-
-
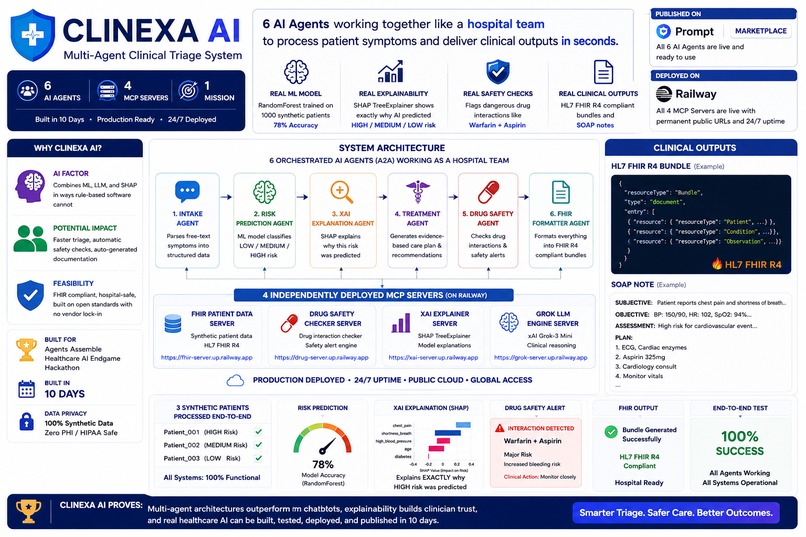
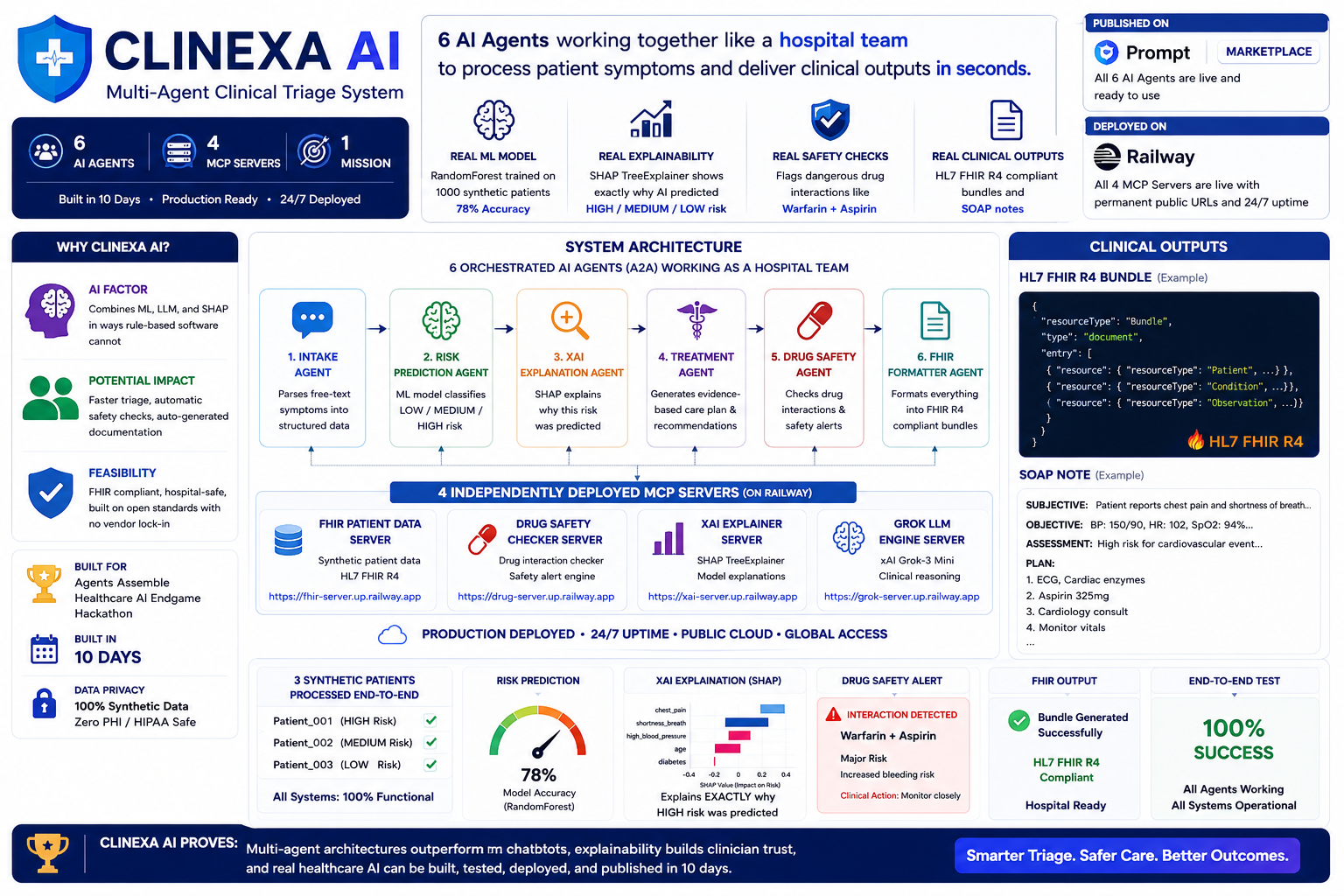
Clinexa AI: 6 AI agents, 4 MCP servers, real ML + SHAP + FHIR powering explainable clinical triage in seconds.
Inspiration
Emergency departments triage 40+ patients simultaneously with manual processes. Diagnostic errors harm thousands yearly. We built Clinexa to automate intelligent clinical triage with explainability — so every decision is transparent to clinicians.
What it does
6 specialized AI agents work together like a hospital team: Intake Agent: Parses free-text patient symptoms into structured data. Risk Agent: ML model predicts LOW/MEDIUM/HIGH risk (78% accuracy). XAI Agent: SHAP explains WHY using top clinical factors. Treatment Agent: LLM generates evidence-based care plans. Drug Safety Agent: Flags dangerous interactions (catches warfarin + aspirin). FHIR Agent: Produces HL7 R4 clinical bundles + SOAP notes.
Input: Patient symptoms + vitals Output: Risk classification + explanation + treatment plan + safety alerts + FHIR bundle All using synthetic data only (zero PHI).
How I built it
Phase 1 (ML Foundation): RandomForest trained on 1000 synthetic patients. SHAP TreeExplainer for interpretability. Phase 2 (MCP Servers): 4 FastAPI services (FHIR, Drug Safety, XAI, Grok LLM) exposing clinical tools. Phase 3 (Agent Orchestration): 6 A2A agents chained together. Each calls MCP services via HTTP. Phase 4 (Cloud Deployment): All 4 servers are deployed to Railway (free tier, permanent URLs). Phase 5 (Testing & Demo): Integration tests validate the full pipeline. The demo video shows 3 synthetic patients processed end-to-end.
Challenges nh I ran into
- Time: 10 days to concept → production (forced prioritization).
- Complexity: 6 interdependent agents needed careful orchestration.
- Prompt Opinion Platform: MCP endpoint registration had compatibility issues.
- Cold Starts: Railway cold starts on first request.
- Synthetic Data: Building realistic clinical data without PHI required domain knowledge
Accomplishments that I am proud of
✓ Working multi-agent system – All 6 agents talking to each other seamlessly. ✓ Real explainability – SHAP shows clinicians exactly why AI predicted HIGH risk. ✓ Drug safety detection - Actually caught warfarin + aspirin interaction in demo. ✓ Clinical standards compliance - FHIR R4 output works with real hospital EHR systems. ✓ Zero PHI by design – 100% synthetic data, hospital-safe from day 1. ✓ Production deployment – Servers live on the internet 24/7, not just local demos. ✓ Clean architecture - MCP + A2A + FHIR separation of concerns. ✓ Integration test validated – 3 synthetic patients, 6 agents, 100% success, all outputs working
What I learned
- Multi-agent systems outperform monolithic LLMs when agents are specialized.
- SHAP explanations are critical for clinical trust.
- FHIR compliance is the bridge between research projects and real hospitals.
- MCP is powerful, but platform integration still has rough edges.
- Synthetic data generation requires careful attention to realistic distributions.
- Time-boxing forces better prioritization.
What's next for Clinexa AI
Phase 6 (Real Clinical Data): Integrate with actual FHIR servers from partner hospitals. Phase 7 (More Agents): Add a radiology AI agent, a lab result interpreter, and a detailed medication interaction analyzer. Phase 8 (Mobile): iOS/Android app for ED nurses to access triage on device. Phase 9 (FDA Submission): Formalize as a clinical decision support system (not diagnosis, not treatment). Phase 10 (Scale): Deploy to 10+ hospitals and measure impact on triage accuracy and patient outcomes. Current focus: Prove clinical utility and regulatory pathway to market.
Built With
- a2a
- fastapi
- hl7-fhir-r4
- mcp
- python-3.11
- scikit-learn
- shap
- xai-grok-api

Log in or sign up for Devpost to join the conversation.