-
Landing Page, Customer Profile
-
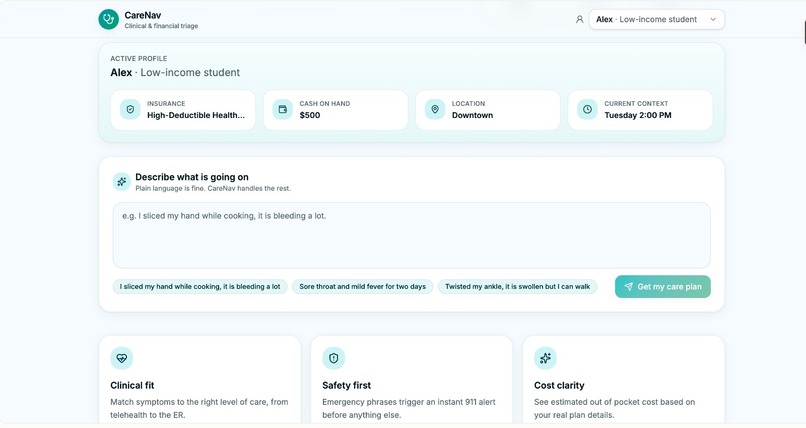
Current situation, describe situation/emergency
-
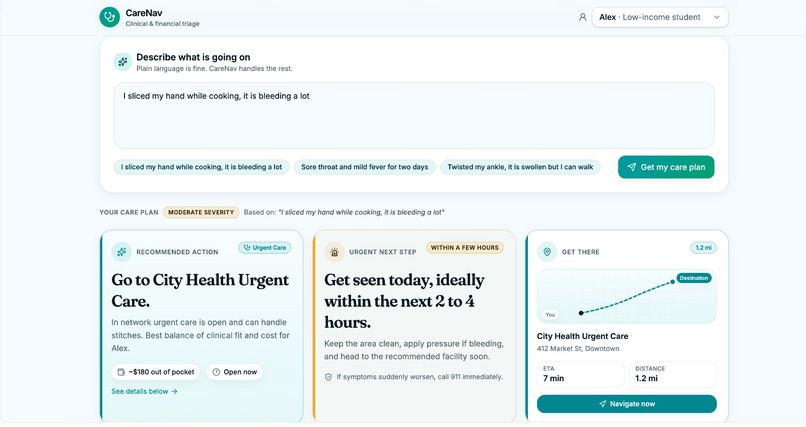
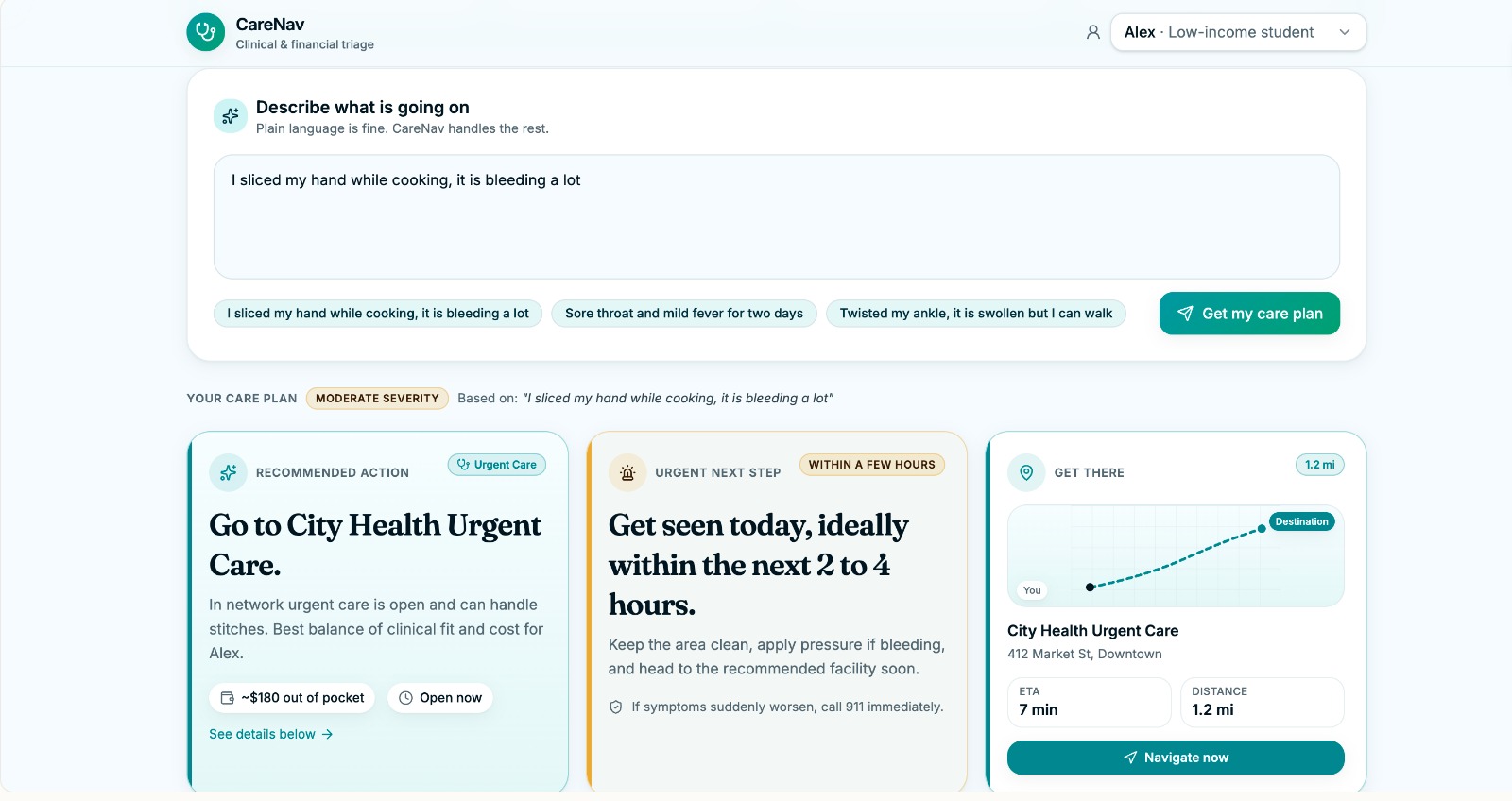
options for care
-
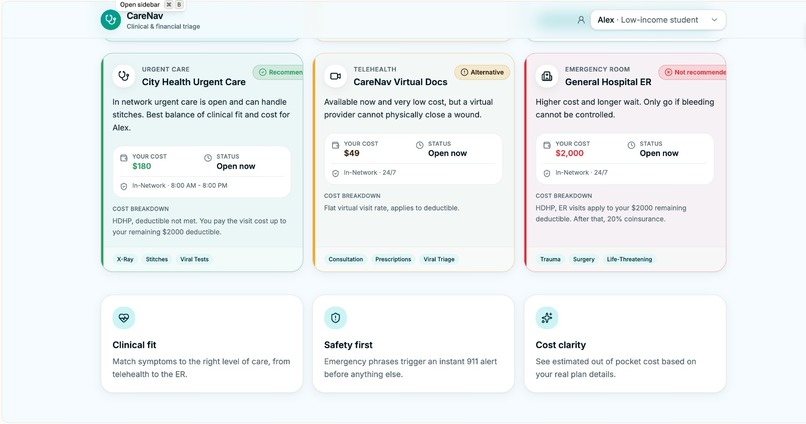
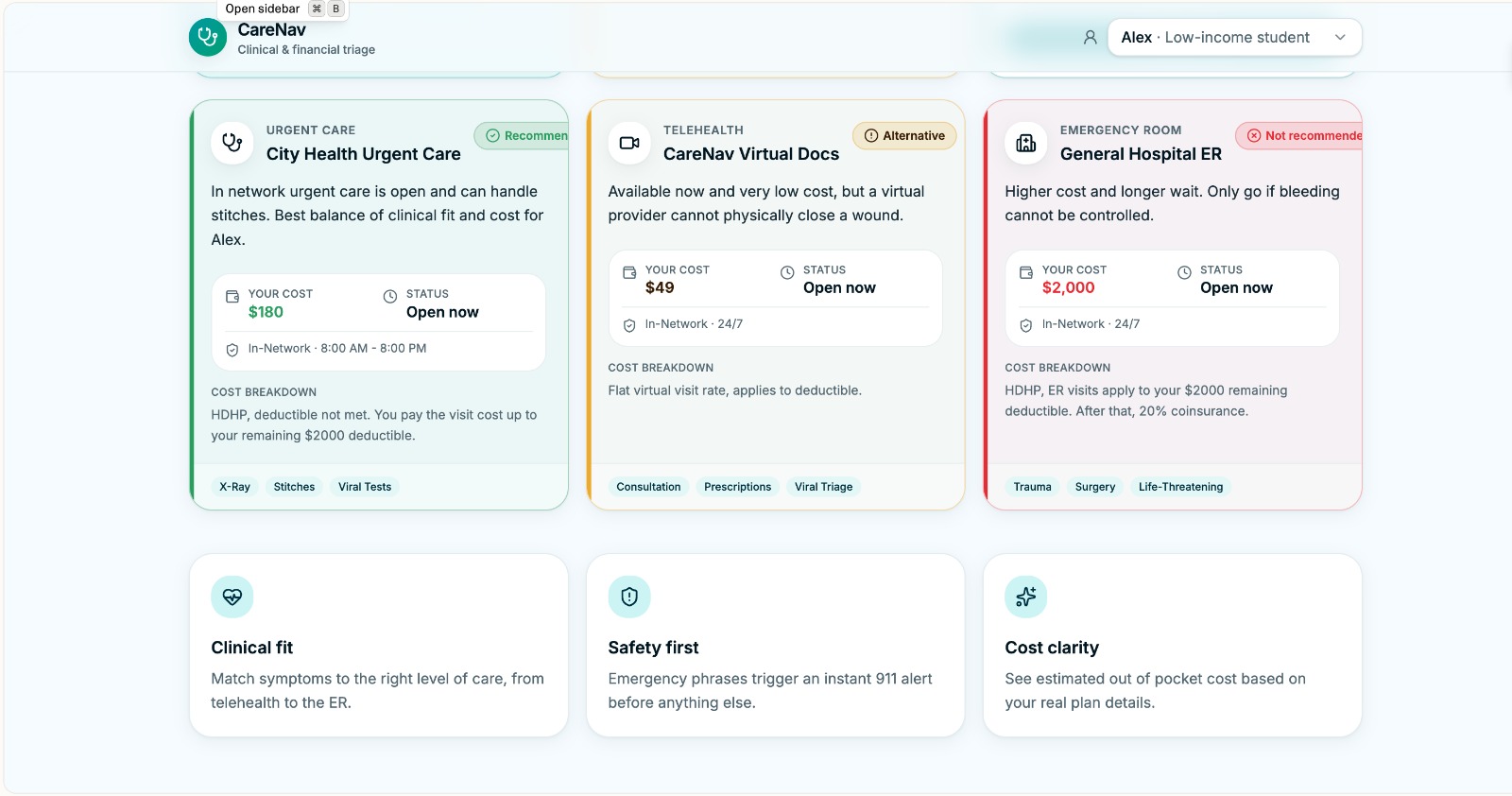
options for care 2
About CareNav
What Inspired Us
The American healthcare system forces patients to make critical medical decisions while blindfolded to the financial realities. We built CareNav for everyday patients—specifically students, young families, and the nearly 50% of Americans enrolled in high-deductible health plans. For these individuals, out-of-pocket costs must reach $2,500 to over $10,000 before their insurance even kicks in.
In this system, uncertainty is exorbitantly expensive. Patients are rarely equipped to determine whether a symptom requires an expensive ER visit or a much cheaper urgent care trip.
| Care Facility | Average Estimated Cost | Wait Time |
|---|---|---|
| Emergency Room | $1,200 – $3,000 | 2 to 4+ hours |
| Urgent Care | Under $200 | Typically < 1 hour |
Because of this dramatic disparity, 1 in 3 Americans delay care due to cost, which often worsens medical outcomes and ironically increases long-term expenses. We were inspired to build a tool that removes this friction, bringing absolute clarity to both medical urgency and financial impact in real time.
How We Built It
CareNav was built over a weekend sprint, operating as a sophisticated clinical and financial triage engine powered by Claude.
We engineered the application in two primary phases:
- Empathetic Intake: We utilized Claude as the front-line receiver. It is designed to take panicked, natural-language symptom descriptions (e.g., "I cut my hand on an avocado") and parse them into structured, medical-grade clinical categories.
- Simulated RAG Workflow: We leveraged Claude’s reasoning capabilities to power a Retrieval-Augmented Generation (RAG) flow. The system instantly cross-references the user's parsed symptoms with their specific, complex insurance profile and the operating hours of nearby medical facilities.
The output is our Decisiveness Dashboard: a tailored, cost-aware UI that presents highly actionable recommendations. Because we built this in a weekend, we relied on mocked insurance and facility availability data to prove the concept, setting the stage for future API integrations (like Zocdoc, Eligible, and PokitDok).
The Challenges We Faced
The single biggest challenge—and failure mode—in health-tech AI is under-triage: missing a life-threatening emergency in an attempt to optimize a user's wallet. With over 120 million ER visits occurring annually in the U.S., even a fractional error rate at scale would have severe, fatal consequences.
We had to carefully balance financial optimization against clinical risk. Mathematically, our core routing engine attempts to minimize the expected cost and wait time for a given facility $f$ from the set of available facilities $\mathcal{F}$:
$$\arg\min_{f \in \mathcal{F}} \left[ \mathbb{E}[C_{f}(I, S)] + \lambda \cdot t_{wait}(f) \right]$$
Where $C_{f}$ is the expected cost given insurance $I$ and symptoms $S$, $t_{wait}$ is the wait time, and $\lambda$ is the time-value weight. However, we realized that allowing an LLM to probabilistically weigh an acute cardiovascular event against a $2,000 ER bill was too dangerous.
Our Solution: We introduced a strict constraint to the optimization function based on a clinical risk score, $\rho(S)$. If the risk exceeds an emergent threshold ($\tau_{emergent}$), the system overrides the AI's cost-saving logic. If a user reports high-risk red flags—such as chest pain, shortness of breath, fainting, or neurological deficits—the platform triggers a hard-coded, full-screen emergency directive to call 911 or go to the nearest ER. No ambiguity, no trade-offs, just immediate escalation.
What We Learned
- Safety Cannot Be Probabilistic: We learned that when building AI for healthcare, you cannot rely entirely on an LLM's generative judgment for critical safety boundaries. Hard-coded guardrails and deterministic overrides are essential.
- Data Silos Are the Real Enemy: While simulating the RAG flow, we discovered just how fragmented healthcare data truly is. Nearly 60% of insured Americans do not understand their deductibles because the data is buried in legacy clearinghouses.
- Accessibility is Multi-Dimensional: Triage isn't just about reading a chart; it's about communication in high-stress moments. Recognizing that over 40% of adults have low health literacy, we learned that text inputs aren't always enough. This insight shaped our product roadmap, highlighting the crucial need for our future multilingual support and Voice Interface integrations to lower friction for underserved populations.
Built With
- accessible-ui-development.-*-**backend:**-[e.g.
- and-api-communications.-*-**database-&-storage:**-[e.g.
- and-the-simulated-retrieval-augmented-generation-(rag)-workflow.-*-**frontend:**-[e.g.
- anthropic
- api
- bootstrap
- claude
- clinical-categorization
- css
- eligible
- fastapi
- firebase
- flask
- handling-complex-natural-language-parsing
- html
- html/js]-was-used-to-build-the-responsive-decisiveness-dashboard-and-the-emergent-full-screen-override-ui.-*-**styling:**-[e.g.
- insurance-logic
- javascript
- json
- mongodb
- next.js
- nextjs
- node.js
- or-custom-css]-for-rapid
- or-firebase]-stored-the-mocked-user-profiles
- or-flask]-handled-the-routing-engine
- pokitdok
- postgresql
- python
- rag
- react
- risk-score-calculations
- tailwind
- tailwind-css
- zocdoc

Log in or sign up for Devpost to join the conversation.