-
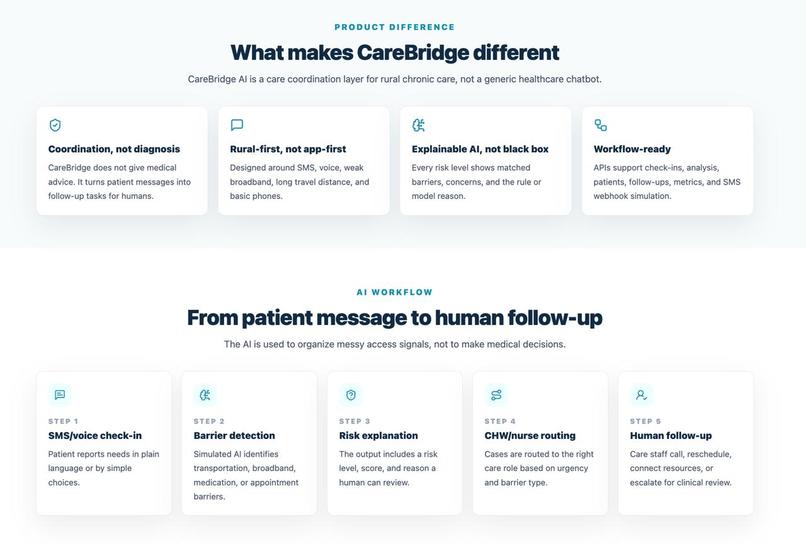
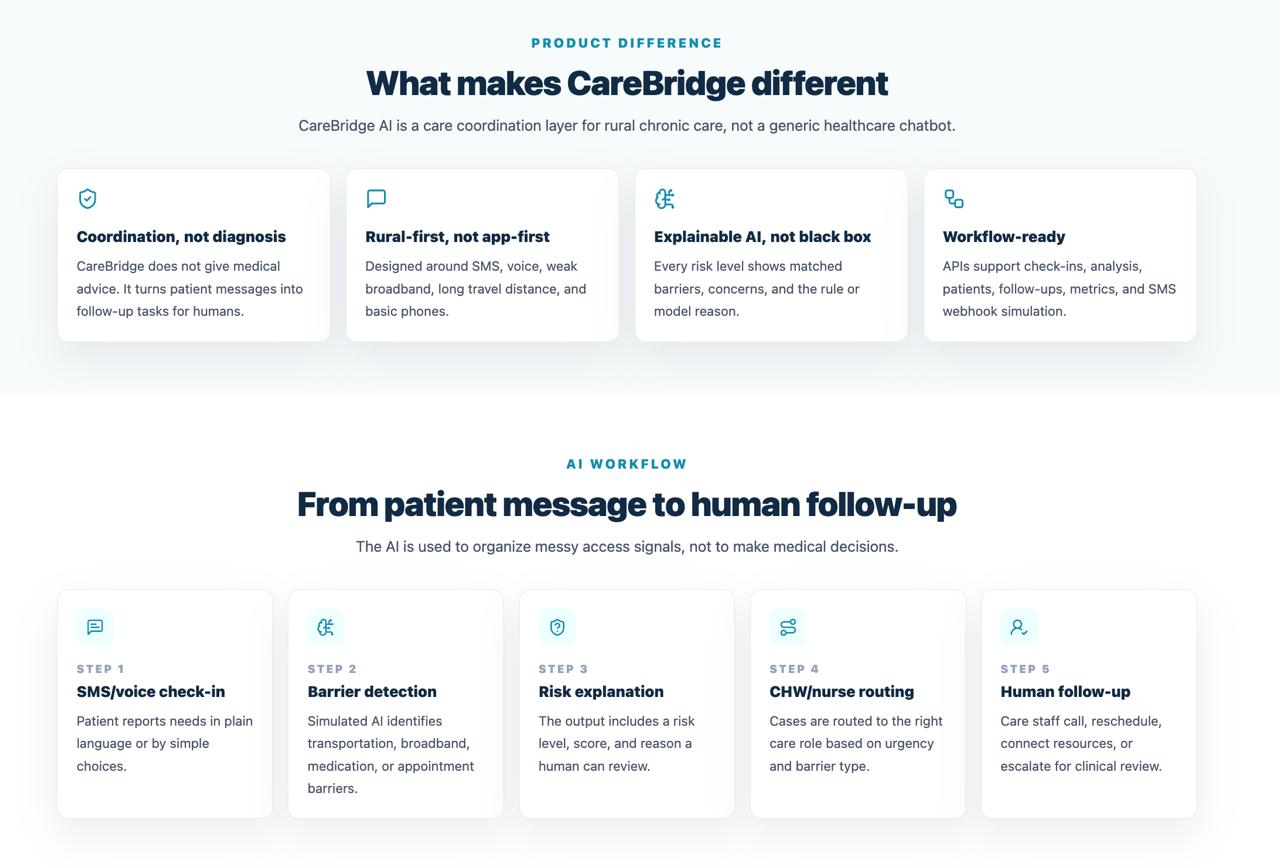
CareBridge is not a chatbot: it routes rural care needs to humans with explainable AI.
-
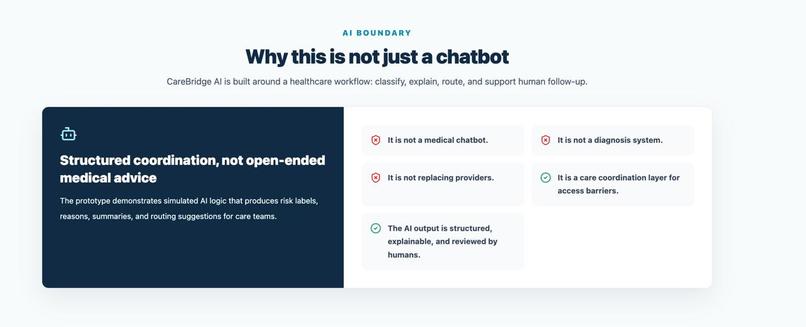
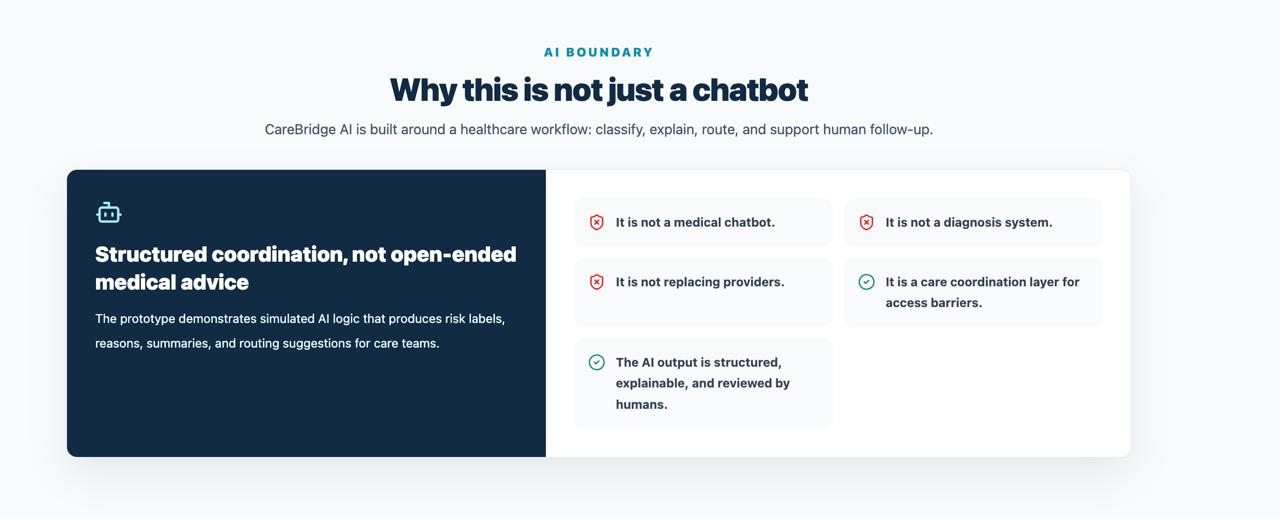
Safety boundary: not a chatbot, not diagnosis, not replacing providers.
-
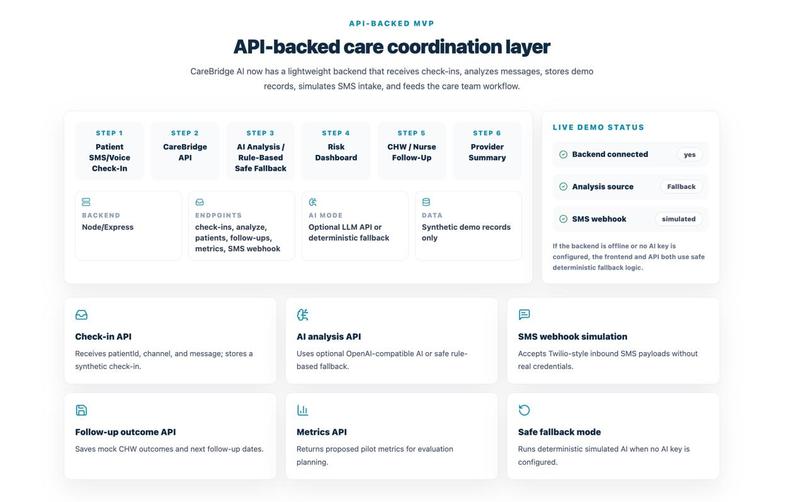
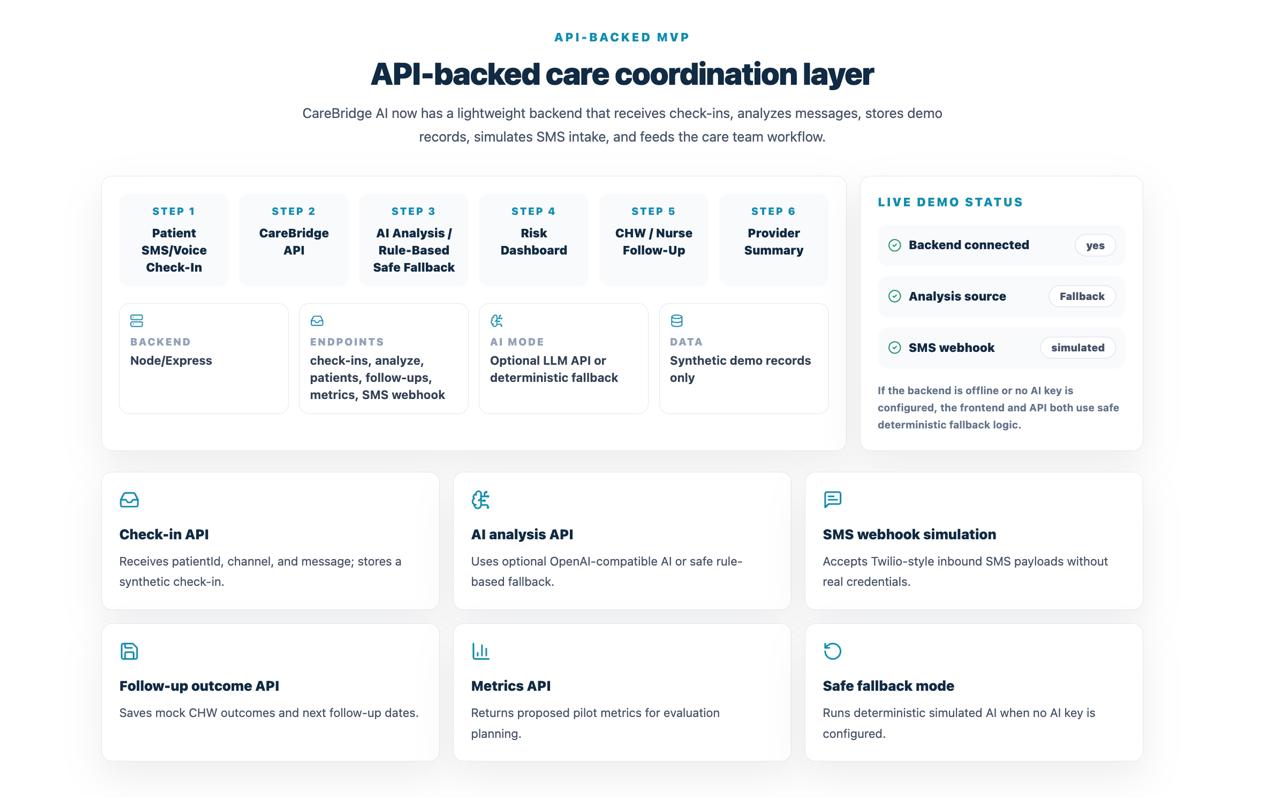
API-backed workflow: check-ins, analysis, fallback logic, dashboard, CHW follow-up, summary.
-
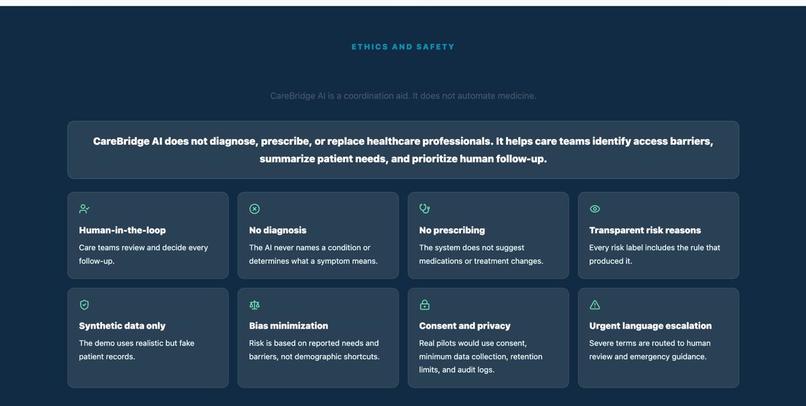
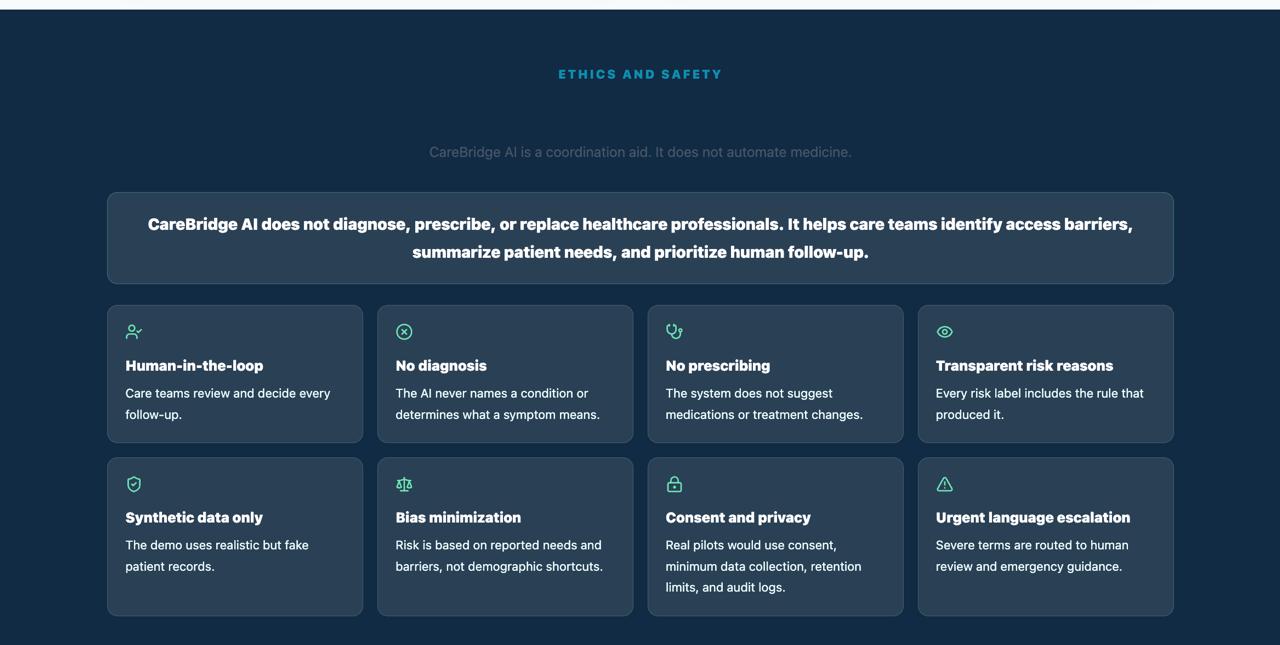
Ethics and safety: human review, no diagnosis, no prescribing, privacy, and transparency.
-
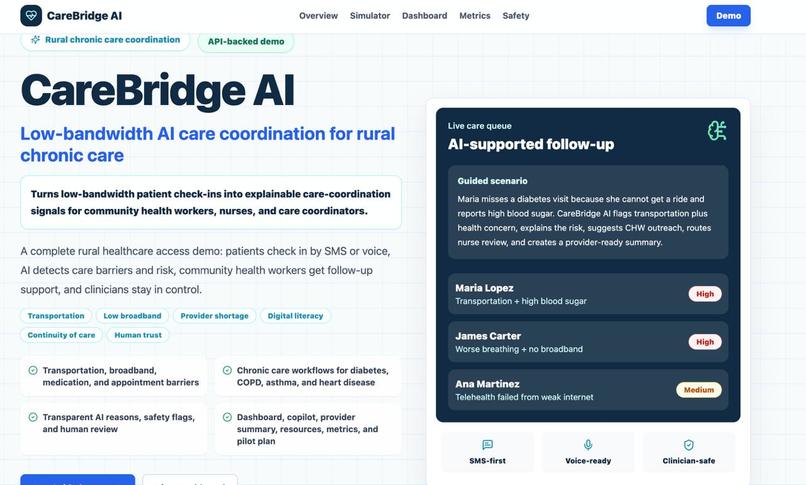
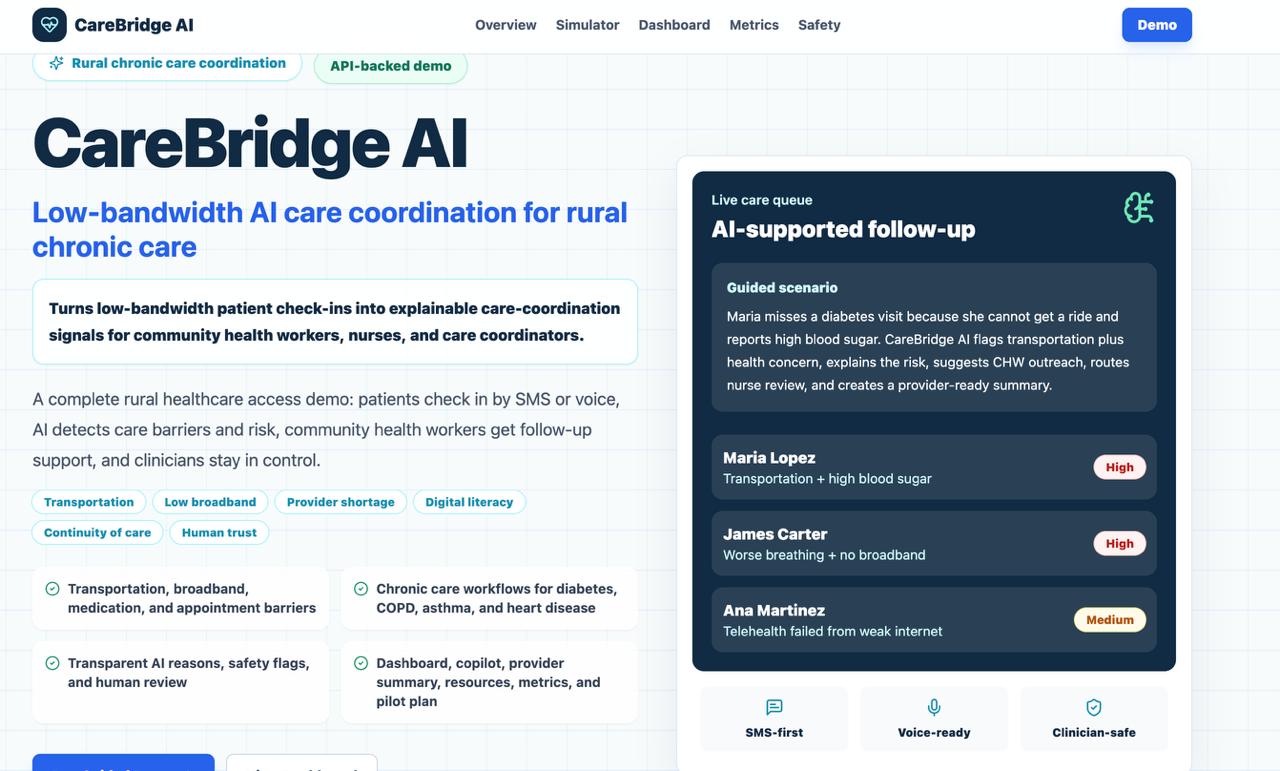
Low-bandwidth rural chronic-care coordination through SMS, voice, AI, and human follow-up.
-
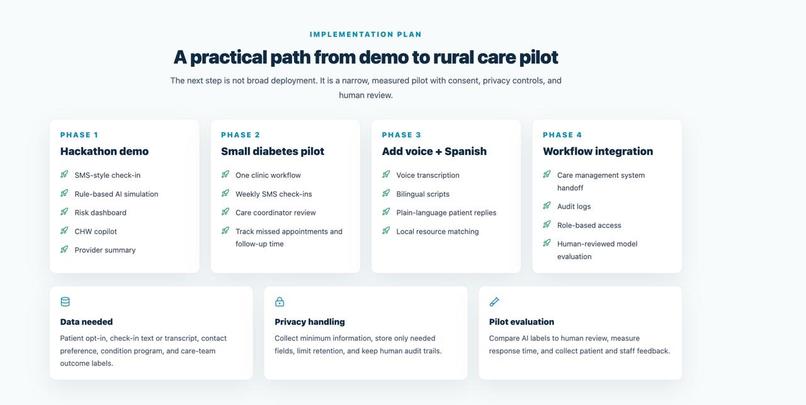
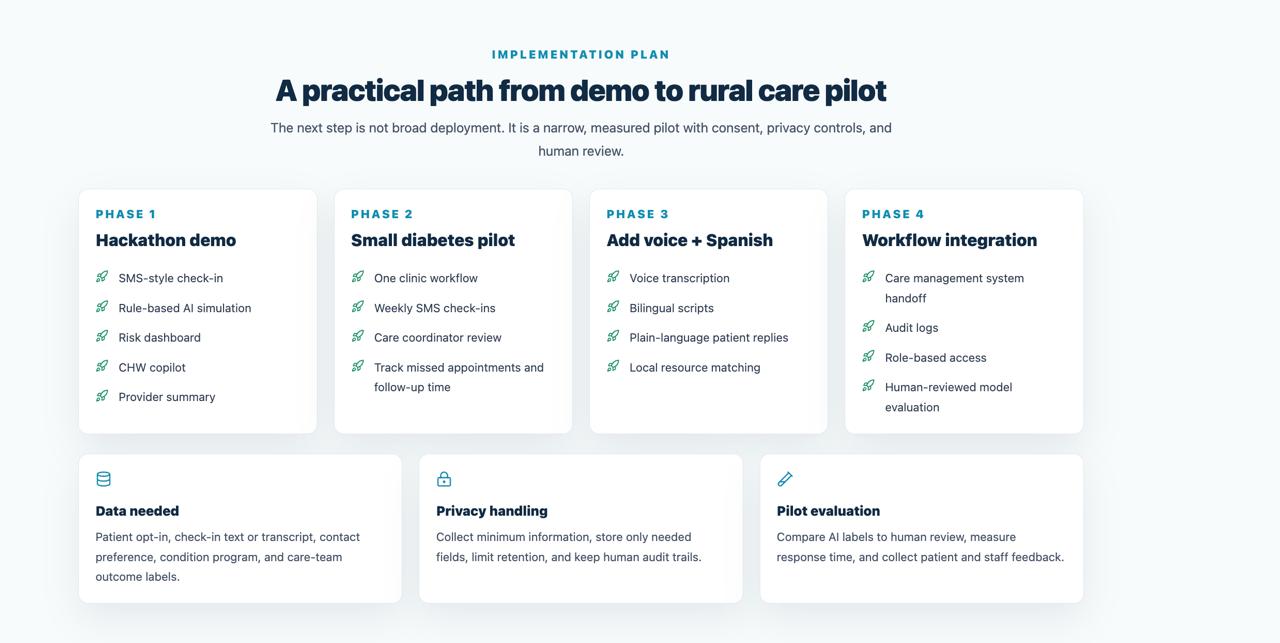
Practical path from hackathon demo to diabetes pilot, voice, Spanish, and workflow integration.
-
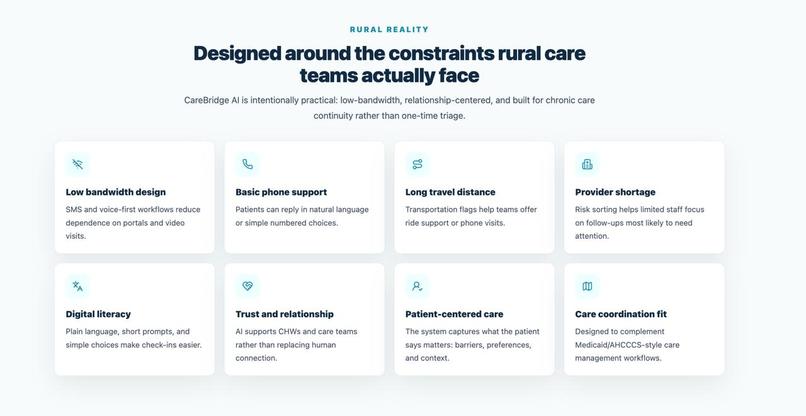
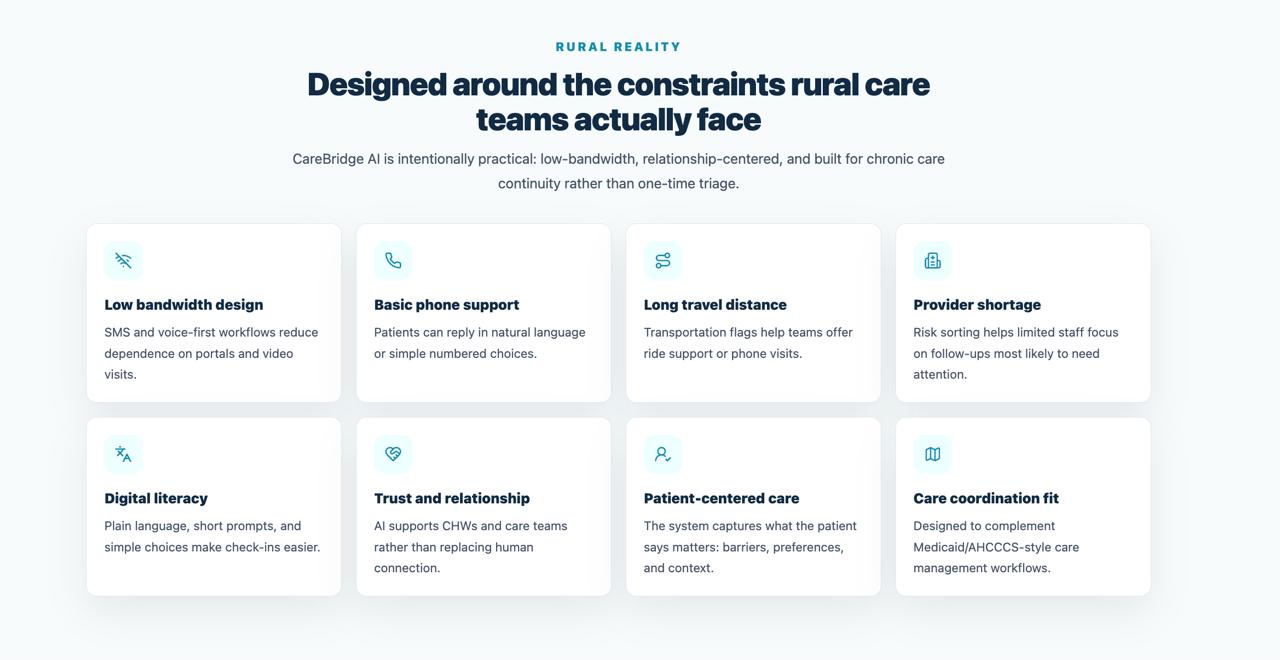
Rural reality: low bandwidth, basic phones, travel distance, trust, and provider shortage.
-
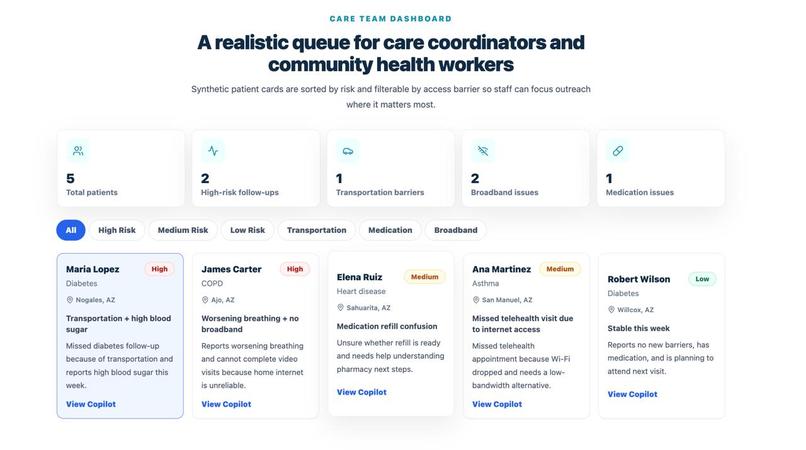
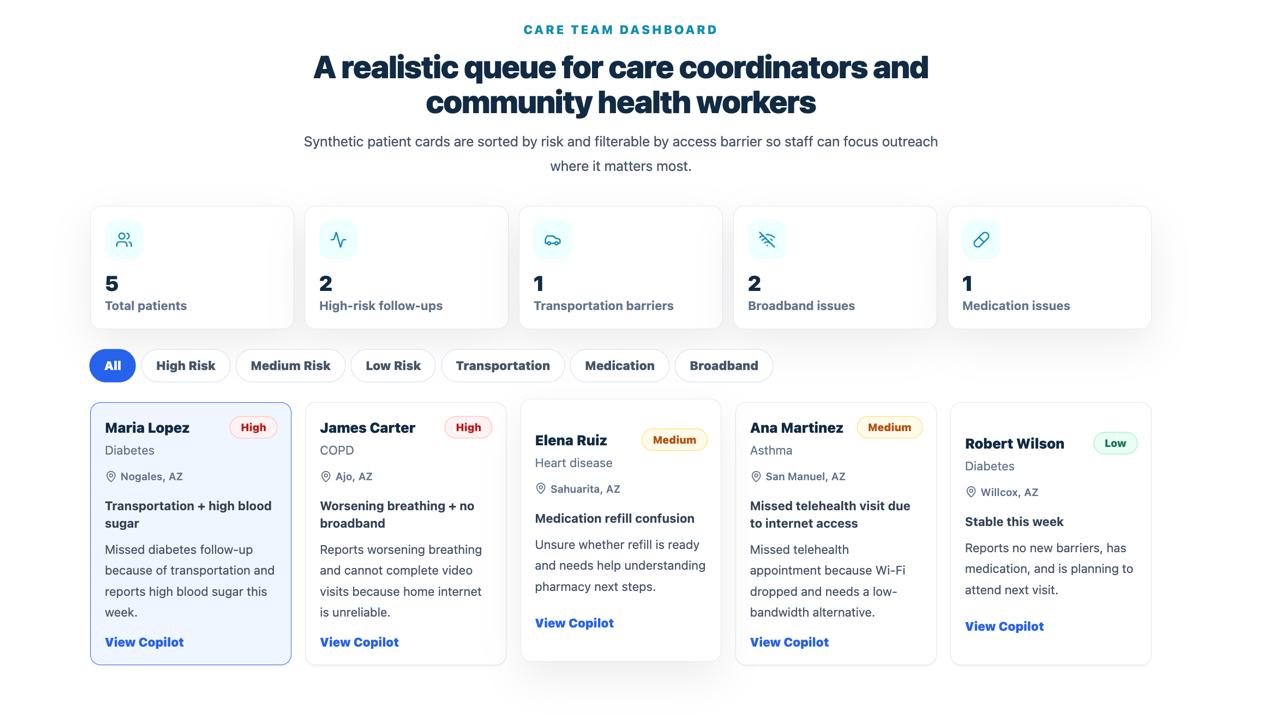
Dashboard sorts synthetic patients by risk, barrier, condition, and suggested follow-up.
-
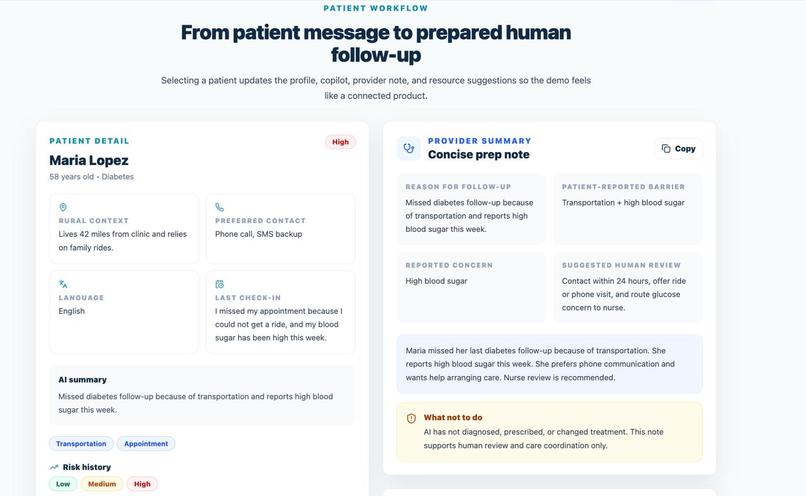
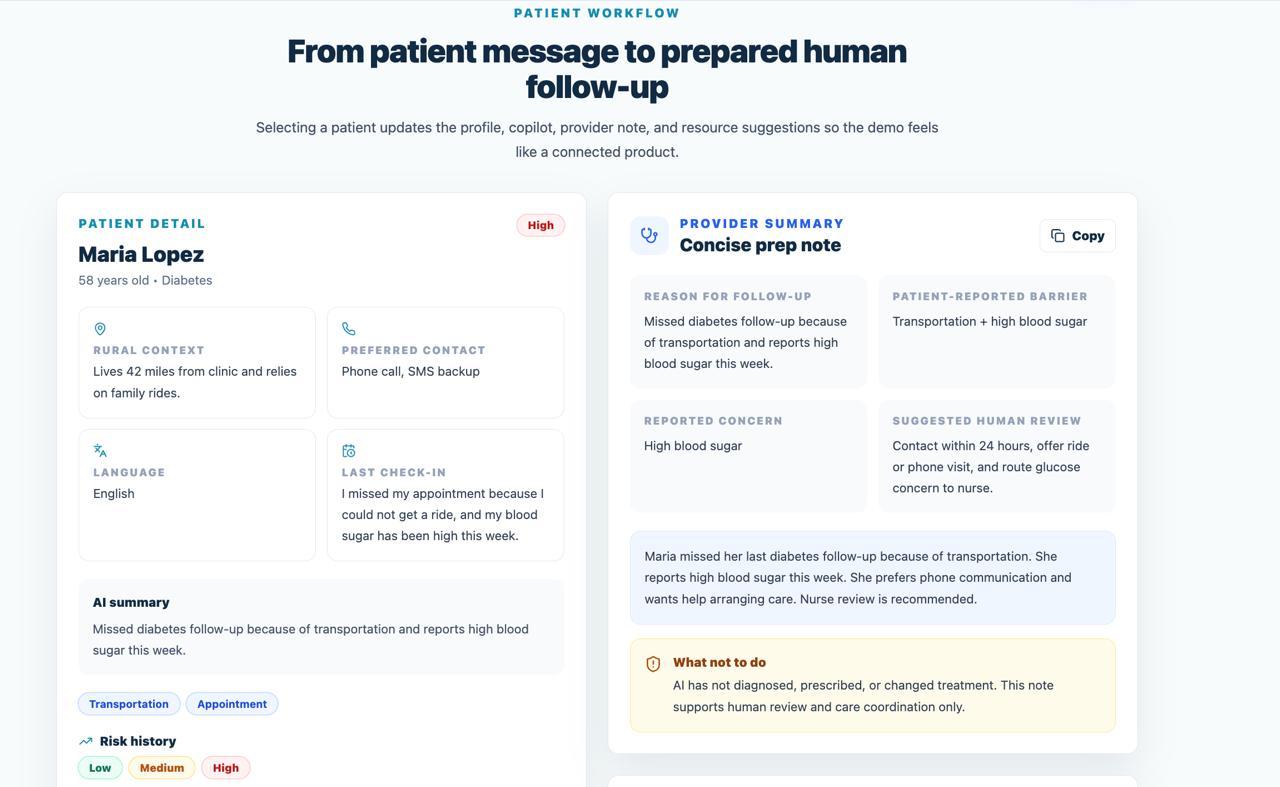
Patient workflow links context, AI summary, provider note, risk history, and safety boundaries.
-
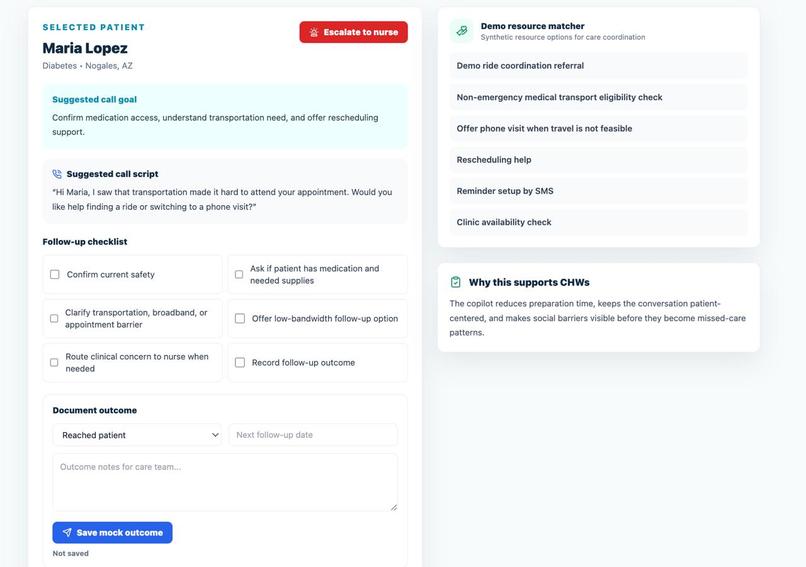
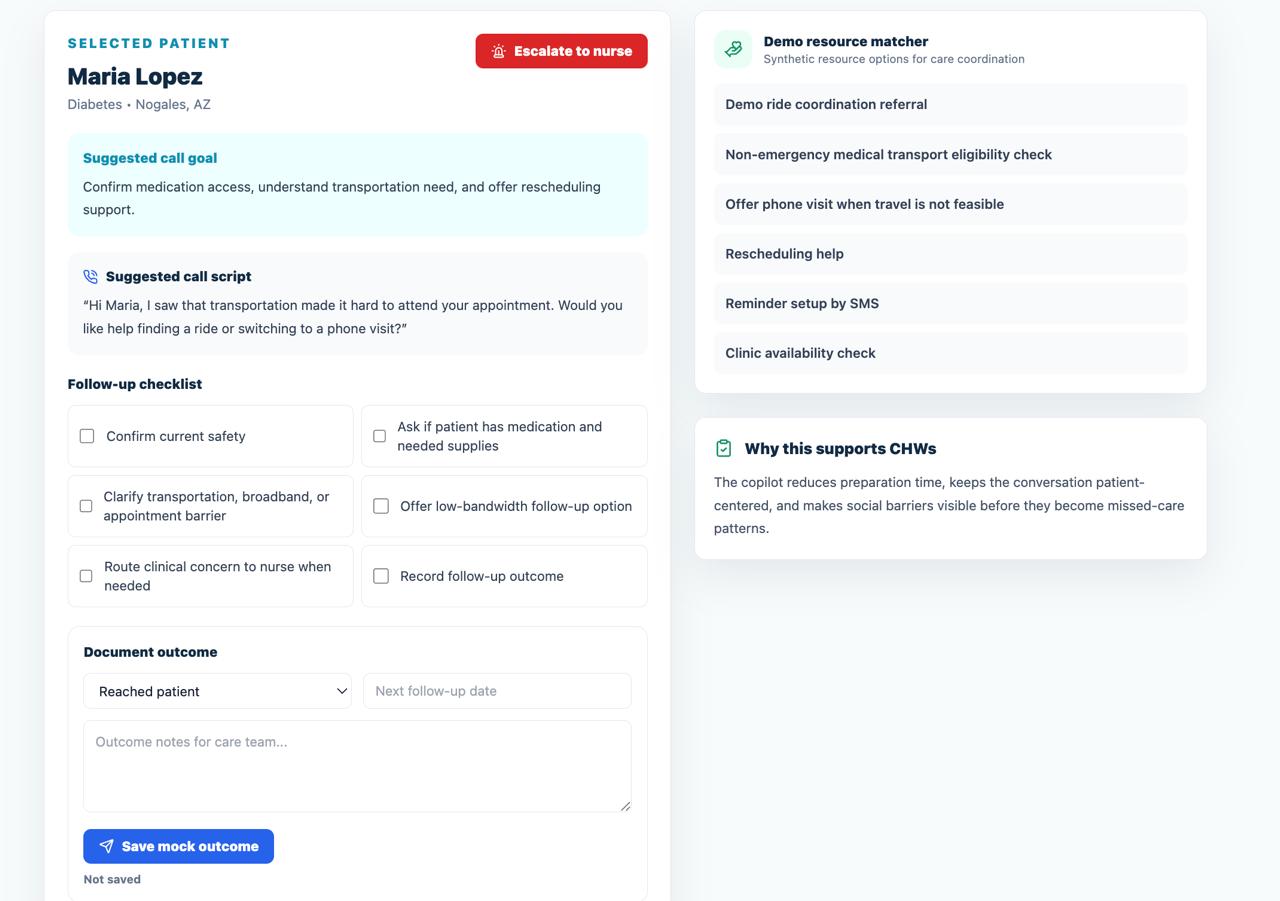
CHW copilot provides call goals, scripts, checklist, resources, and follow-up documentation.
-
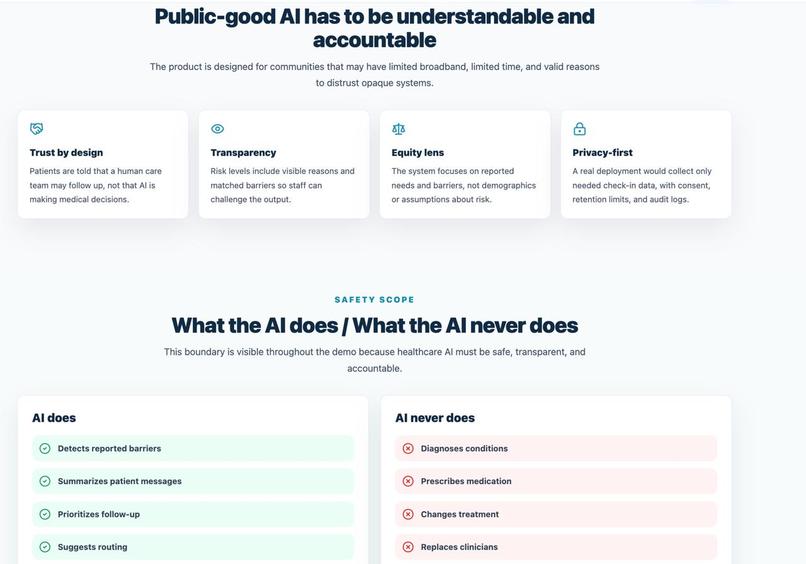
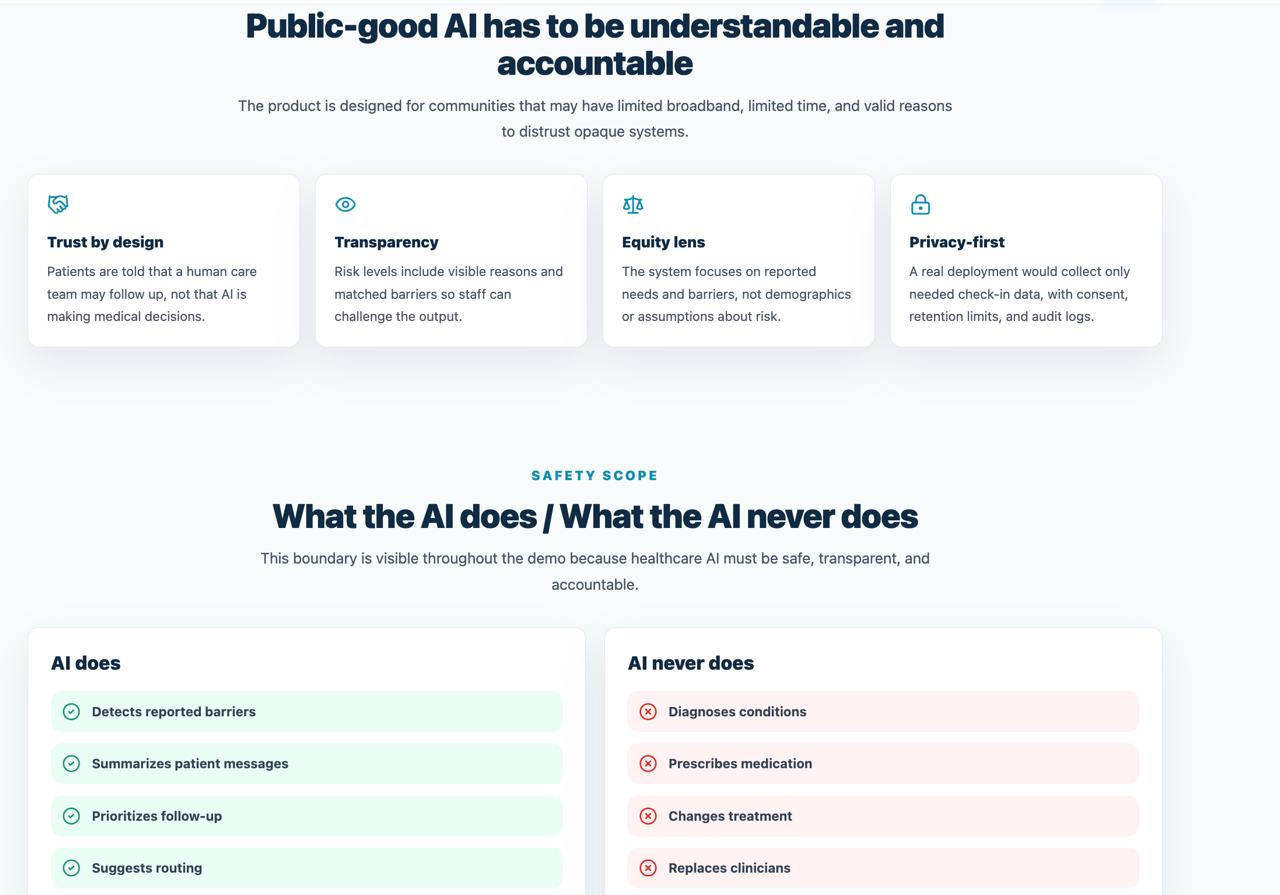
Public-good AI section showing trust, transparency, equity, privacy, and clear safety limits.
-
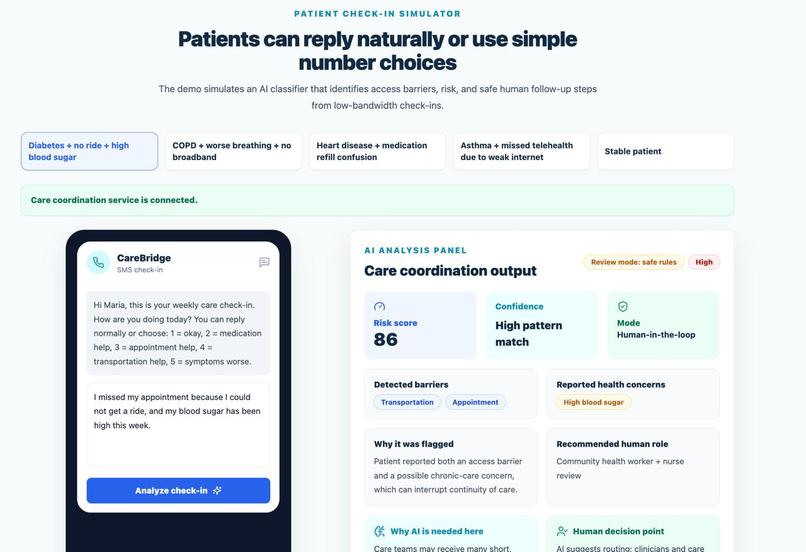
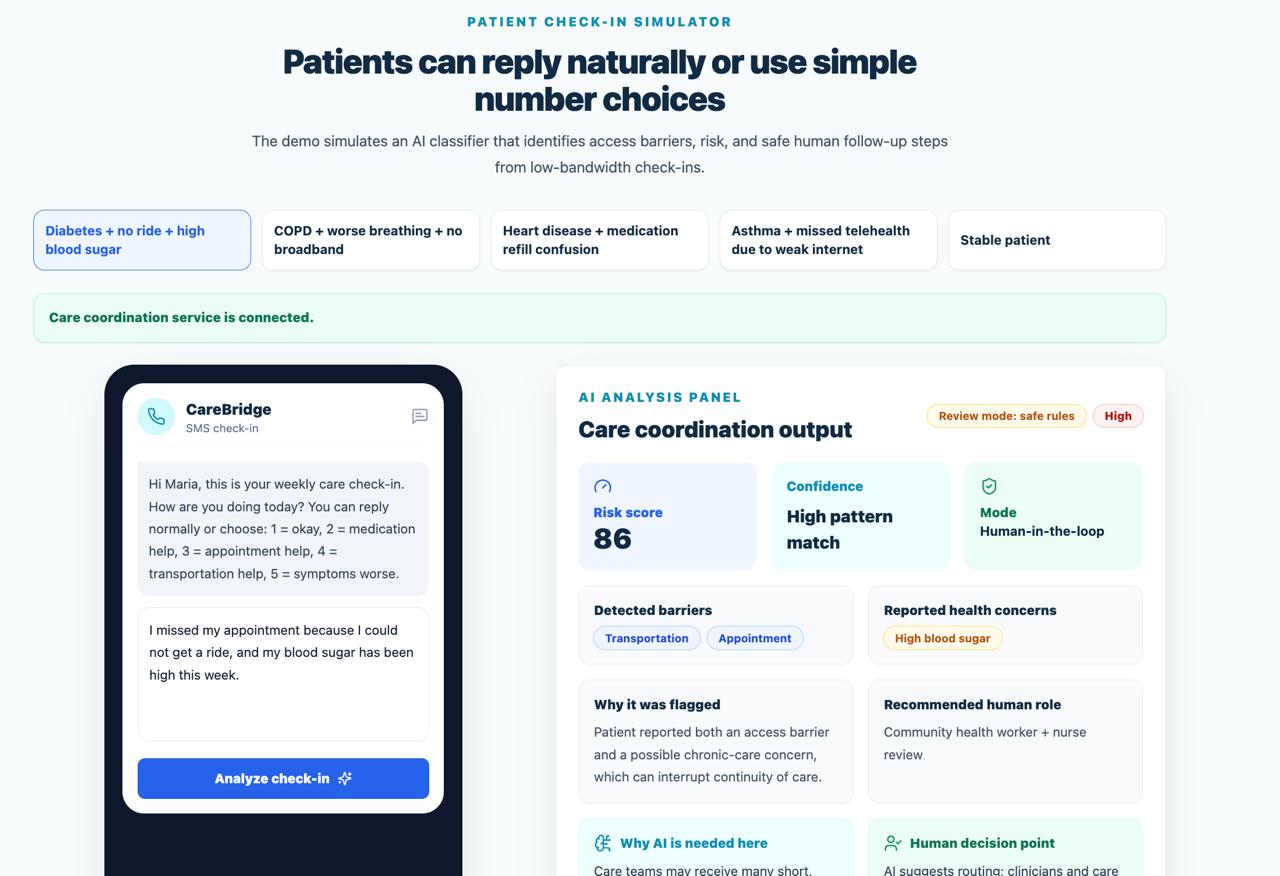
SMS-style check-in simulator turns patient messages into risk and care-coordination signals.
Inspiration
Rural patients managing chronic conditions often face barriers that are not only medical: long travel distance, unreliable transportation, weak internet, missed follow-ups, medication confusion, and limited clinic availability. These issues can quietly interrupt care before a care team knows what happened.
We built CareBridge AI to help rural care teams notice those barriers earlier and prioritize human follow-up for patients who may otherwise fall through the cracks.
What it does
CareBridge AI is a low-bandwidth care coordination system for rural chronic care. Patients can send SMS-style or voice check-ins about problems like missed appointments, transportation needs, medication confusion, weak broadband, or worsening symptoms.
The system analyzes the message, detects reported barriers, assigns a risk level, explains why it was flagged, and creates a care-team summary. Community health workers, nurses, and care coordinators can then use the dashboard, copilot view, provider summary, and nurse escalation workflow to follow up with the right patient sooner.
CareBridge AI does not diagnose, prescribe, change treatment, or replace clinicians. It supports care coordination and human review.
How we built it
We built the frontend with React, Vite, and Tailwind CSS. The app includes an SMS check-in simulator, AI analysis panel, risk dashboard, community health worker copilot, provider summary, resource matcher, safety guardrails, and pilot metrics.
We also added a lightweight Node.js and Express backend. The backend includes API endpoints for check-ins, analysis, synthetic patients, follow-up outcomes, metrics, SMS webhook simulation, and nurse escalation. Check-in messages and follow-up records are stored in a local SQLite database.
For AI analysis, CareBridge AI can use an optional OpenAI-compatible API if an API key is configured. If no key is available, it automatically falls back to deterministic rule-based analysis so the demo remains safe and reproducible.
Challenges
The biggest challenge was making the AI useful without making it unsafe. In healthcare, it would be risky to build a system that gives medical advice or pretends to replace clinicians. We designed CareBridge AI around a strict boundary: the AI only detects reported barriers, summarizes patient needs, explains risk, and routes cases to humans.
Another challenge was making the workflow realistic for rural communities. We focused on SMS, voice-style check-ins, weak broadband, transportation barriers, low digital literacy, and limited staff time instead of assuming every patient can use a full app or video visit.
Accomplishments
We created a working API-backed prototype that shows the full care coordination flow: patient check-in, AI analysis, risk prioritization, community health worker support, provider summary, resource suggestions, follow-up documentation, and nurse escalation.
We are proud that CareBridge AI uses AI in a practical public-good role. It does not try to automate medicine. It helps human care teams organize signals, identify access barriers earlier, and prepare safer follow-up.
What we learned
We learned that rural healthcare access is about more than clinic visits. Communication, transportation, internet access, trust, medication access, and follow-up workflows all affect whether chronic care continues.
We also learned that explainability matters. A risk score is not enough. Care teams need to know what the patient said, what barrier was detected, why a case was flagged, and what human role should review it.
What's next
Next, we would like to add real SMS integration, voice transcription, Spanish-language support, local resource matching, audit logs, and role-based access. We would also like to pilot the workflow with one chronic condition, such as diabetes, and measure proposed outcomes like missed appointment reduction, follow-up response time, patient check-in response rate, and staff triage time saved.
Built With
- ai
- api
- express.js
- healthcare
- javascript
- lucide-react
- node.js
- openai-api
- react
- rule-based-ai
- sms
- sqlite
- tailwind-css
- vite

Log in or sign up for Devpost to join the conversation.