-
recommendation
-
Prediction
-

website

💡 Inspiration
Alzheimer’s disease is one of the most complex challenges in modern medicine, characterized by slow onset and subtle early symptoms. While researching machine learning applications in healthcare, I realized something critical: building a high-accuracy model is only half the battle.
In clinical settings, "black box" AI models are dangerous. If a model predicts a high risk of Alzheimer's but can't explain why, a doctor cannot trust it. Furthermore, models "drift" over time—a model trained today might fail silently tomorrow due to changing patient demographics or data quality issues.
This inspired me to build Cogaly: not just a prediction engine, but a safety-first observability system. My goal was to answer the question: "If this AI begins to fail or behave unsafely, will we know before it harms a patient?"
⚙️ How We Built It
We approached Cogaly as a production-grade engineered system, not just a data science notebook.
1. The Core Engine (XGBoost + SHAP)
We used XGBoost for the core classification task because of its superior performance on tabular clinical data. To mitigate the "black box" problem, we integrated SHAP (SHapley Additive exPlanations) directly into the inference pipeline.
Each prediction $f(x)$ is decomposed into the sum of feature contributions $\phi_i$, giving clinicians an exact reasoning for every risk score:
$$ f(x) = \phi_0 + \sum_{i=1}^M \phi_i $$
Where $\phi_i$ represents the marginal contribution of feature $i$ (e.g., MMSE score or Hippocampal volume) to the final risk probability.
2. The Observability Layer (Datadog)
This is the heart of Cogaly. Instead of just logging "200 OK", we emit custom metrics for every prediction:
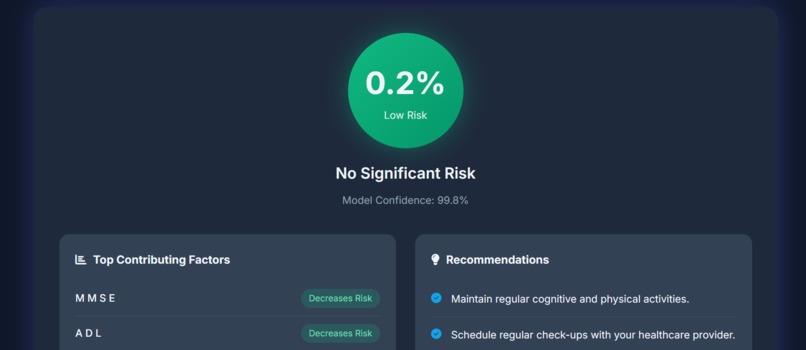
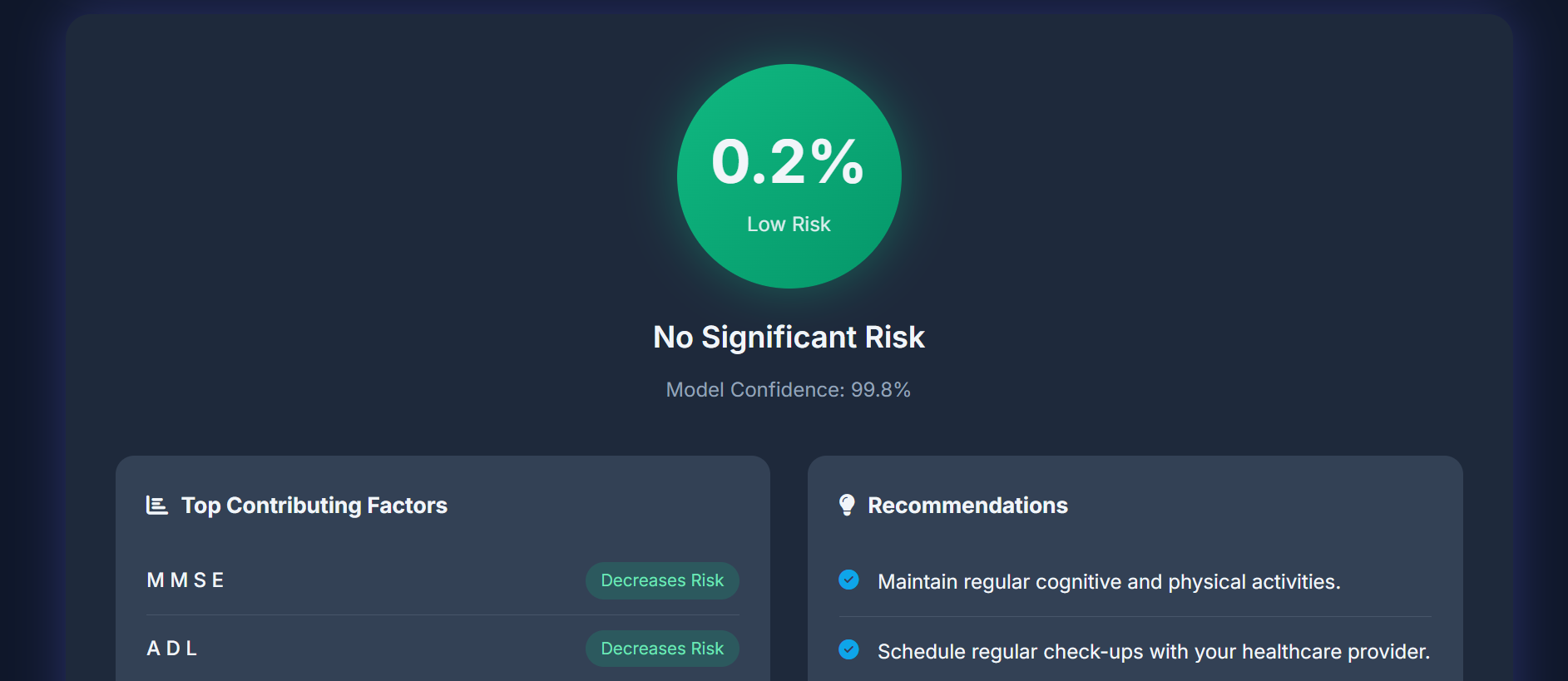
- Confidence Scores: Tracking the model's certainty ($P(y|x)$).
- Data Drift: Monitoring distributions of key inputs like Age and MMSE.
- Latency: Ensuring real-time responsiveness.
We configured Datadog monitors to alert us on specific "Medical Safety" violations—for example, if the model confidently predicts "Low Risk" for a patient with severe cognitive decline indicators.
3. Application & Deployment
- Backend: Python FastAPI for high-performance inference.
- Frontend: A responsive, accessible web UI to democratize access.
- Deployment: Hosted on Render, auto-deploying from GitHub to ensure continuous delivery.
🚧 Challenges We Faced
The journey wasn't smooth. Our biggest hurdle was the "Works on My Machine" adaptation of the deployment:
- Serialization Hell: We faced cryptic
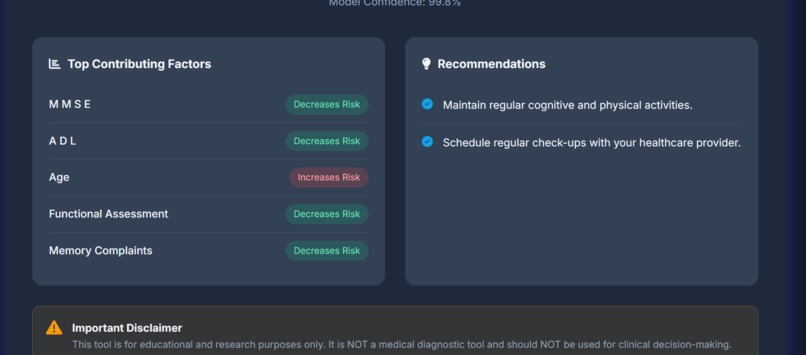
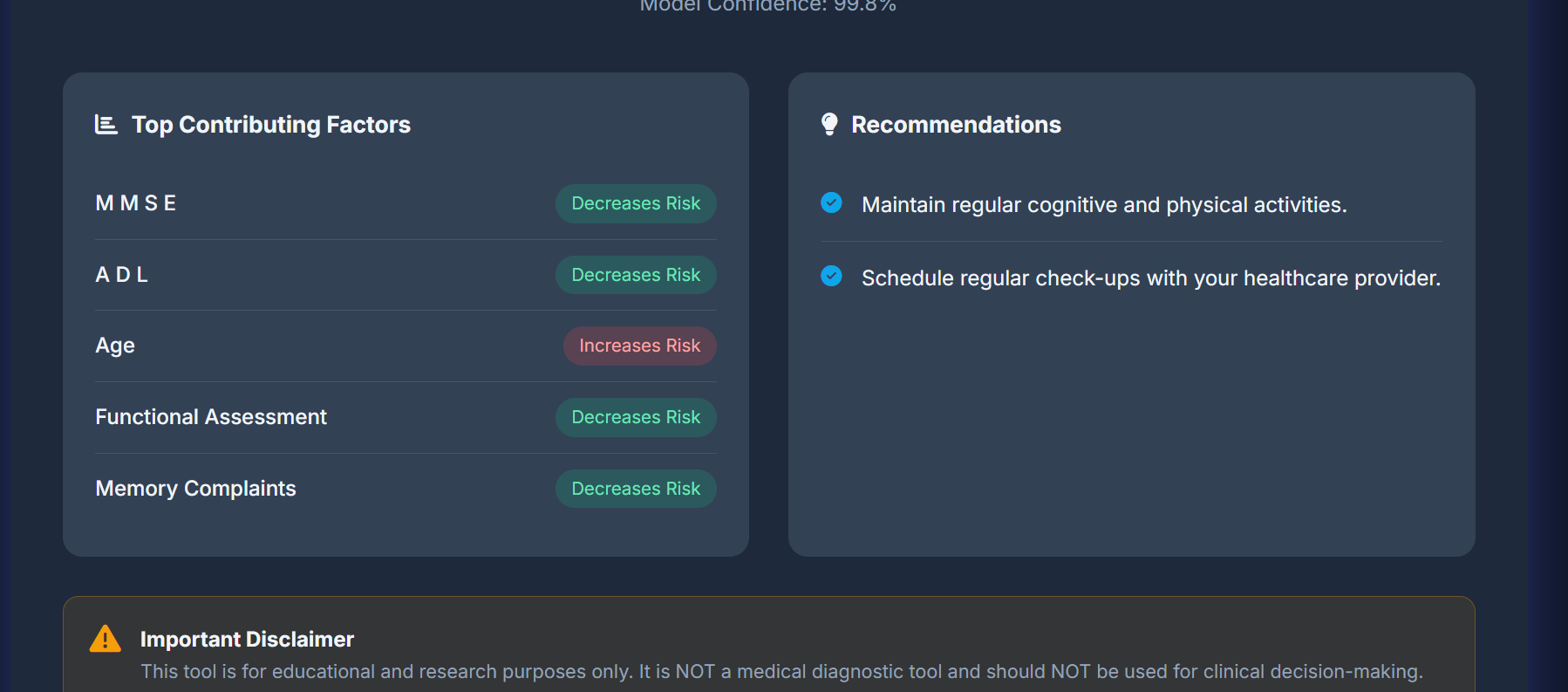
pickleserialization errors when deploying to Azure due to a Python version mismatch (3.11 vs 3.10). The model trained locally refused to load in the cloud. We solved this by standardizing our runtime environment and migrating to Render for more granular control over the build process. - Explainability vs. Noise: Initially, SHAP returned contributions for all 30+ features, overwhelming the user. We had to implement a filtering logic to present only the top 5 statistically significant factors, translating raw math into clinical insights.
🧠 What We Learned
- Observability is not optional: In healthcare AI, observability is safety. Measuring model confidence is just as important as measuring accuracy.
- Infrastructure matters: A great model trapped in a broken container is useless. Mastering the deployment pipeline (Docker, CI/CD, Environment Variables) was a huge learning curve but essential for delivering a real product.
- Empathy in UX: Designing the result screen required empathy—telling someone they are at "High Risk" requires careful framing, clear data, and actionable next steps, not just a raw red banner.
🚀 What's Next for Cogaly
We plan to expand Cogaly by introducing Multimodal Data Support, incorporating MRI image tensors alongside our tabular data to increase predictive power using ensemble networks.
$$ \hat{y}{ensemble} = w_1 \cdot P{tabular} + w_2 \cdot P_{image} $$
We believe Cogaly proves that student hackers can build tools that are not only technically impressive but ethically designed and operationally safe.



Log in or sign up for Devpost to join the conversation.