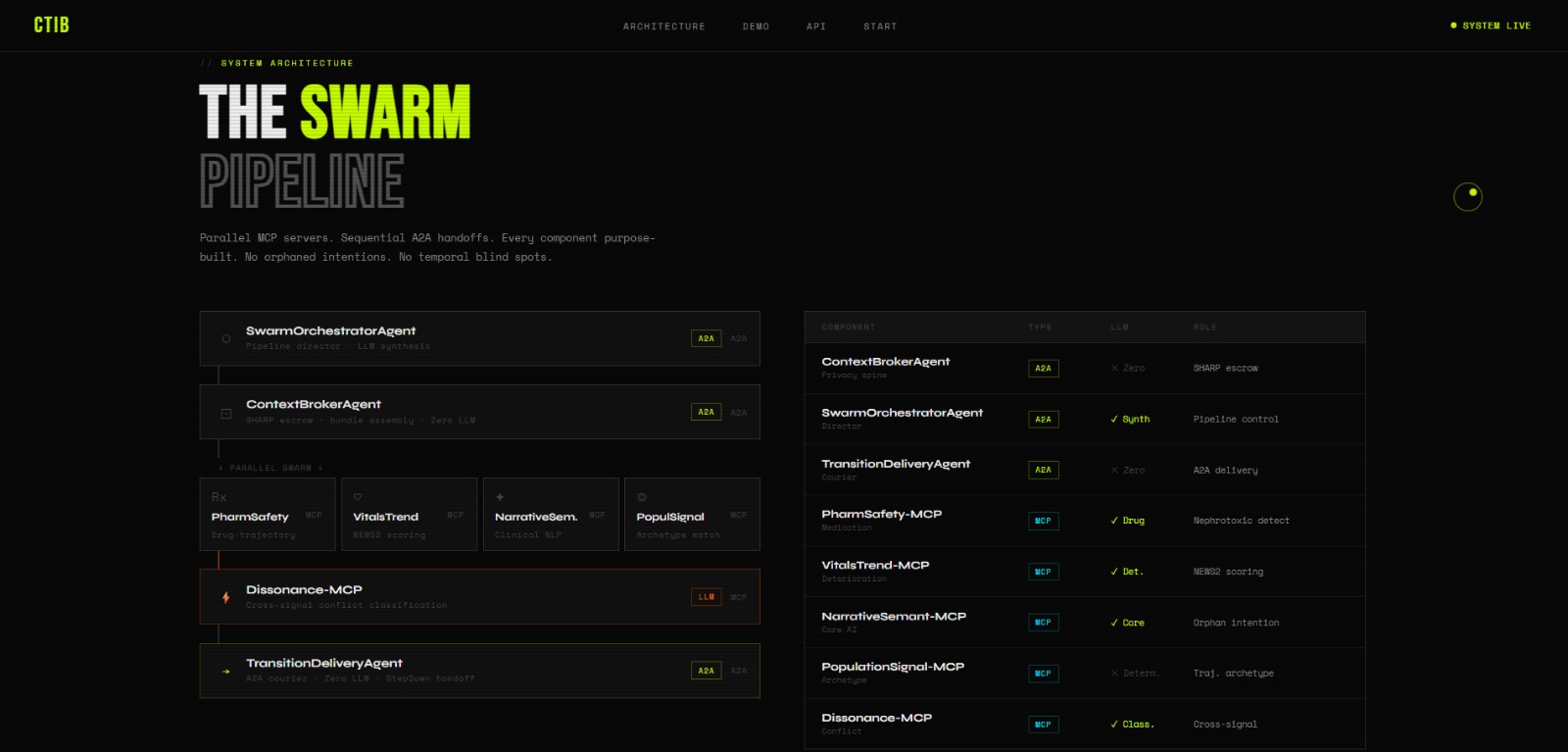
CTIB orchestrates a swarm of 5 MCP constraint servers and 3 A2A agents to synthesize structured FHIR R4 data + unstructured clinical notes into a FHIR-native EpistemicHandoffBundle.
The Golden Path Pipeline (runs in ~2 seconds):
- SHARP Context - Cryptographically scoped consent token minted for the session
- FHIR Fetch - 97 resources pulled in parallel (vitals, labs, meds, notes)
- MCP Swarm - 5 specialized servers analyze in parallel:
- PharmSafety-MCP: Medication reconciliation + nephrotoxic trajectory detection
- VitalsTrend-MCP: NEWS2 scoring + subtle deterioration patterns
- NarrativeSemant-MCP: Clinical NLP + orphaned intention detection
- PopulationSignal-MCP: Trajectory archetype matching
- Dissonance-MCP: Cross-signal adversarial conflict detection
- LLM Synthesis - Gemini synthesizes a trajectory narrative from all signals
- Bundle Assembly - EpistemicHandoffBundle with 4 mandatory sections
- A2A Delivery - Bundle delivered to receiving agent via A2A protocol
Three Critical Findings (Demo Maria Chen):
🔴 Temporal Dissonance Cefepime dose is correct for current creatinine (0.95 mg/dL), but PharmSafety and VitalsTrend independently detect that the renal trajectory will make this dose nephrotoxic within 18 hours. The conflict is caught BEFORE it causes harm.
🟡 Orphaned Intention Day 3 progress note says "Will revisit if CRP continues to trend." CRP was never drawn on Day 4 or Day 6. A clinical intent was silently lost.
🟢 Watch Subscriptions FHIR Subscriptions automatically generated so the step-down team is alerted when creatinine crosses the threshold.
Technical Stack
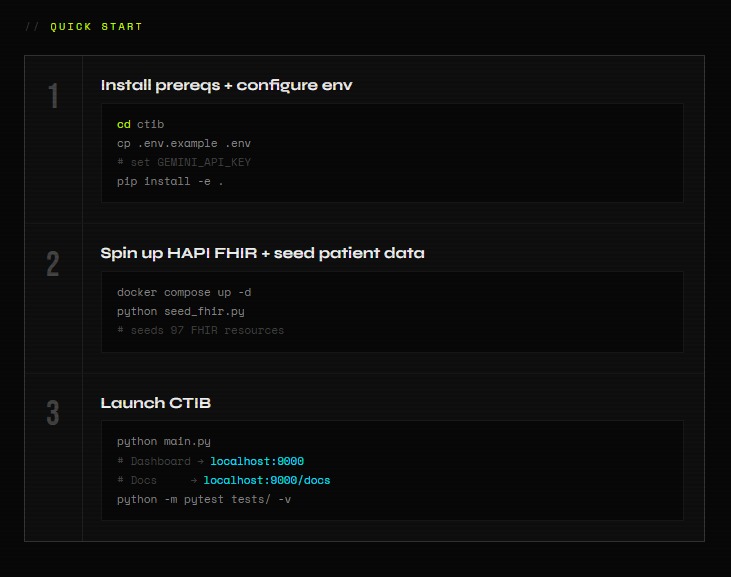
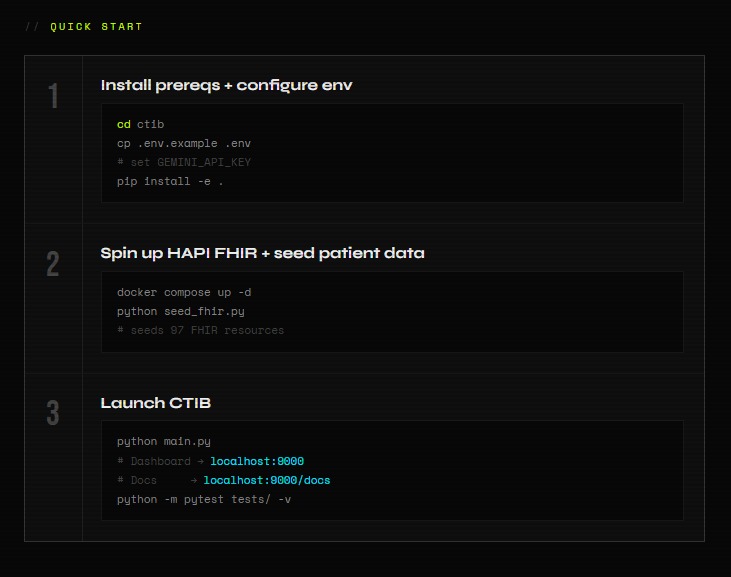
- Runtime: Python 3.11 / FastAPI / Uvicorn
- LLM: Google Gemini 2.0 Flash (via google-genai SDK)
- Protocols: MCP SDK, A2A Protocol (v1.0), SHARP Extension Specs, FHIR R4
- Data: 100% synthetic - zero PHI
- Deployment: Render.com (free tier)
- Marketplace: Published on Prompt Opinion Marketplace
Why This Is Not a Wrapper
CTIB is NOT a "ChatGPT wrapper with a FHIR API." Here's why:
- 5 independent MCP constraint servers each contribute domain-specific analysis
- Adversarial validation - Dissonance-MCP cross-checks all signals against each other
- Zero-LLM agents - ContextBrokerAgent and TransitionDeliveryAgent are fully deterministic (no AI hallucination risk in the privacy and delivery layers)
- SHARP compliance - Every signal exchange is scoped by a cryptographic consent token
- FHIR-native output - The EpistemicHandoffBundle is a valid FHIR Composition, not a text blob
Judging Criteria
The AI Factor
CTIB uses Gemini 2.0 Flash for two tasks that rule-based systems cannot perform: (1) Extracting orphaned clinical intentions from unstructured progress notes NarrativeSemant-MCP identifies that "will revisit CRP trend" was written but never acted on, something impossible with keyword matching alone. (2) Cross-signal conflict classification Dissonance-MCP uses LLM to detect that a medication safety signal and a vital trend signal, each individually unremarkable, create a critical temporal conflict when analyzed together.
Potential Impact
Care transitions account for up to 80% of serious medical errors (Joint Commission). CTIB addresses the root cause: lost reasoning. The EpistemicHandoffBundle ensures three things survive every transfer: (1) Drug-trajectory conflicts detected proactively, (2) Clinical intentions that would otherwise be silently lost, and (3) Automated monitoring protocols so the receiving team knows exactly what to watch. This isn't another PDF it's a machine-readable artifact that enables downstream automation.
Feasibility
CTIB is deployed and running today at ctib.onrender.com. It uses 100% synthetic data (zero PHI), SHARP consent scoping for every data exchange, and zero-LLM agents for privacy-critical layers (ContextBrokerAgent and TransitionDeliveryAgent are fully deterministic no hallucination risk). The FHIR R4 native output integrates with any standards-compliant EHR. Published on Prompt Opinion Marketplace and invokable today.


Log in or sign up for Devpost to join the conversation.