-
-

-
Research Paper Figure
-
Research Paper Figure
-
Research Paper Figure
-
Research Paper Figure
-
Research Paper Figure
-
Research Paper Figure
-
Research Paper Figure

ClearPath: FHIR-Native Prior Authorization Readiness Agent
ClearPath is a Prompt Opinion agent workflow that converts fragmented clinical context into a clinician-review prior authorization readiness packet.
I built ClearPath for the healthcare AI “last mile”: the gap between raw AI intelligence and a safe, actionable deliverable that can actually fit into a clinician workflow.
This project was created for the Agents Assemble: The Healthcare AI Endgame Challenge, which focuses on building interoperable healthcare agents at the intersection of MCP, A2A, FHIR, and Prompt Opinion’s SHARP-style healthcare context propagation.
Inspiration
Prior authorization is one of the most frustrating administrative workflows in healthcare.
A clinician may already know why a medication is clinically reasonable, but the authorization packet still requires evidence from many places:
- diagnoses
- laboratory results
- medication history
- prior therapy failures or intolerance
- clinical notes
- payer criteria
- contraindication documentation
- safety confirmations
This is exactly the “last mile” problem Prompt Opinion describes: raw intelligence is not enough. Healthcare AI needs to produce a concrete deliverable that a clinician can review and act on.
ClearPath was inspired by that idea.
Instead of building an AI agent that simply answers questions, I built an agent that helps prepare a prior authorization readiness packet.
The goal is not to replace a clinician or make a coverage decision. The goal is to reduce administrative burden by organizing the evidence, identifying missing documentation, and generating a clinician-review packet.
What ClearPath Does
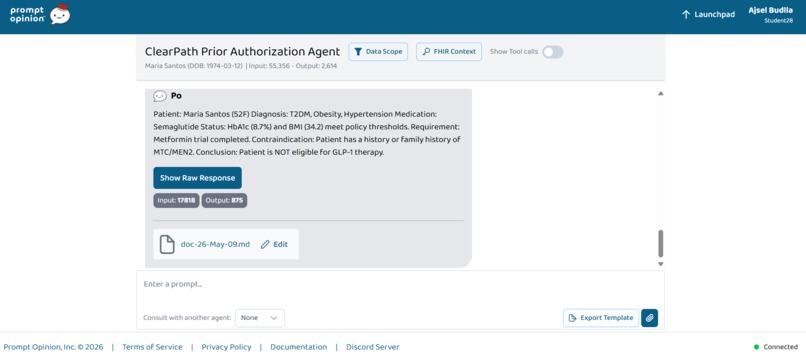
ClearPath evaluates a synthetic patient, Maria Santos, for semaglutide GLP-1 therapy.
The patient case includes:
- Patient: Maria Santos, 52-year-old female
- Conditions: Type 2 diabetes mellitus, obesity, hypertension
- Requested therapy: Semaglutide GLP-1 therapy
- Current medication: Metformin 1000 mg twice daily
- Prior medication: Glipizide, discontinued due to symptomatic hypoglycemia
- HbA1c: 8.7%
- BMI: 34.2 kg/m²
- Missing documentation: family history confirmation for medullary thyroid carcinoma or MEN2
ClearPath generates a structured prior authorization readiness packet with:
- Requested therapy
- Patient summary
- Key evidence found
- Policy criteria match table
- Missing documentation
- Draft prior authorization letter
- Clinician review note
The final status is:
Ready for clinician review with missing documentation.
ClearPath does not:
- prescribe therapy
- submit prior authorization
- guarantee approval
- make a final coverage decision
- replace clinician judgment
Why This Matters
Prior authorization is painful because it is not just a form. It is an evidence-alignment problem.
A complete prior authorization packet requires alignment among:
Patient facts
↔ Policy requirements
↔ Safety constraints
ClearPath helps close that gap.
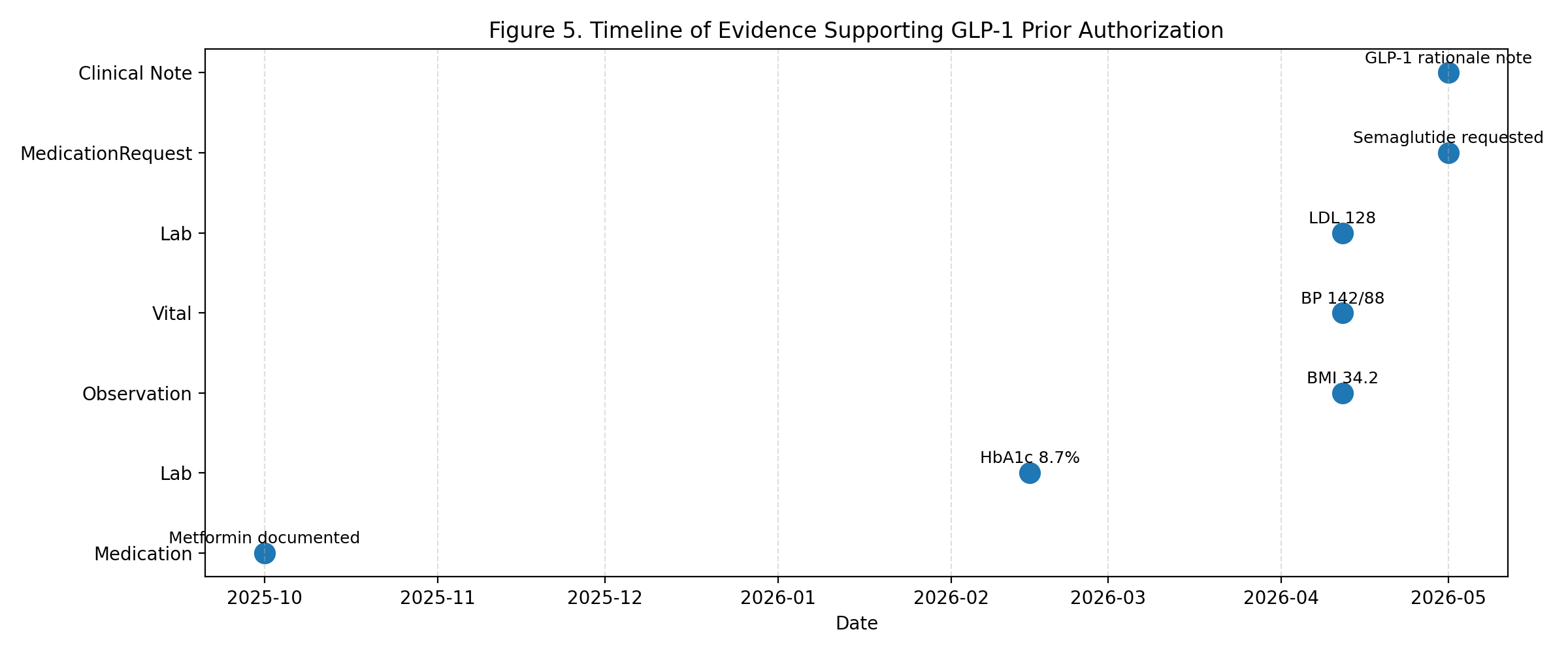
For the demo patient, ClearPath identifies the following supporting evidence:
- Type 2 diabetes diagnosis
- HbA1c of 8.7%
- BMI of 34.2 kg/m²
- current metformin therapy
- prior glipizide intolerance
- documented rationale for GLP-1 therapy
It also identifies the missing safety item:
Family history of medullary thyroid carcinoma or MEN2 is missing or unknown and requires clinician confirmation.
This is the most important safety behavior in the project.
ClearPath does not hallucinate missing safety documentation. It does not treat unknown family history as approval-ready evidence.
The Core Safety Principle
The most important rule in ClearPath is:
Unknown family history ≠ no family history
Unknown family history ≠ positive family history
The correct interpretation is:
Missing documentation requiring clinician confirmation.
This matters because GLP-1 therapies such as semaglutide require careful contraindication review for personal or family history of medullary thyroid carcinoma or MEN2.
ClearPath keeps that uncertainty visible instead of hiding it.
Technical Architecture
ClearPath was built around Prompt Opinion’s interoperability model.
The workflow is:
Prompt Opinion Launchpad
→ Patient context
→ FHIR Context
→ ClearPath Prior Authorization Agent
→ GLP-1 policy criteria
→ Evidence matching
→ Clinician-review packet
The project includes:
- ClearPath Prior Authorization Agent
- GLP-1 Policy Criteria Agent
- A2A-style agent composition
- FHIR-style synthetic patient bundle
- Reusable skill:
extract-glp1-prior-auth-criteria - Policy-grounded prior authorization template
- MCP-style technical simulation in Colab
- Research figures
- Readiness scoring model
- GitHub repository
- Static project website
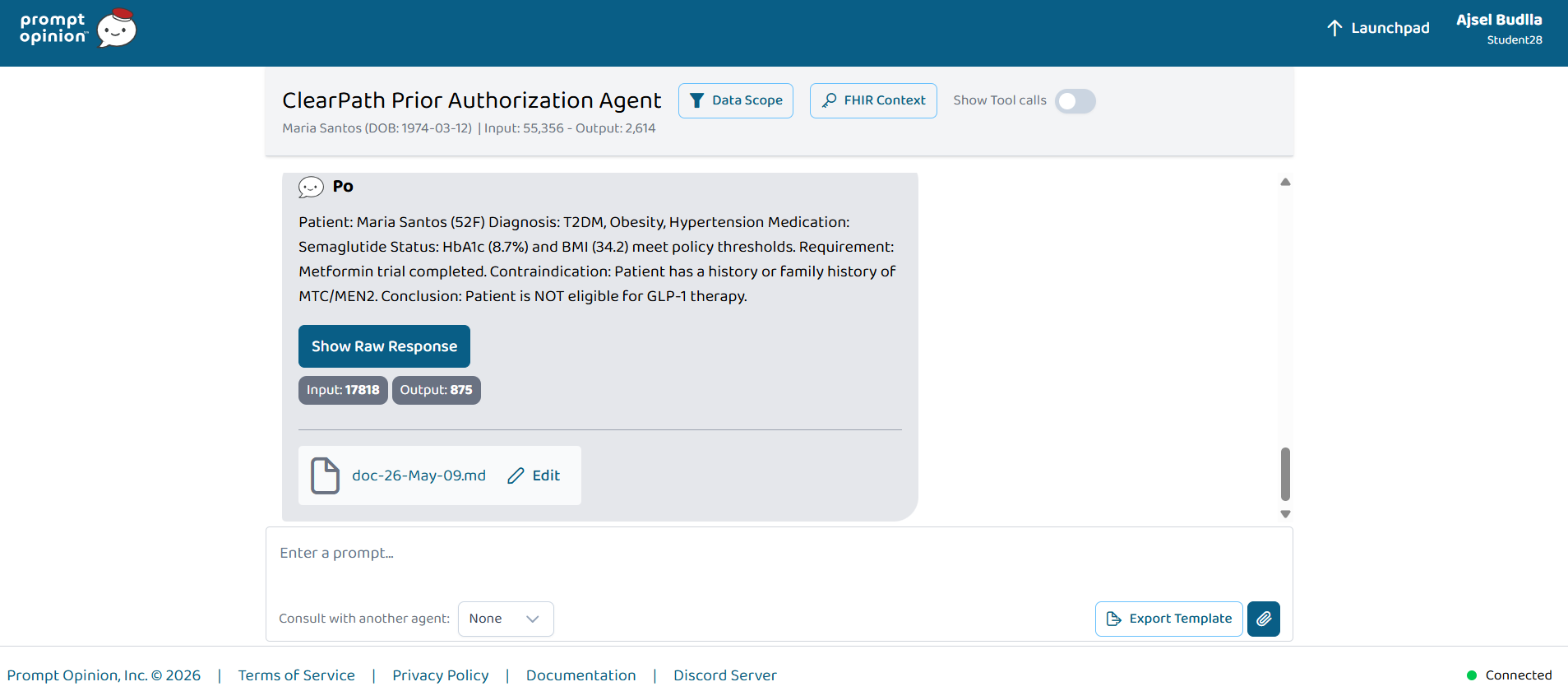
Prompt Opinion Implementation
I used Prompt Opinion as the main clinical agent environment.
The live workflow runs through:
- Prompt Opinion Launchpad
- Patient scope
- Maria Santos selected as the patient
- ClearPath Prior Authorization Agent
- FHIR Context visible
- GLP-1 prior authorization readiness output
I also configured a separate GLP-1 Policy Criteria Agent with A2A availability to represent the policy-specialist role.
This follows the challenge theme of building interoperable healthcare agents at the intersection of:
- MCP
- A2A
- FHIR
- SHARP-style context propagation
- Prompt Opinion agent composition
Agent Components
1. ClearPath Prior Authorization Agent
This is the main workflow agent.
Its role is to:
- receive patient context
- use GLP-1 policy criteria
- identify supporting evidence
- detect missing documentation
- generate a clinician-review packet
- avoid unsafe claims
The ClearPath agent is responsible for the final prior authorization readiness packet.
2. GLP-1 Policy Criteria Agent
This is the policy-specialist agent.
Its role is to extract GLP-1 prior authorization criteria from payer policy content.
It is designed to return:
- criterion name
- required evidence
- whether the criterion is mandatory
- missing documentation guidance
- clinician-review safety note
This agent was configured with A2A availability so it can be consulted by other agents.
3. Reusable Skill
I created a reusable skill named:
extract-glp1-prior-auth-criteria
The skill is designed to extract GLP-1 prior authorization criteria from policy documents and return a structured checklist.
It focuses on:
- Type 2 diabetes diagnosis
- HbA1c threshold
- metformin or prior therapy requirement
- BMI documentation
- therapy rationale
- contraindication review
- MTC/MEN2 family history documentation
FHIR-Style Data Model
The technical notebook models the patient using FHIR-style resources.
The synthetic FHIR bundle includes:
PatientConditionMedicationRequestMedicationStatementObservationDocumentReference
These resources represent the evidence needed for the prior authorization packet.
Examples:
| FHIR Resource | Purpose |
|---|---|
Patient |
Maria Santos demographics |
Condition |
Type 2 diabetes, obesity, hypertension |
MedicationRequest |
Semaglutide request and metformin therapy |
MedicationStatement |
prior glipizide intolerance |
Observation |
HbA1c, BMI, blood pressure, LDL |
DocumentReference |
clinical note and rationale |
This structure shows how ClearPath can operate on realistic healthcare data patterns rather than only free-text prompts.
MCP-Style Tool Design
The Colab technical simulation models ClearPath as a sequence of MCP-style tools.
The simulated tools are:
get_patient_evidence_snapshot
extract_glp1_policy_criteria
match_patient_to_policy
generate_prior_auth_packet
Tool 1: get_patient_evidence_snapshot
This tool extracts patient evidence from FHIR-style resources.
It collects:
- diagnoses
- labs
- vitals
- medication history
- prior therapy history
- clinical note evidence
- safety documentation
The evidence snapshot can be represented as:
$$ E = {D, L, M, P, R, S} $$
Where:
- \(D\) = diagnoses
- \(L\) = laboratory and vital observations
- \(M\) = medication history
- \(P\) = prior therapy history
- \(R\) = documented clinical rationale
- \(S\) = safety documentation
Tool 2: extract_glp1_policy_criteria
This tool converts policy text into structured criteria.
The criteria set is:
$$ C = {c_1, c_2, ..., c_n} $$
Each criterion can be represented as:
$$ c_i = (\text{name}_i, \text{required evidence}_i, \text{mandatory}_i, \text{policy note}_i) $$
For the GLP-1 use case, the criteria include:
- Type 2 diabetes diagnosis
- HbA1c threshold
- metformin trial
- BMI documentation
- therapy rationale
- absence of personal or family history of MTC/MEN2
Tool 3: match_patient_to_policy
This tool compares patient evidence against policy criteria.
Each criterion receives a status:
met
needs review
missing
The scoring model is:
$$ m_i = \begin{cases} 1, & \text{criterion is met} \ 0.5, & \text{criterion needs review} \ 0, & \text{criterion is missing} \end{cases} $$
Tool 4: generate_prior_auth_packet
This tool generates the final clinician-facing packet.
The packet is modeled as:
$$ P = f(E, C, M, G) $$
Where:
- \(E\) = patient evidence
- \(C\) = policy criteria
- \(M\) = match results
- \(G\) = safety guardrails
The final packet includes evidence, missing documentation, and clinician-review language.
Readiness Scoring
The technical notebook models prior authorization readiness as:
$$ R = \frac{\sum_{i=1}^{n} w_i m_i}{\sum_{i=1}^{n} w_i} $$
Where:
- \(R\) = readiness score
- \(w_i\) = criterion weight
- \(m_i\) = match score for criterion \(i\)
In this prototype, all criteria have equal weight:
$$ w_i = 1 $$
Each criterion is scored as:
met = 1.0
needs review = 0.5
missing = 0.0
For the demo patient:
$$ R = \frac{1 + 1 + 1 + 1 + 1 + 0}{6} $$
$$ R = 83.3\% $$
The missing criterion is:
Family history confirmation for medullary thyroid carcinoma or MEN2.
Therefore, the final status is:
Ready for clinician review with missing documentation.
Safety Gating Logic
ClearPath uses a specific safety gate for MTC/MEN2 documentation.
The safety gate is:
$$ g_{\text{MTC/MEN2}} = \begin{cases} 1, & \text{absence of personal and family history is explicitly documented} \ 0, & \text{family history is missing, unknown, or ambiguous} \end{cases} $$
The status rule is:
$$ \text{Status} = \begin{cases} \text{Ready for clinician review}, & R = 100\% \text{ and } g_{\text{MTC/MEN2}} = 1 \ \text{Ready for clinician review with missing documentation}, & R < 100\% \text{ or } g_{\text{MTC/MEN2}} = 0 \end{cases} $$
This prevents the system from converting missing information into a false conclusion.
Algorithm
Input:
Patient context P
FHIR evidence bundle F
Policy document D
Requested therapy T
Output:
Prior authorization readiness packet R
1. Select patient in Prompt Opinion Launchpad.
2. Propagate patient-scoped FHIR/SHARP context.
3. Extract structured patient evidence:
diagnoses
observations
medication history
prior therapy history
clinical notes
4. Extract GLP-1 policy criteria from the policy document.
5. For each policy criterion:
identify required evidence
search patient evidence
assign status: met, missing, or needs review
6. Apply safety gates:
do not infer absent MTC/MEN2 history from missing documentation
do not claim approval
do not prescribe
do not submit authorization
7. Compute readiness score.
8. Generate clinician-review packet:
requested therapy
patient summary
key evidence
policy criteria match table
missing documentation
draft letter
clinician review note
9. Return the packet inside Prompt Opinion.
Research Figures
The project includes research-style figures generated in Colab.
The most important figures are:
Figure 1: ClearPath Architecture
This figure shows the end-to-end workflow:
Prompt Opinion Launchpad
→ Patient Context
→ SHARP/FHIR Context Propagation
→ ClearPath Prior Authorization Agent
→ Policy Matching
→ Prior Authorization Readiness Packet
It also shows the GLP-1 Policy Criteria Agent and FHIR resources as supporting components.
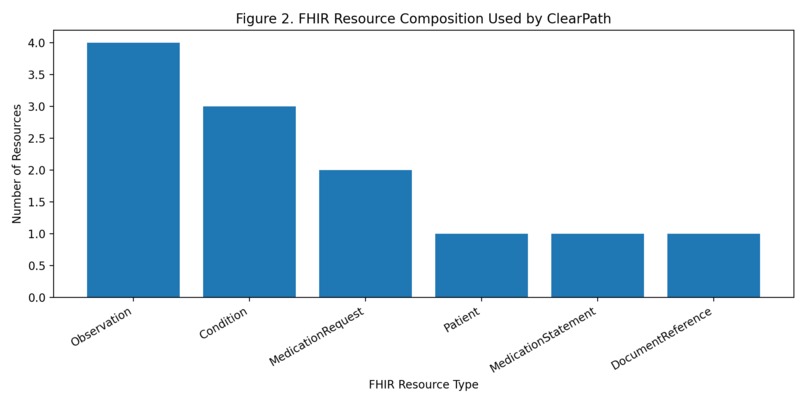
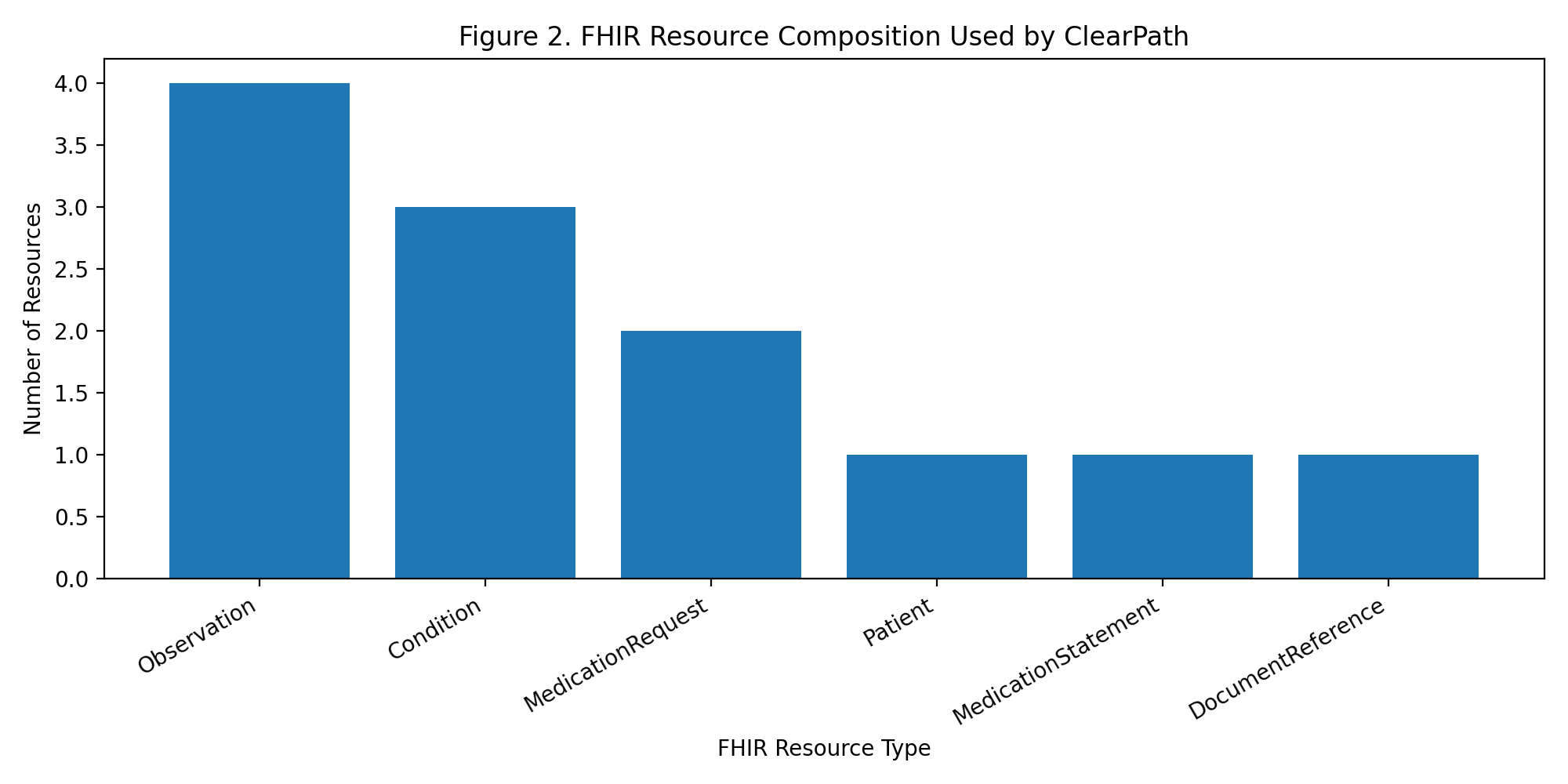
Figure 2: FHIR Resource Composition
This figure shows the FHIR-style resources used in the technical simulation.
The resource model includes:
- Observations
- Conditions
- MedicationRequests
- Patient
- MedicationStatement
- DocumentReference
This supports the feasibility of using FHIR-style data as the evidence layer.
Figure 4: Evidence Completeness Matrix
This is one of the most important figures.
It shows that the system has evidence for:
- Type 2 diabetes mellitus
- HbA1c threshold
- metformin trial
- BMI documentation
- GLP-1 rationale
But it does not have evidence for:
- absence of MTC/MEN2 family history
That missing item is intentionally preserved as a documentation gap.
Figure 7: Agent Orchestration Trace
This figure shows the workflow sequence:
- Prompt Opinion Launchpad
- SHARP/FHIR Context
- ClearPath Prior Authorization Agent
- GLP-1 Policy Criteria Agent
- MCP-style evidence snapshot
- MCP-style policy matching
- MCP-style packet generation
- Safety layer
This demonstrates that ClearPath is designed as an interoperable workflow, not just a chatbot.
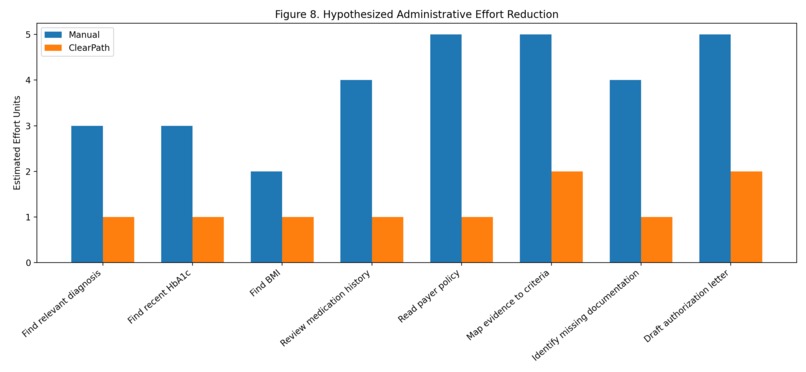
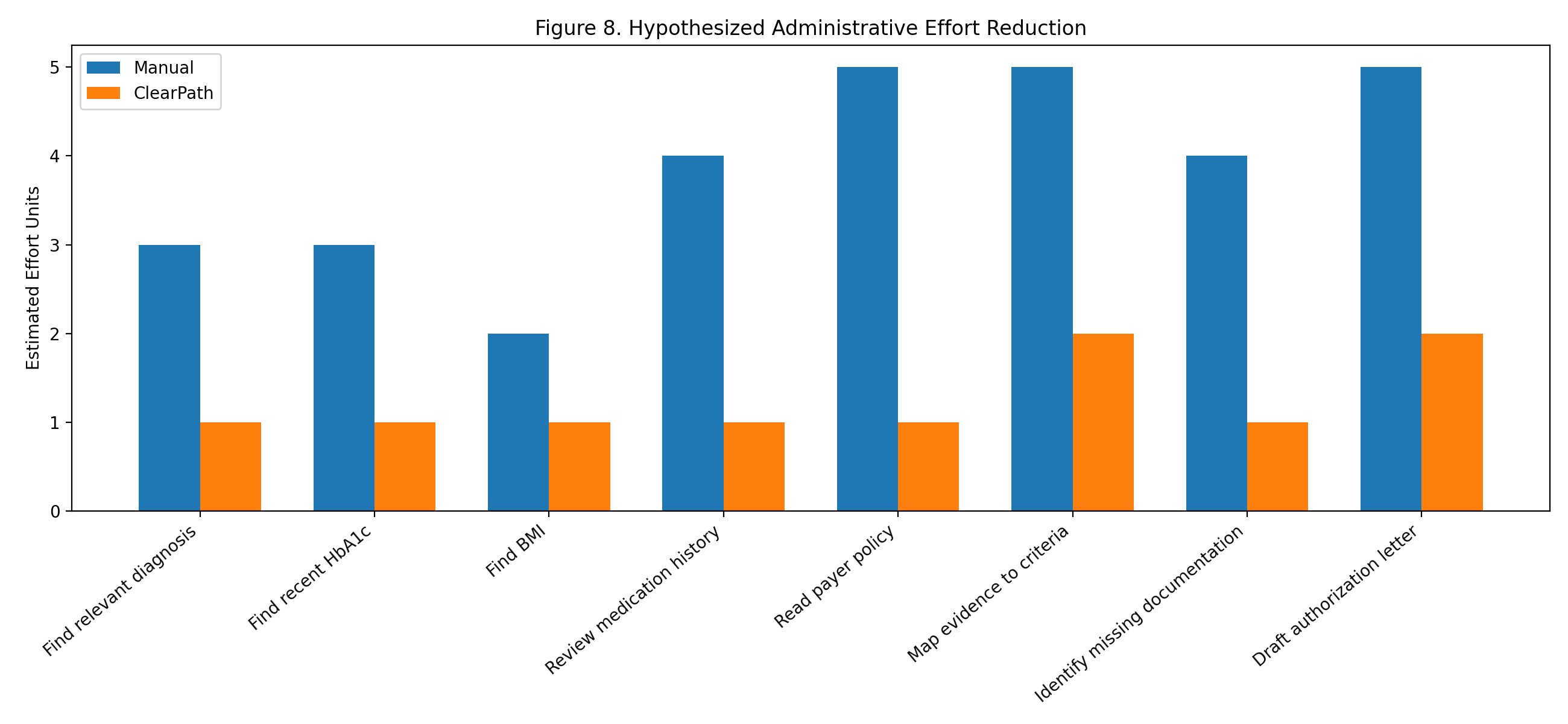
Figure 8: Hypothesized Administrative Effort Reduction
This figure compares manual workflow effort against ClearPath-assisted effort.
The estimate shows a reduction from 31 manual effort units to 10 assisted effort units.
The hypothesized reduction is:
$$ \frac{31 - 10}{31} \times 100 = 67.7\% $$
This is not a measured clinical study result. It is a hypothesis-generating estimate showing the type of administrative burden ClearPath targets.
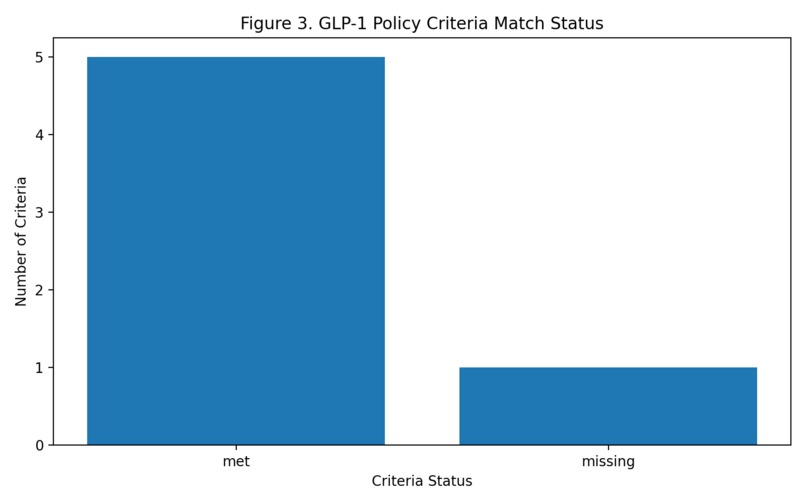
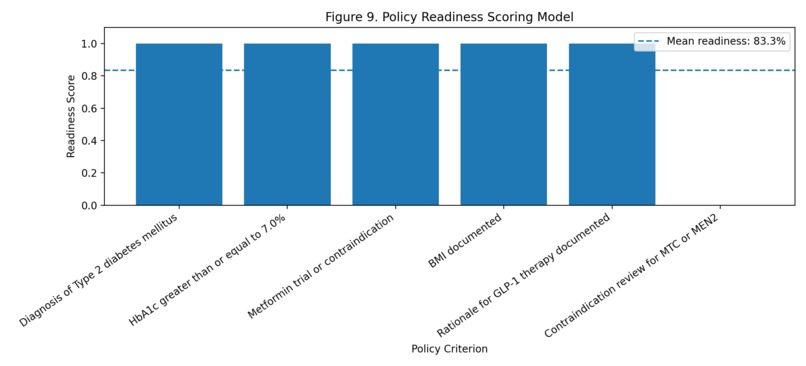
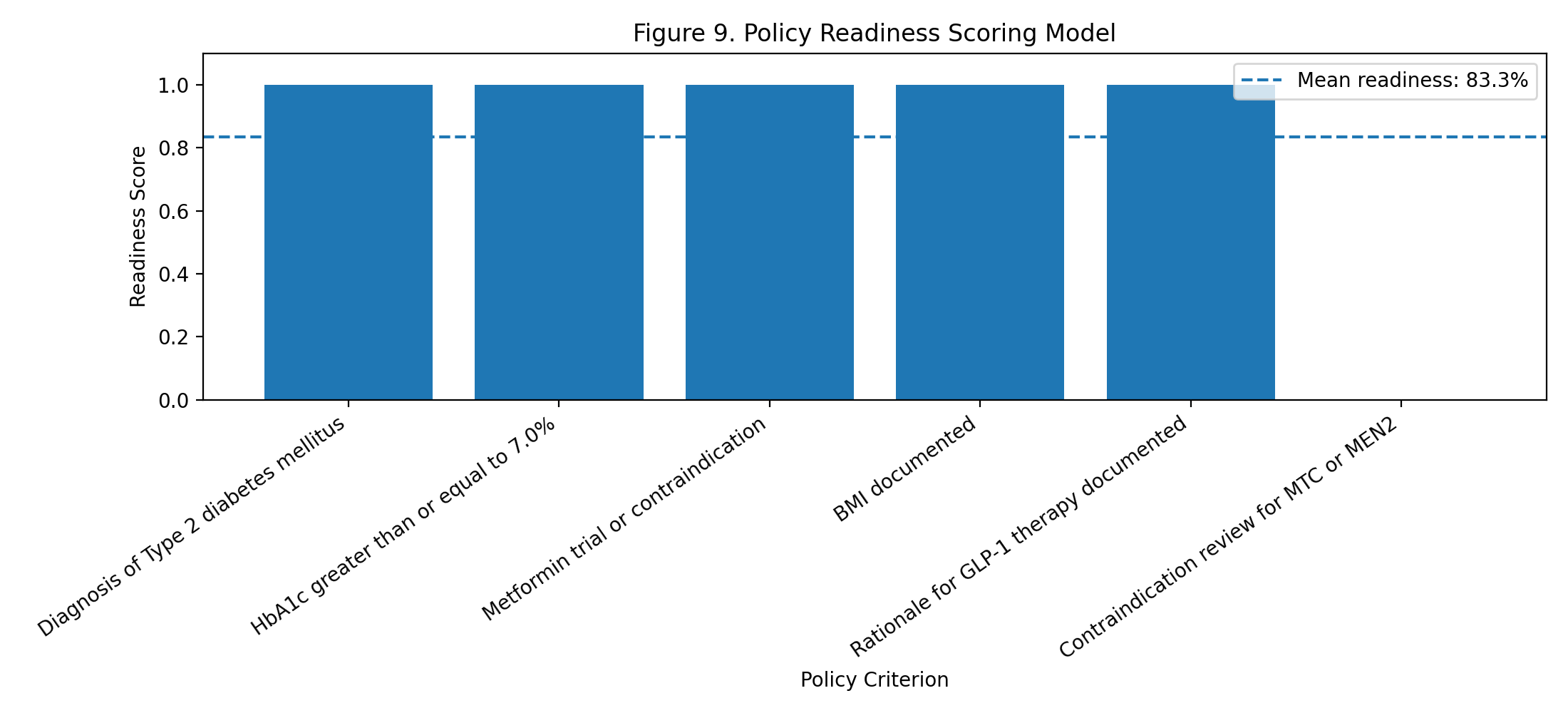
Figure 9: Policy Readiness Scoring Model
This figure shows the 83.3% readiness score.
Five criteria are met.
One safety criterion is missing.
The missing criterion prevents the packet from being marked fully ready.
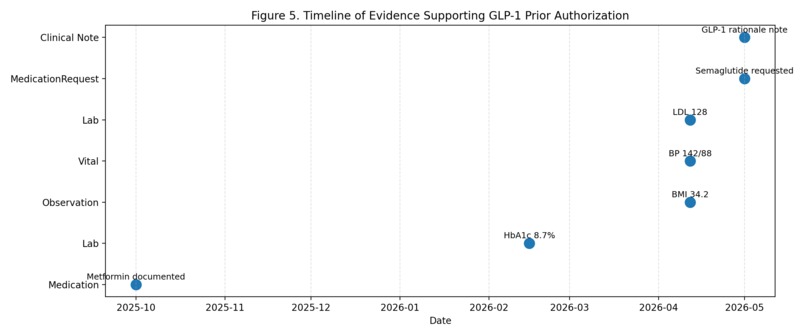
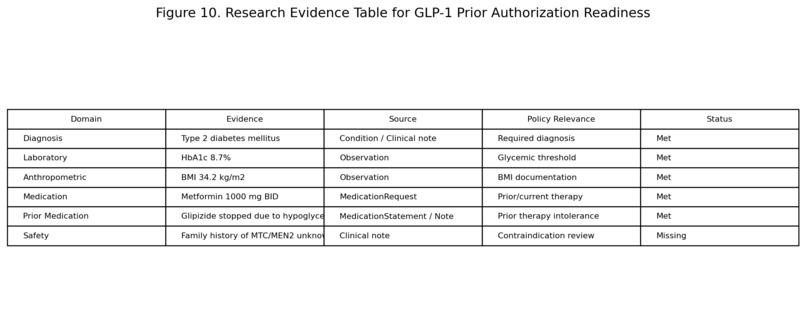
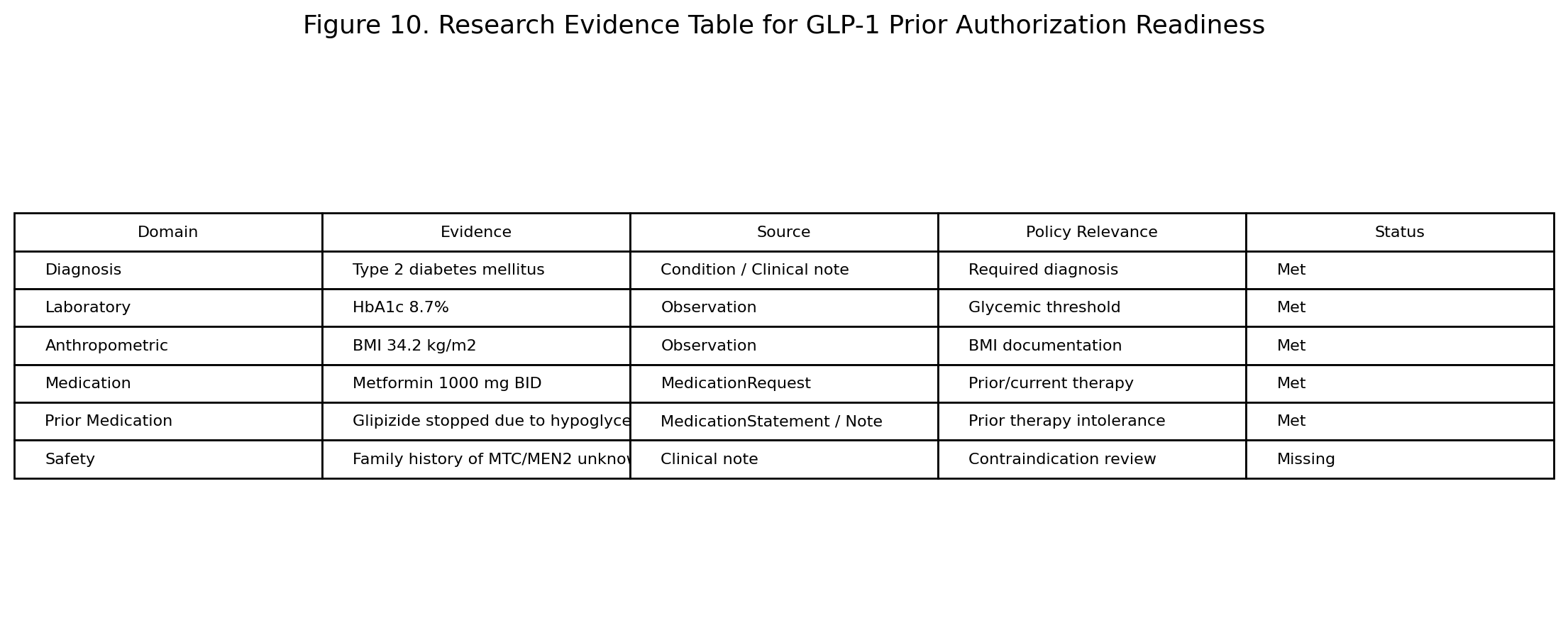
Figure 10: Research Evidence Table
This figure summarizes the full case:
| Domain | Evidence | Source | Policy Relevance | Status |
|---|---|---|---|---|
| Diagnosis | Type 2 diabetes mellitus | Condition / clinical note | Required diagnosis | Met |
| Laboratory | HbA1c 8.7% | Observation | Glycemic threshold | Met |
| Anthropometric | BMI 34.2 kg/m² | Observation | BMI documentation | Met |
| Medication | Metformin 1000 mg BID | MedicationRequest | Prior/current therapy | Met |
| Prior Medication | Glipizide stopped due to hypoglycemia | MedicationStatement / note | Prior therapy intolerance | Met |
| Safety | Family history of MTC/MEN2 unknown | Clinical note | Contraindication review | Missing |
This table is the clearest summary of the project’s value: ClearPath finds the evidence that exists and flags the evidence that is missing.
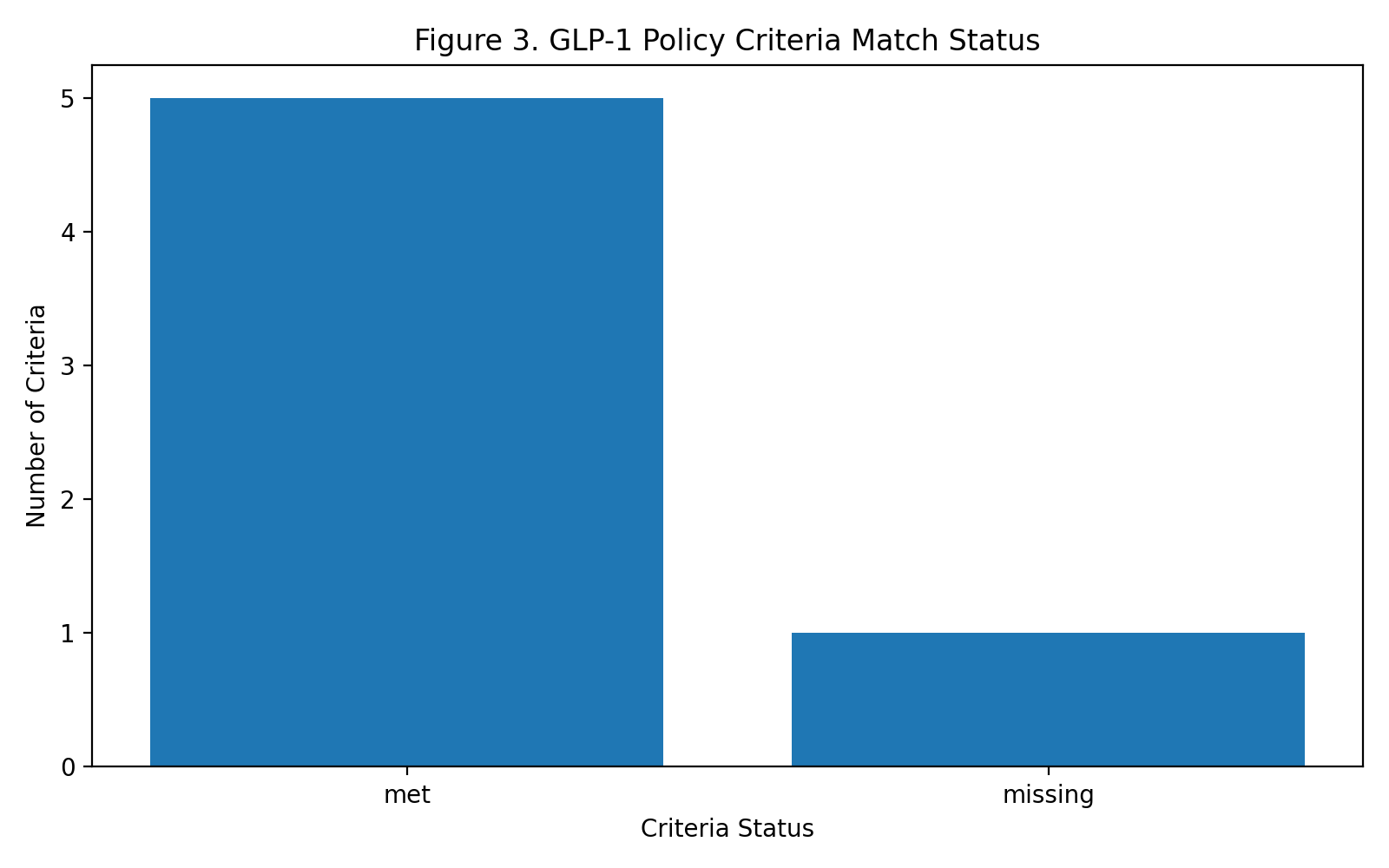
Results
ClearPath identified five GLP-1 prior authorization criteria as met:
- Type 2 diabetes diagnosis
- HbA1c threshold
- Metformin trial
- BMI documentation
- Therapy rationale
ClearPath identified one criterion as missing:
- Family history confirmation for medullary thyroid carcinoma or MEN2
The final readiness score was:
$$ 83.3\% $$
The final status was:
Ready for clinician review with missing documentation.
The final output was not:
- approved
- denied
- submitted
- prescribed
It was a clinician-review readiness packet.
Judging Criteria Alignment
AI Factor
ClearPath uses generative AI for a task that traditional rule-based software does not handle well.
A rules engine can check whether a field exists, but prior authorization often requires synthesis across:
- structured FHIR-style data
- unstructured clinical notes
- medication history
- policy criteria
- missing documentation
- safety constraints
ClearPath uses generative AI to assemble this context into a coherent, clinician-review packet.
The AI is not just answering a question. It is producing an actionable clinical-administrative artifact.
Potential Impact
Prior authorization is a major administrative burden.
ClearPath targets:
- reduced documentation search time
- fewer incomplete packets
- earlier identification of missing evidence
- reduced rework
- safer packet preparation
- clearer clinician review
- more structured handoff between clinical data and administrative requirements
The technical simulation estimated a possible administrative effort reduction of:
$$ 67.7\% $$
This is a hypothesis, not a clinical outcome claim, but it clearly shows the workflow burden ClearPath is designed to reduce.
Feasibility
ClearPath is designed around real healthcare constraints.
It is feasible because:
- it runs inside Prompt Opinion
- it uses patient-scoped context
- it models FHIR-style data
- it uses A2A-style agent composition
- it can be extended with MCP-style tools
- it uses clinician-review language
- it does not autonomously prescribe
- it does not autonomously submit authorization
- it does not guarantee approval
- it uses synthetic data only for the demo
- it explicitly flags missing documentation
The architecture respects the reality that healthcare AI should support clinicians, not bypass them.
What I Built
I built:
- a Prompt Opinion prior authorization agent
- a GLP-1 policy criteria agent
- an A2A-enabled policy specialist workflow
- a reusable skill package
- a synthetic FHIR transaction bundle
- a GLP-1 prior authorization policy document
- a readiness packet template
- a Colab technical notebook
- evidence extraction logic
- policy matching logic
- readiness scoring logic
- research visualizations
- a GitHub repository
- a static project website
What I Learned
I learned that healthcare AI should not be designed as one giant prompt.
It should be designed as a workflow with:
- context
- standards
- tools
- agents
- safety gates
- clinician review
The most important lesson was that uncertainty must be preserved.
A missing clinical fact should not be converted into a confident conclusion.
For ClearPath, the safest and most useful output is:
This packet is ready for clinician review, but family history documentation must be confirmed before submission.
Challenges
The hardest challenge was making the system both useful and safe.
Early testing showed that the model could incorrectly interpret missing MTC/MEN2 family history as a positive contraindication or as a final eligibility decision.
That failure mode was important because it showed why safety gates are necessary.
I addressed this by redesigning the workflow around:
- explicit missing-documentation language
- readiness scoring
- clinician-review status
- no approval claims
- no prescribing language
- no submission language
- uncertainty-preserving logic
This made the final project safer and more realistic.
Why ClearPath Is Not Just a Chatbot
ClearPath is not just a chatbot because it has:
- a defined clinical-administrative workflow
- patient-scoped context
- FHIR-style evidence representation
- policy criteria matching
- readiness scoring
- A2A-style policy agent design
- MCP-style tool simulation
- safety gates
- clinician-review output
- reusable artifacts
- research figures
- deployment-ready documentation
It does not simply respond to a prompt. It converts fragmented healthcare context into a structured deliverable.
Limitations
ClearPath is a prototype.
The current demo uses synthetic patient data.
The readiness score is a technical demonstration, not a validated clinical metric.
The administrative effort reduction is a hypothesis, not a measured outcome.
The A2A policy-agent path was configured, but the stable live demo used the main ClearPath workflow because long A2A calls sometimes caused latency issues.
The FHIR integration was modeled technically in Colab and represented in Prompt Opinion with patient context and FHIR Context visible.
A production version would need:
- direct FHIR querying
- payer-specific policy libraries
- audit logs
- source-level evidence citations
- clinician sign-off workflow
- privacy and security review
- real-world validation
Future Work
The next version of ClearPath would include a production MCP server with tools such as:
get_patient_evidence_snapshot
extract_policy_requirements
match_patient_to_policy
generate_prior_auth_packet
It would also include:
- direct FHIR queries using patient context
- stronger A2A orchestration
- shorter policy-agent responses to reduce latency
- evidence provenance for every generated claim
- source references such as Observation IDs and DocumentReference IDs
- support for multiple payer policies
- additional prior authorization categories
Possible future use cases include:
- MRI prior authorization readiness
- specialist referral readiness
- durable medical equipment requests
- high-cost biologic therapy authorization
- clinical trial pre-screening packets
Final Outcome
ClearPath demonstrates the healthcare AI endgame: converting raw intelligence into a standards-aligned, clinician-review deliverable.
It is not an autonomous decision-maker.
It is a safe administrative synthesis agent that helps clinicians prepare better prior authorization packets inside Prompt Opinion.
The final result is:
Ready for clinician review with missing documentation.
That is the core idea: useful, safe, interoperable healthcare AI that helps close the last mile without taking the clinician out of the loop.
Built With
- agent-to-agent-(a2a)-workflow-design
- chart.js
- css
- fhir-context
- github
- github-pages-/-netlify
- google-ai-studio
- google-colab
- google-gemini
- html
- javascript
- json
- latex
- markdown
- mcp-style-tool-architecture
- prompt-opinion
- prompt-opinion-a2a-agents
- prompt-opinion-launchpad
- prompt-opinion-marketplace-studio
- python
- sharp-style-context-propagation
- synthetic-fhir-transaction-bundle

Log in or sign up for Devpost to join the conversation.