One in five Medicare patients is readmitted to the hospital within 30 days of discharge. The majority of those readmissions are preventable, and the two biggest culprits are missed follow-up appointments and medication errors.
When a patient goes home without clearly understanding their new medication regimen, doses get skipped, old medications get taken alongside new ones, or a critical dosage change goes unnoticed. Adverse drug events from poor post-discharge communication affect over a million patients a year in the US alone, and they are one of the leading causes of emergency readmissions.
Missed follow-ups compound the problem. A patient who doesn't see their cardiologist two weeks after discharge doesn't get early warning signs caught. A wound that needed a check-in gets infected. A medication that needed adjusting stays wrong for another month. By the time the patient comes back, they come back sicker and through the emergency department.
Each unplanned readmission costs the healthcare system an average of $15,000–$20,000. Collectively, preventable readmissions cost the US $26 billion a year. CMS actively penalizes hospitals with high 30-day readmission rates under the Hospital Readmissions Reduction Program, so the financial pressure lands on both the discharging hospital and the receiving facility.
The root cause is almost always the same: the transition from hospital to post-acute care is a handoff that happens on paper, at the worst possible moment for the patient, with no system ensuring they actually understood what comes next.
That's the gap CareBridge closes.
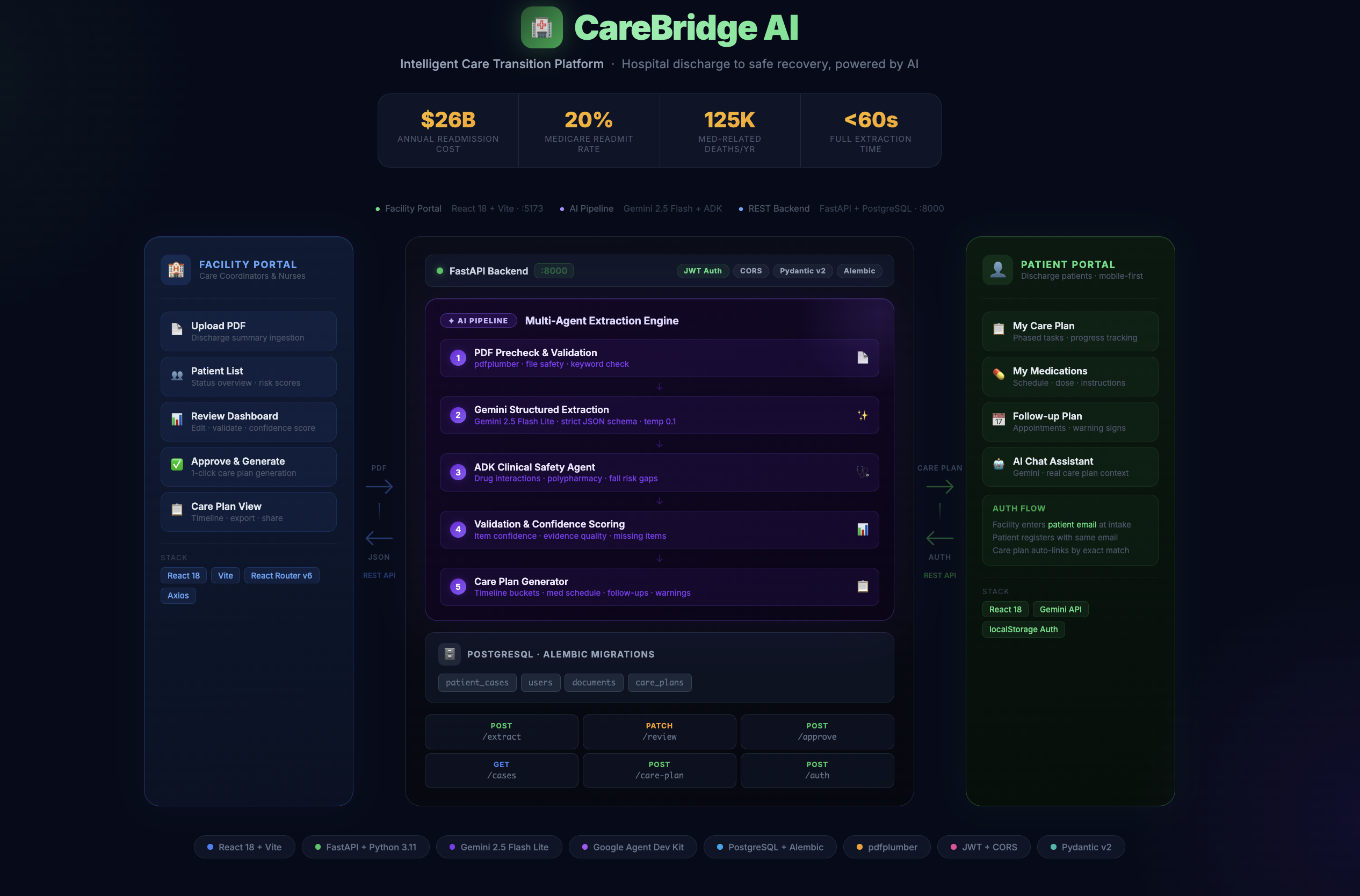
CareBridge turns a one-time discharge handoff into an active, coordinated safety net. Instead of relying on a patient to remember everything from a stressful discharge moment, CareBridge continuously monitors what happens next and intervenes early.
The Medication Safety Agent reconciles discharge medications against prior regimens, flags duplicate therapies, dangerous interactions, and missed dosage changes, then prompts staff and patients with clear, plain-language instructions before errors become adverse events. The Follow-Up Risk Agent identifies patients likely to miss specialist or primary-care visits, prioritizes outreach, and triggers reminders and escalation workflows so critical appointments happen on time. The Patient Summary and Normalization Agents convert fragmented records, notes, and discharge documents into a unified, actionable care view for post-acute teams. The Review Decision Agent helps care coordinators triage risk and decide the next best action quickly and consistently.
With CareBridge, medications are understood, follow-ups are completed, risks are surfaced early, and care teams act before deterioration leads to an avoidable readmission.
Built With
- alembic
- axios
- css
- deployment
- docker
- fastapi
- gemini-api
- genai
- godaddy
- javascript
- pdfplumber
- postgresql
- pydantic
- python
- railway
- react
- sql
- sqlalchemy
- tailwind
- vite











Log in or sign up for Devpost to join the conversation.