-
-
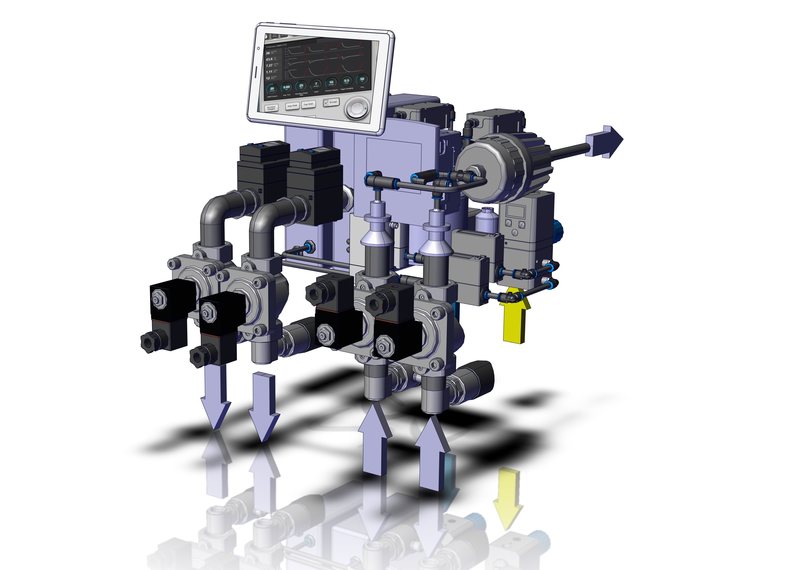
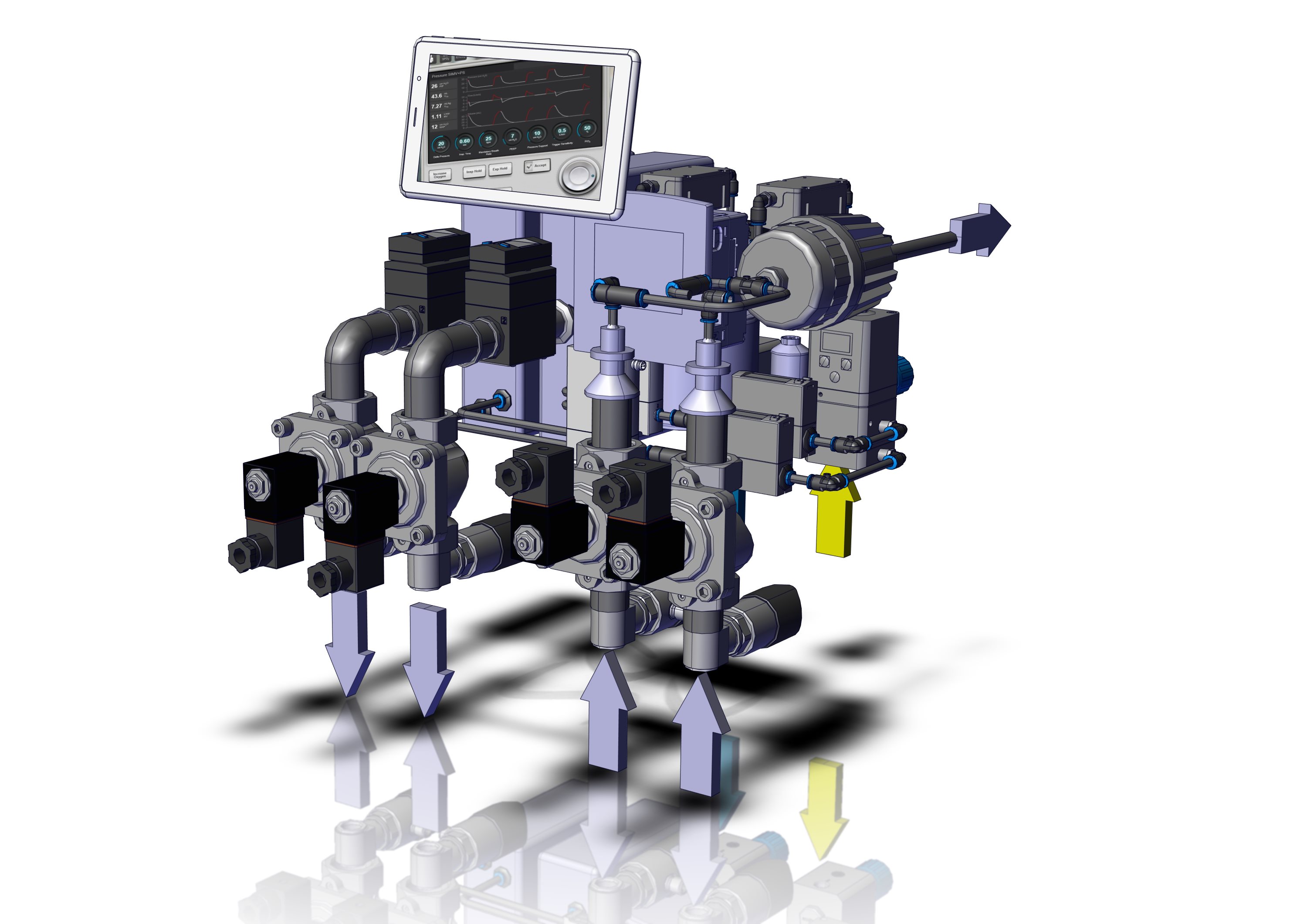
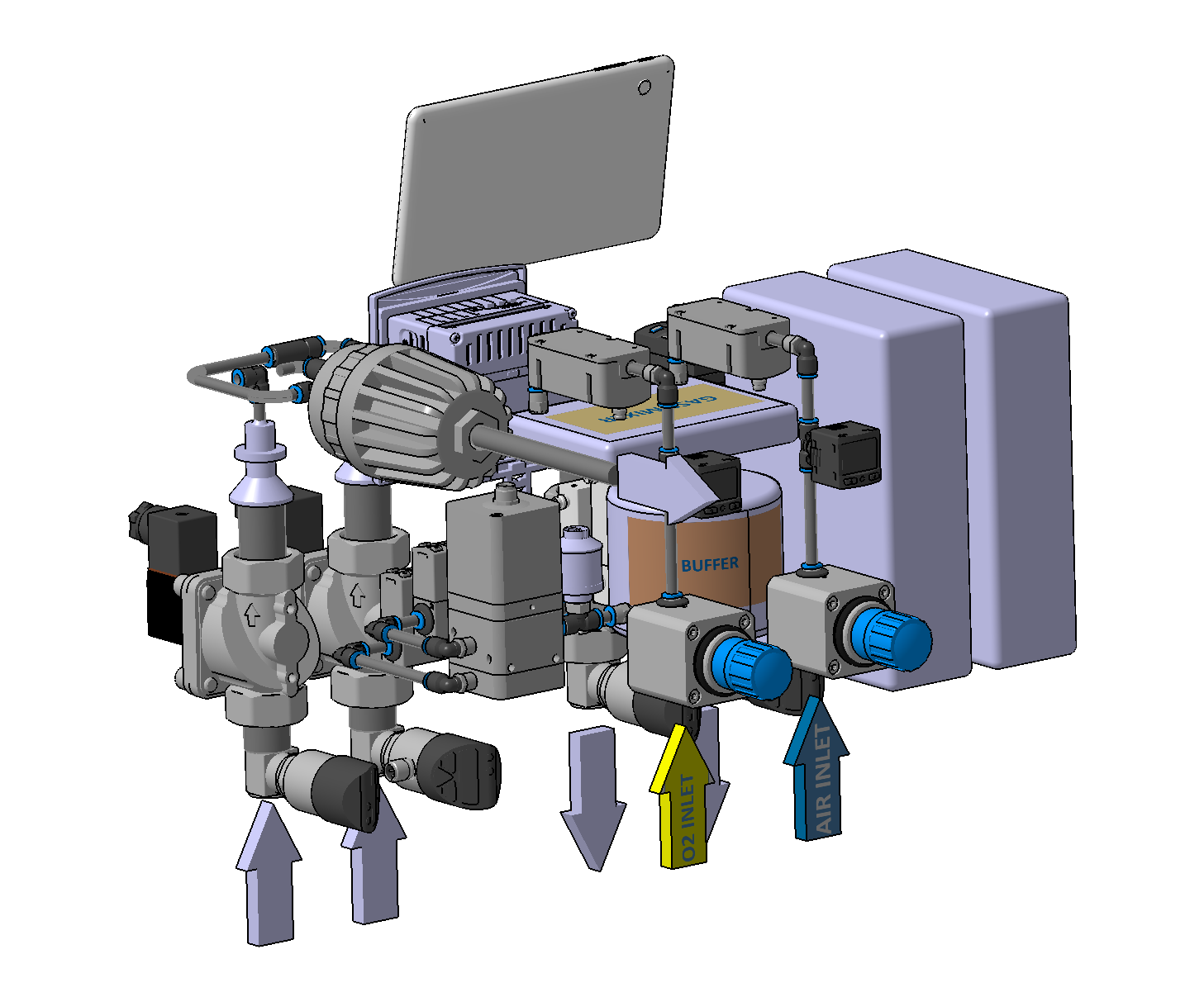
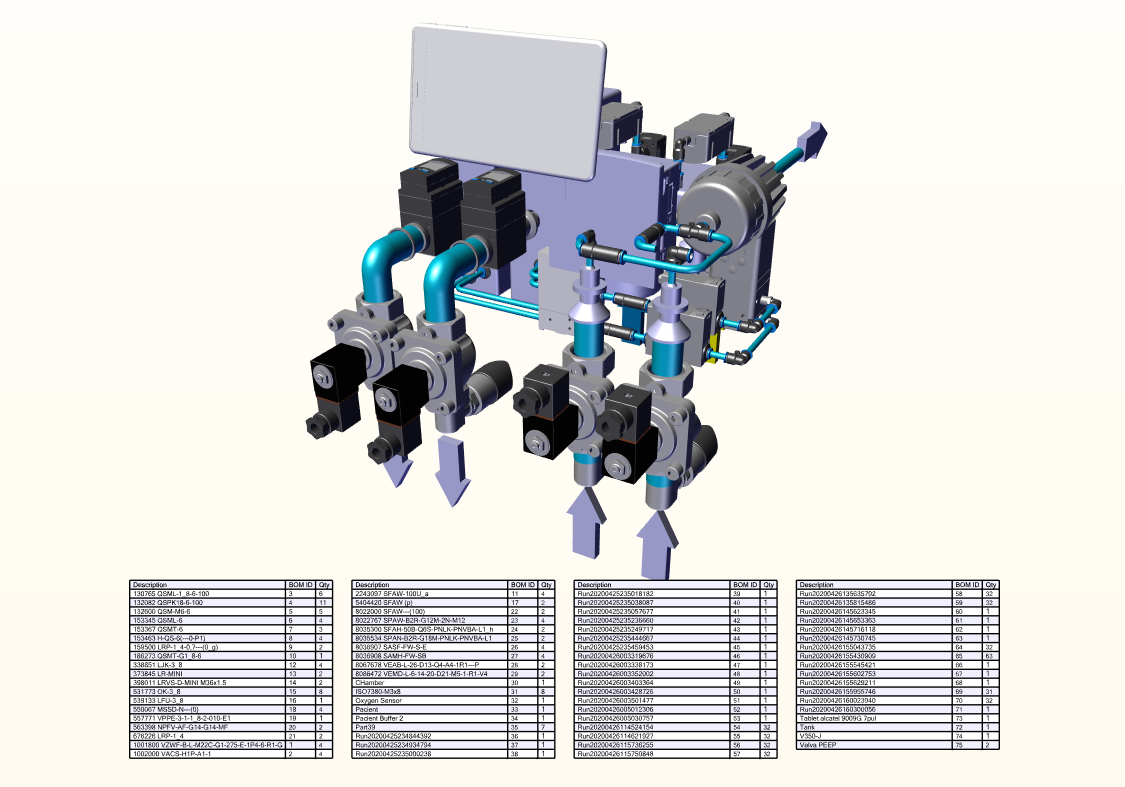
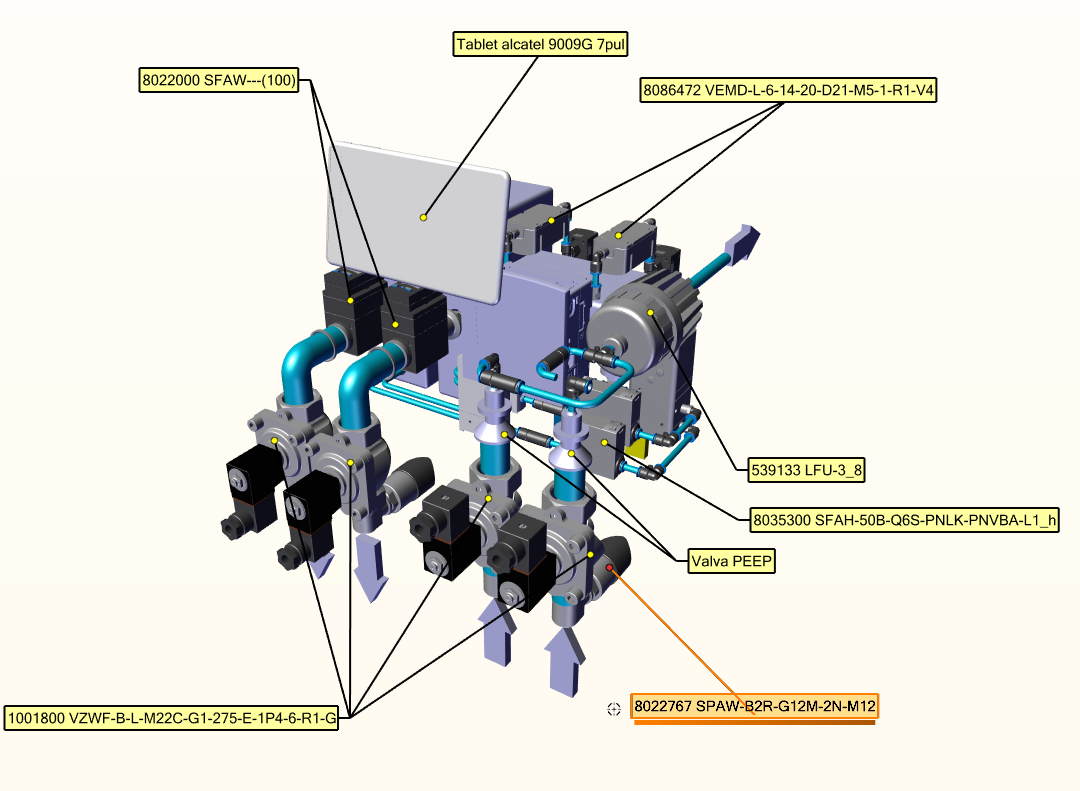
Isometric view
-
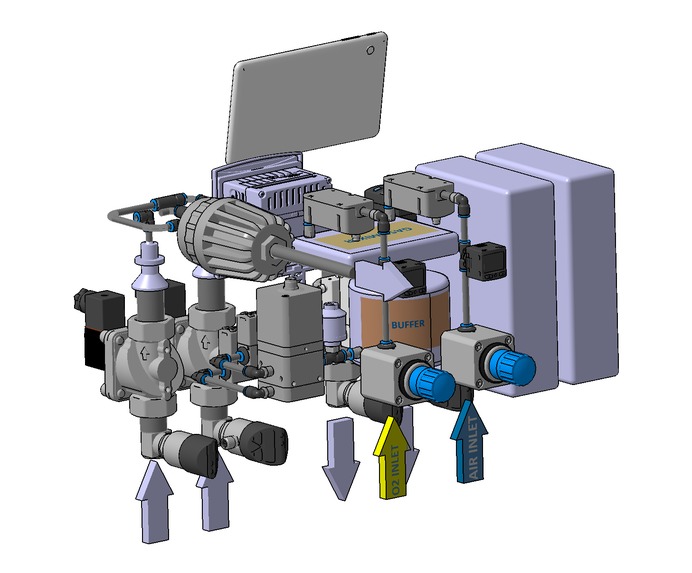
Isometric view
-
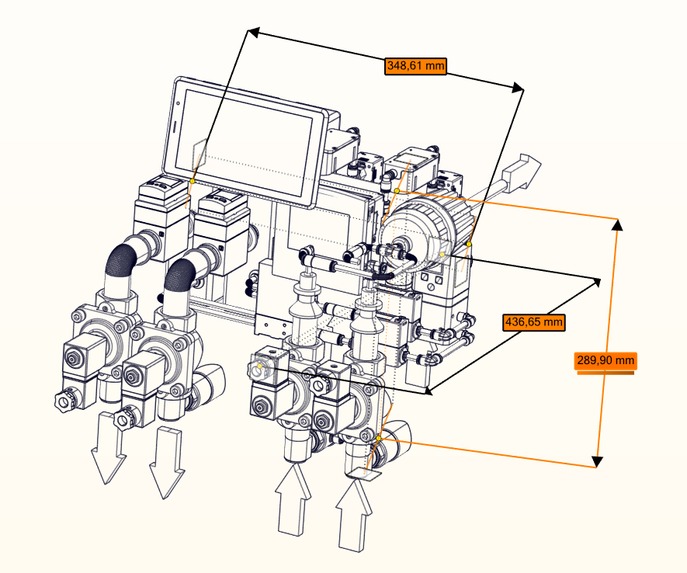
Dimensions
-
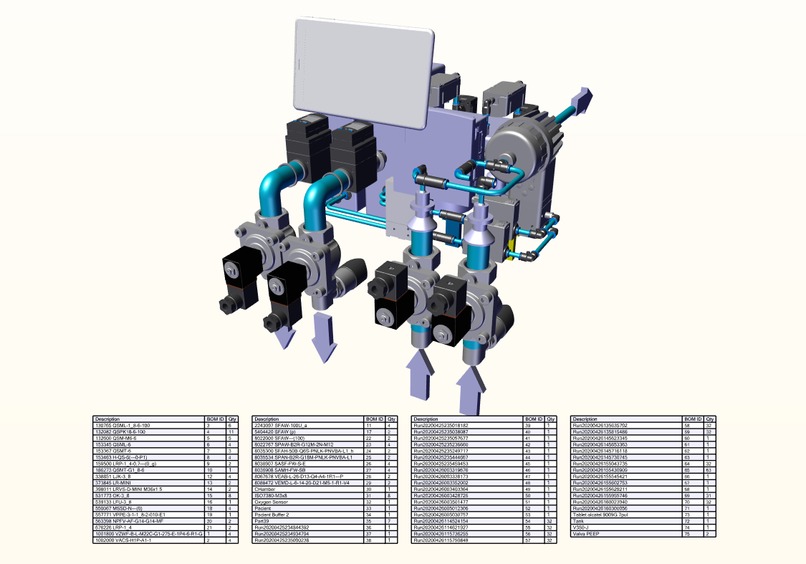
Bill of Material with part number
-
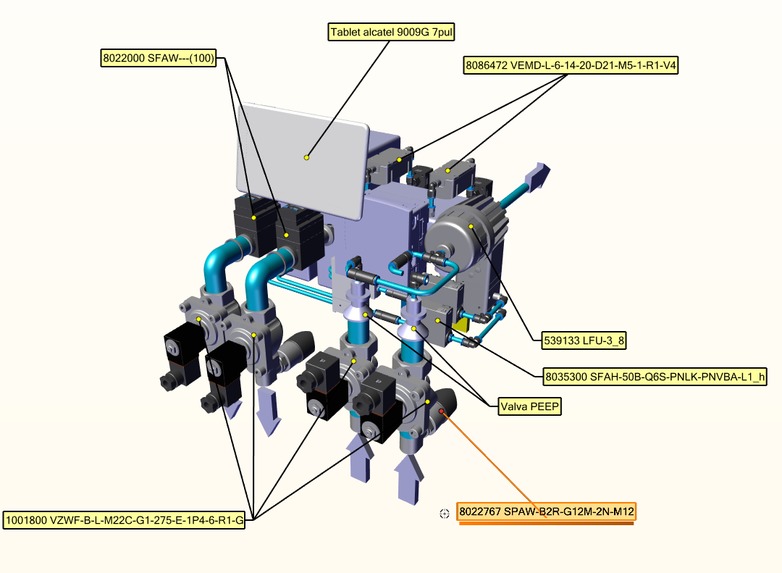
Components
-
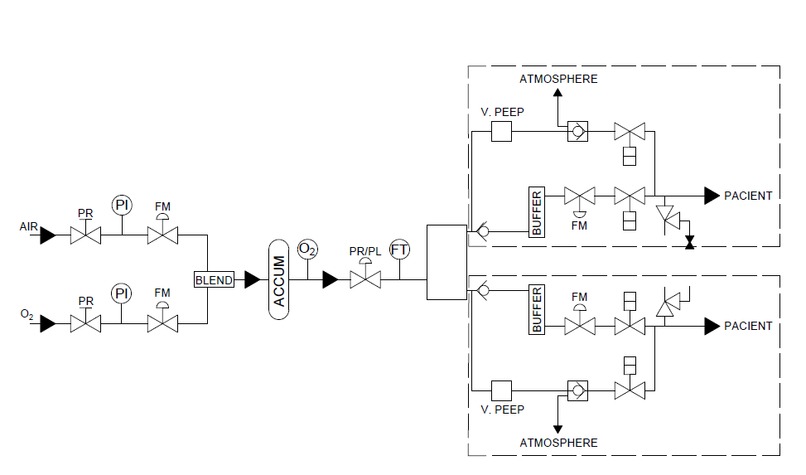
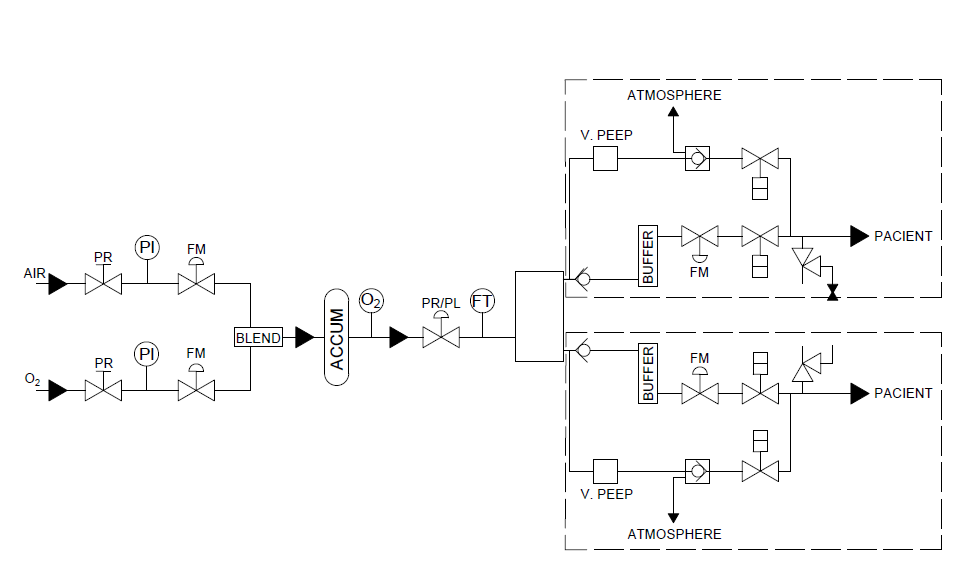
Pneumatic schema

The context
A GlobalData analysis (https://www.nsmedicaldevices.com/analysis/coronavirus-ventilators-global-demand/) shows there is a shortage of 880,000 ventilators worldwide, with France, Germany, Italy, Spain and the UK needing urgently about 74,000 units to supplement their existing ICU capacity. For example, the NHS is looking for 20,000 to 30,000 ventilators to buy, Germany has put a domestic order for 16,000 products and Italy has only one manufacturer making 500 pieces a month (https://www.voanews.com/science-health/coronavirus-outbreak/european-governments-scramble-ventilators-urge-shoppers-stop).
The difference between demand and supply is very large and many other companies are trying to step up, either voluntarily or being ordered by their governments. The process is still complex and slow, especially compared to the exponential spread of the virus.
The most important companies active on this market are (https://www.marketsandmarkets.com/Market-Reports/ventilators-market-11018337.html?gclid=CjwKCAjw4pT1BRBUEiwAm5QuRyz6aPYoE8qHyMRfdgK4arFRSu5js0VEJAwSchfPtD_vOmxGVCrIChoCKrwQAvD_BwE): Philips Healthcare (Netherlands), ResMed (US), Medtronic (Ireland), Becton, Dickinson and Company (US), Getinge (Sweden), Dräger (Germany), Smiths Group (UK), Hamilton Medical (Switzerland), GE Healthcare (US), Fisher & Paykel (New Zealand), Air Liquide (France), Zoll Medical (US), Allied Healthcare Products (US), Airon Mindray (China), and Schiller (Switzerland).
About us
The TUCNONE team consists of teachers from the Department of Design Engineering and Robotics at the Technical University of Cluj-Napoca. We are participating for the first time in a Hackathon, in the current formula, and we are proposing a new idea in terms of mechanical ventilators: an integral pneumatic device that can provide different recipes for Air / O2 / volume / pressure to at least two patients. In some hospitals during the pandemic a series of adapters were used that allowed ventilation of two patients from the same device but with the same prescription of Air / O2 / volume / pressure.
The problem and project aim
The need for ventilators at the moment is large and urgent, with most countries looking for solutions, internally or externally. Monitoring so far (https://www.worldometers.info/coronavirus/) shows that cca. 20% of closed cases resulted in the death of the patient, and another 3% of active cases are in serious or critical condition, with many of these requiring mechanical ventilation.
This project aims to develop a pneumatic ventilator capable of providing at least two different air+O2 mixtures to two different patients. The ventilator uses only pneumatic components for dosing and creating the gas mix.
The solution
The equipment we propose is supplied from the compressed air and oxygen wall sockets at a pressure between 1.2 and 2.5 bar. On each supply line (air and oxygen) there is a pressure regulator that regulates the pressure to a fixed value between 1.2 and 2.5 bar, a pressure indicator and a flow meter. With the help of the flow meter the volume of air and oxygen that enters the mixing chamber is controlled, thus allowing Fractional O2 control (FIO2) between 21% to 100%. Here the two gases mix due to a serpentine path that creates vortices. From the mixing chamber, the air-oxygen mixture reaches a buffer in which the mixture is stabilized for dosing the patient.
From the buffer the mixture is picked up by a three-way proportional valve that sends to each patient on different circuits the mixture through a flow meter that controls Tidal Volume (TV) between 250 and 650 ml, a pressure regulator that regulates Peak Inspiratory Pressure (PIP) between 10 and 40 cm h2o and a buffer tank. Thus, in each tank there may be different pressures and volumes of fluid. Because there is a low pressure in the buffer tank, all connections were made further with a 22mm diameter inner pipe similar to the kit with which the patient is connected to the device. From the buffer tank the air is sent to the patient with the help of a flow meter that measures exactly the volume of gas and an electrically operated on-off valve that closes or opens the flow towards the patient.
On the expiratory route there is a pressure sensor that detects if the patient is trying to expire, an expiratory solenoid valve (EVE), a PEEP valve, a directional control valve on each of the two routes and a filter.
The system we propose is fully pneumatic, the frequency at which it can work is 20 milliseconds, so the respiratory rate control (RR) to be between 10-30 bpm is not a problem. The system is completely automatic, the adjustment of the Inspiratory / Expiratory ratio (I / E) between 1:1 and 1:4 is done using a PLC.
The humidity control is done with an external unit controlled by PLC, the equipment has a 10-inch tablet for entering data and monitoring the operating cycles. The PLC has a network connection and can be accessed from the intranet, if this device permission is granted, and the evolution of the parameters can be followed in a centralized manner. For security reasons the modification of the parameters can be done only from the tablet of the equipment and not remotely.
The equipment can operate in CMV – Continuous Mandatory Ventilation mode.
The equipment can operate in PRVC / Pressure Controlled mode – a set pressure is delivered for the inspiration period and the volume achieved is measured and displayed, the pressure and flow are controlled both before the buffer tank, dedicated to each patient, and before the delivery of the gas mix to the patient.
The equipment can also operate in Volume Control Ventilation mode – the user sets a tidal volume and respiratory rate. The tidal volume and respiratory rate can be adjusted separately for each patient.
A series of alarms can be set and activated:
- Gas supply failure – we have two sensors, one for oxygen and one for compressed air;
- Machine switched off while in mandatory ventilation mode from PLC;
- Inspiratory airway pressure exceeded;
- Inspiratory and PEEP pressure not achieved (equivalent to disconnection alarm);
- Tidal volume not achieved or exceeded.
What is innovative about our ventilator?
The equipment provides mechanical ventilation to two patients, but it's capable of differentiating between their necessities, respecting their O2 prescription, thus, it can replace two conventional ventilators. It makes use of two pressures: one higher for creating the air-O2 mixture and one lower for providing the resulted mixture to the patients. A limitation of our equipment is that it's larger and heavier than the professional ones because stainless steel components are used in the construction of valves and regulators, but it has a low price (approximately 3,000 euros) and it's built entirely using standardized components from various pneumatic parts manufacturers.
The scalability and next steps
The project is scalable and can be mass-produced, we intend to manufacture in the next two weeks 15 pieces, which we will donate to various hospitals in Romania. The components we use are from Festo and Emerson ASCO, manufacturers of micro valves and industrial regulators, and they can supply the necessary parts for building such a device. The oxygen sensor is the only component that is manufactured exclusively for the medical industry.
What have we done already?
During the hackathon weekend, the team has focused on bringing the project up to a Technology Readiness Level (TRL) of 3 meaning "experimental proof of concept". For this goal, we have refined and detailed the conceptual design (mechanical structure, piping connections, automation controls) and started the assembly of the minimum viable product (MVP) using the commercially available components described. The result can be seen in the above video and figures and it fully validates the design process, being ready to be expanded immediately into a complete laboratory prototype.
Built With
- catia-v5
- fluiddraw-p6
- lvsim-ems










Log in or sign up for Devpost to join the conversation.