-
-

BridgeHealth AI
-
-
-
-

-
-

-



What Inspired Me
I remember watching the news during COVID-19 and feeling completely helpless.
Families in rural villages — in India, in the Philippines, in Indonesia — were losing their mothers, their fathers, their grandparents. Not always because medicine didn't exist. Not always because doctors didn't know what to do. But because nobody told them it was an emergency in time.
A grandmother with chest pain thought it was indigestion. A father with shortness of breath waited three days before anyone said the word hospital. A young mother didn't know who to call, couldn't read the English pamphlet, and lived four hours from the nearest clinic.
That broke my heart.
I am not from a technical background. I had never built an app before. I had never entered a hackathon before. But I kept asking myself one question I couldn't let go of:
What if there was something — anything — that could have told that grandmother, in her own language, in 30 seconds: "This is an emergency. Call for help right now."
That question became BridgeHealth AI.
What I Built
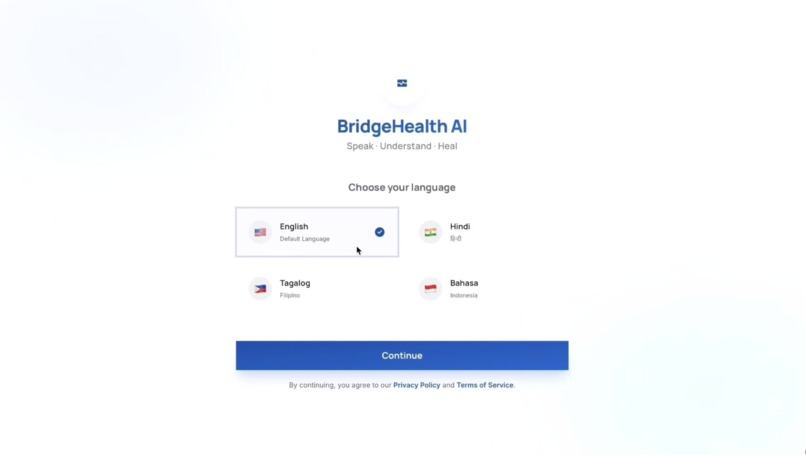
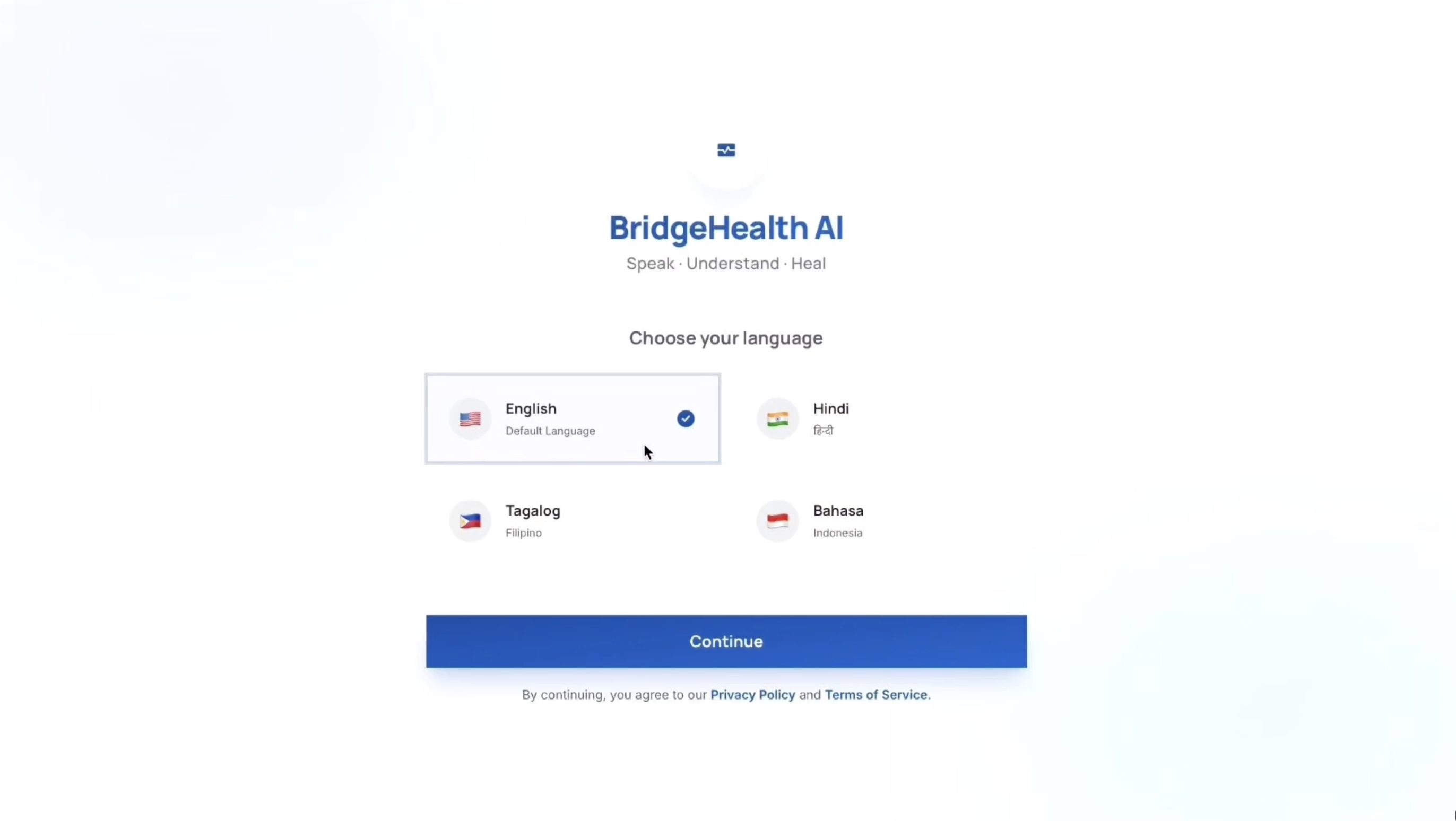
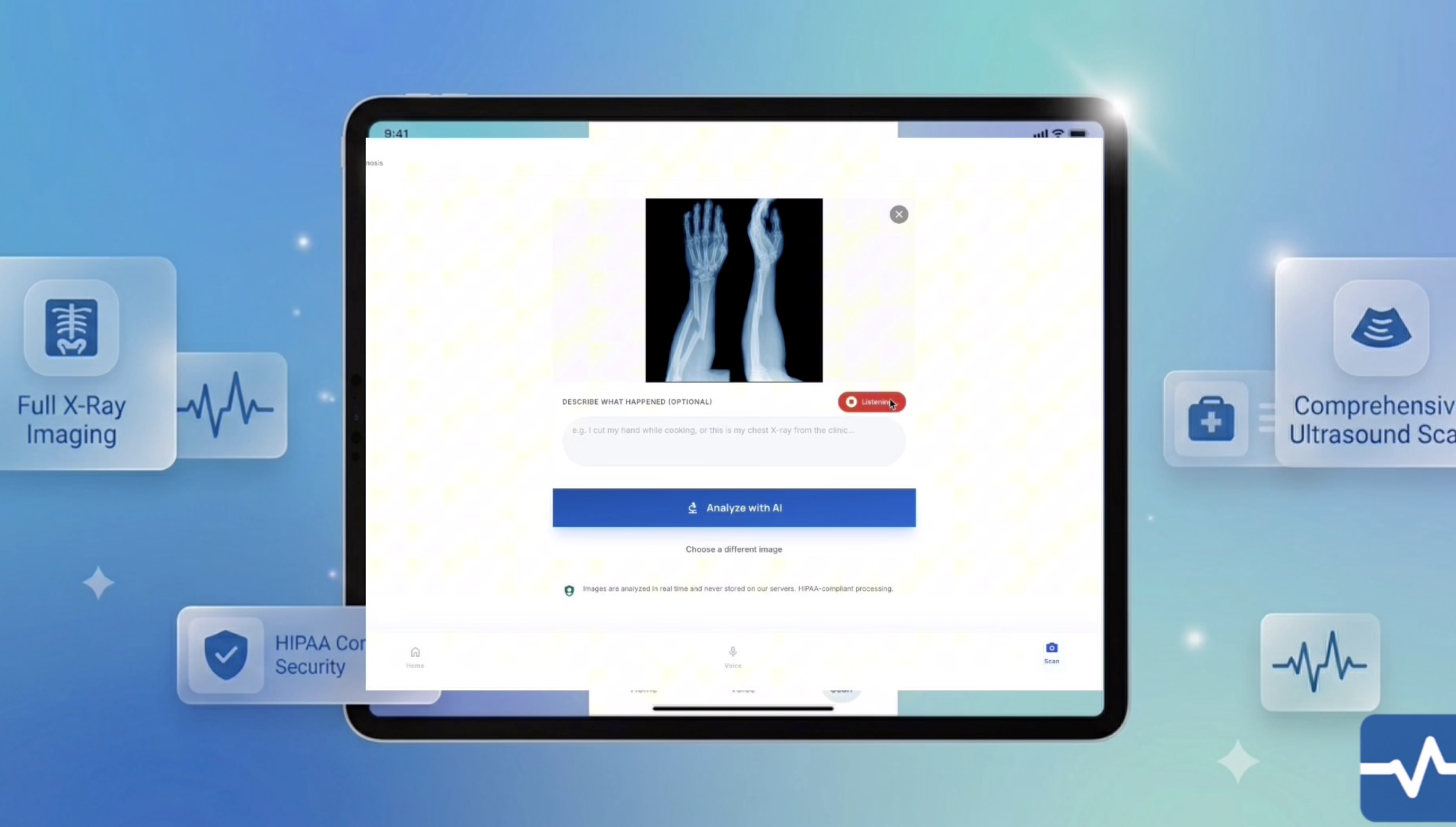
BridgeHealth AI is a voice-first, multilingual AI healthcare assistant designed for patients in rural India, Philippines, and Indonesia who have no reliable access to doctors, speak little or no English, and cannot afford to wait.
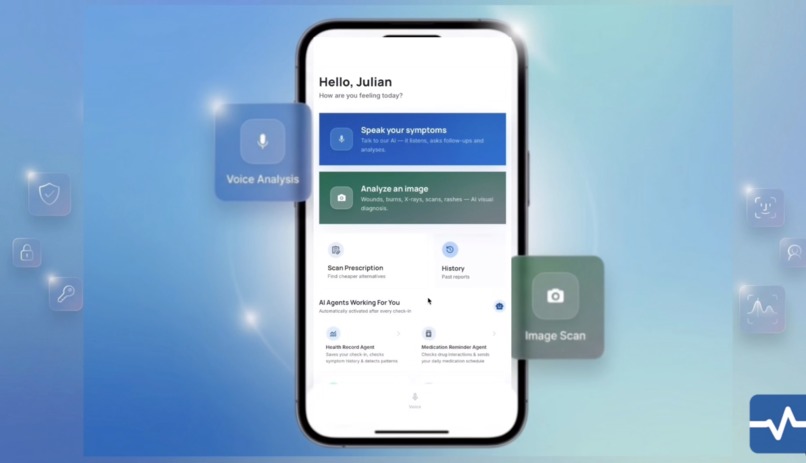
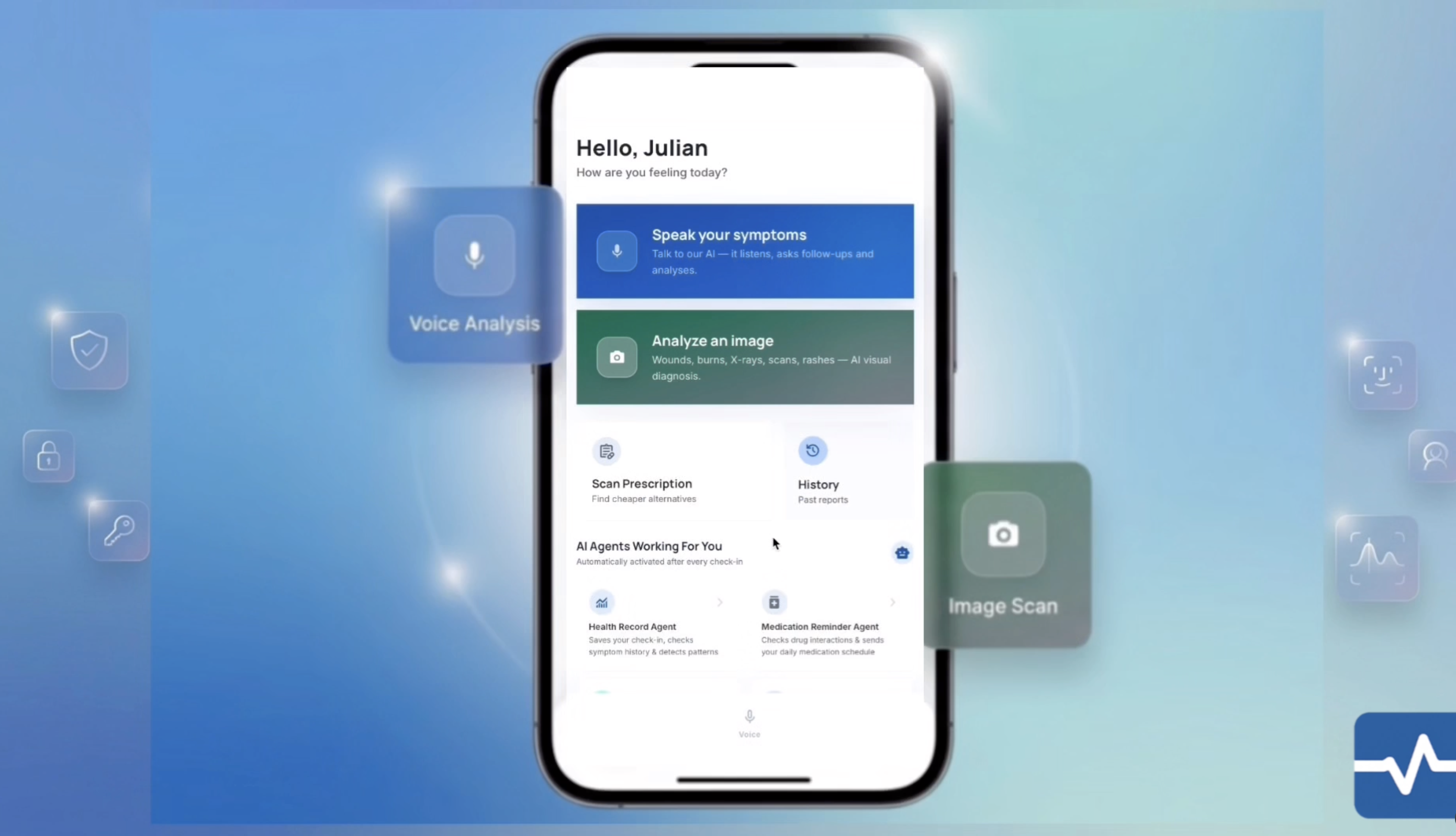
A patient speaks their symptoms out loud — in Hindi, Tagalog, Bahasa Indonesia, or English. The AI listens, asks structured clinical follow-up questions, triages the severity in real time, and within 30 seconds delivers:
- A severity classification — EMERGENCY, SEE DOCTOR, or HOME CARE
- A personalised care plan spoken aloud in their language
- An automatic WhatsApp alert to their caregiver — with zero taps
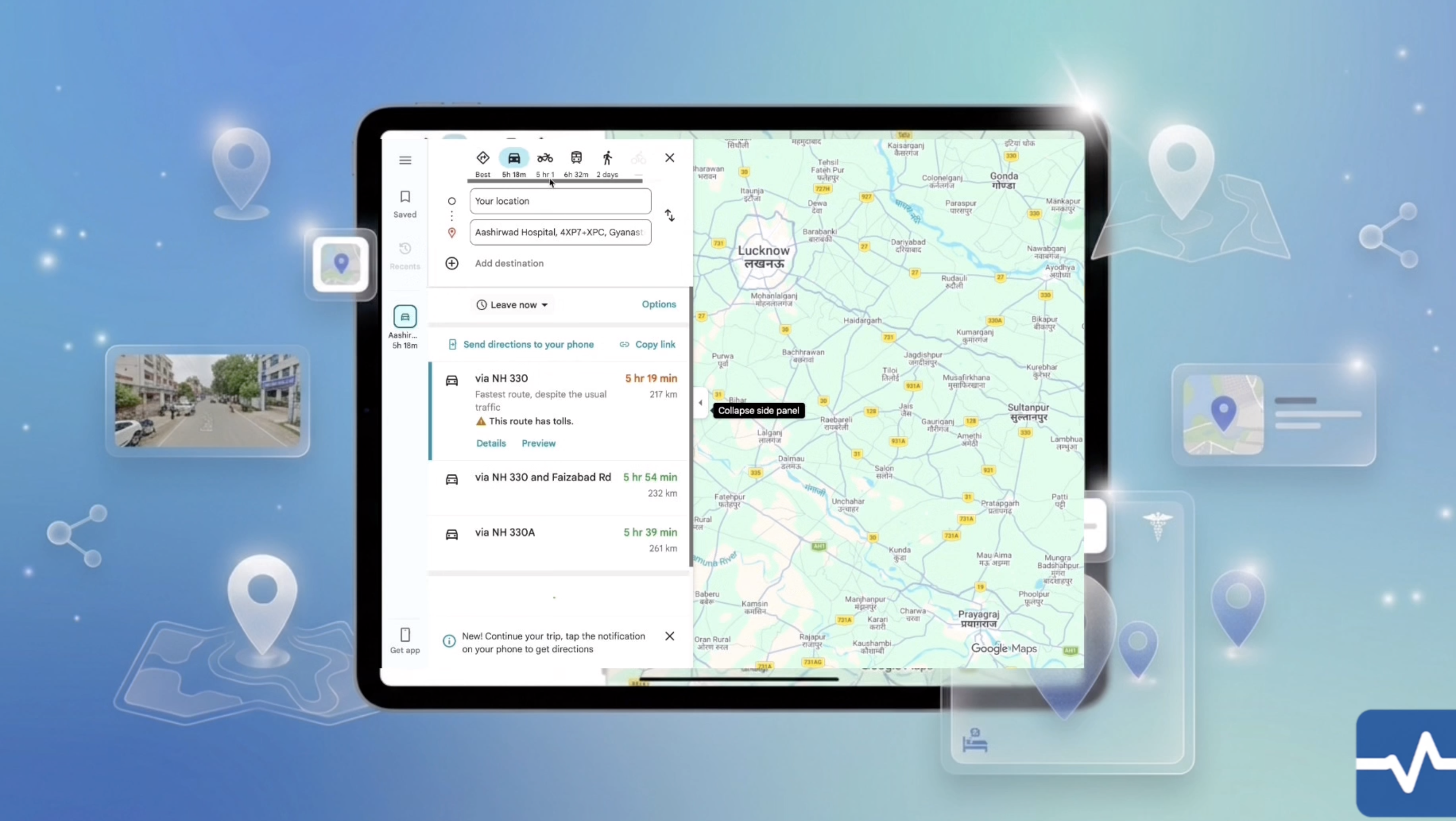
- A list of nearby hospitals with exact distances
- A 7-day recovery plan, medicine price comparisons, and a doctor visit prep document
Everything. In their language. Without typing a single word.
How I Built It
I built this entirely alone, as my first ever technical project, over several weeks of learning and iteration.
The core AI triage engine uses Groq's LLaMA 3.1 8B Instant model — chosen for its speed and generous free tier. If Groq ever fails, the system automatically falls back to Featherless AI using the same model architecture via an OpenAI-compatible endpoint, so the app never goes dark for a patient who needs it.
The clinical conversation follows the SAMPLE framework — the same structured symptom collection method used by paramedics worldwide:
$$ \text{SAMPLE} = \text{Symptoms} + \text{Allergies} + \text{Medications} + \text{Past History} + \text{Last Meal} + \text{Events} $$
The medical triage prompt was designed with one hard rule above all others:
When in doubt — always escalate. These patients may be far from hospitals. Being cautious saves lives.
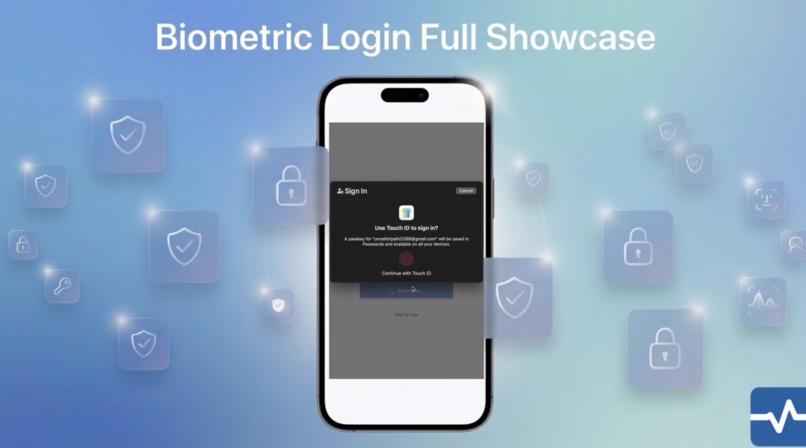
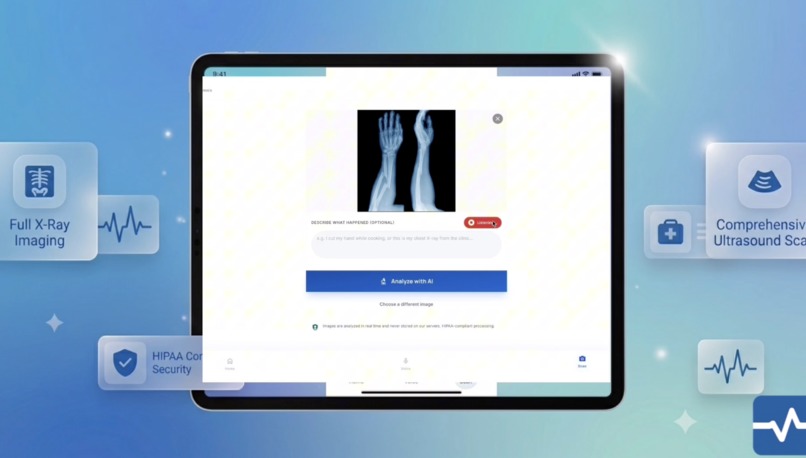
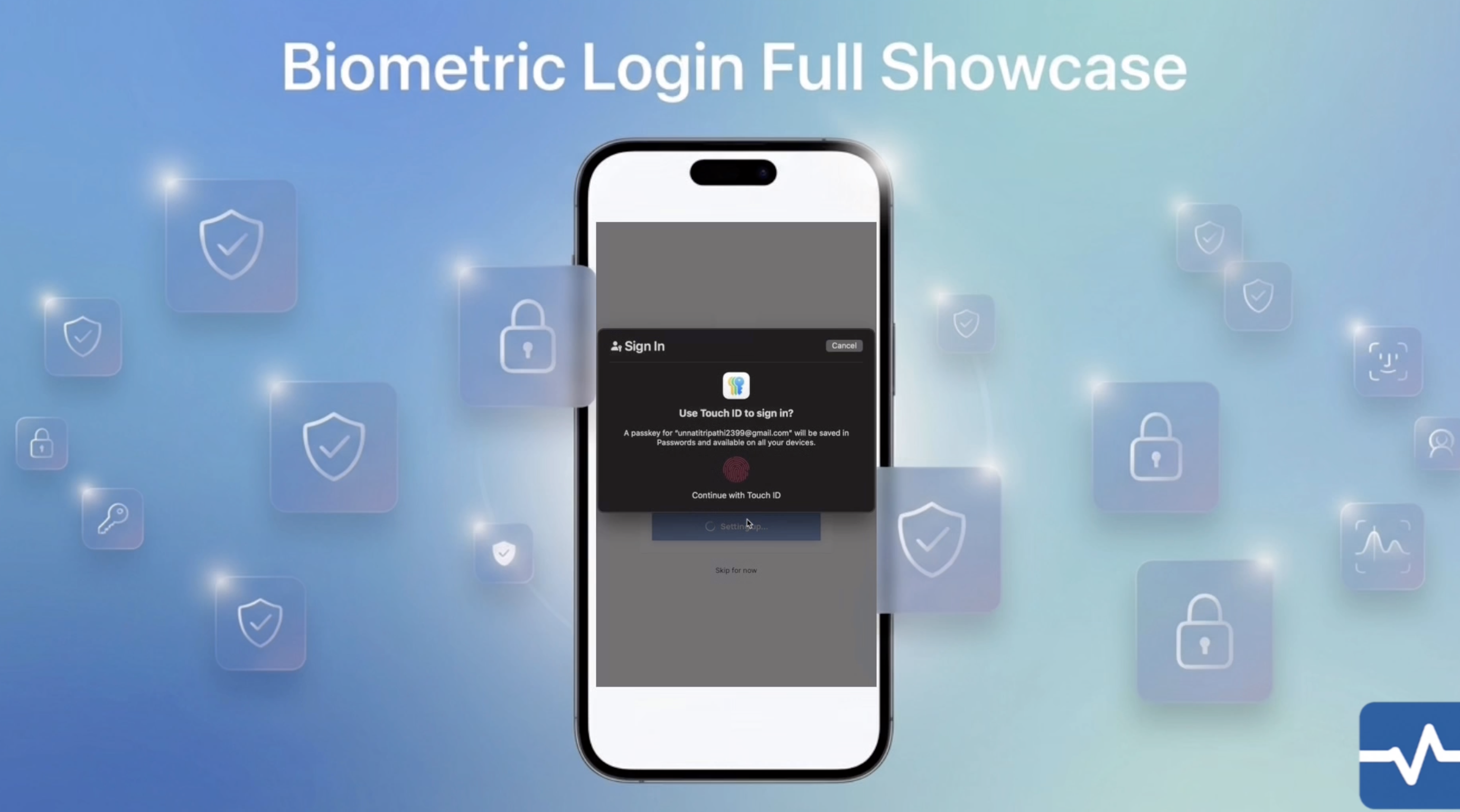
Anthropic Claude handles agent orchestration — executing 6 parallel background tasks the moment a triage completes. Google Gemini 2.5 Flash powers the prescription scanner and image diagnosis. WebAuthn FIDO2 provides biometric login so users never have to remember a password. Resend delivers 24-hour follow-up emails to both patient and caregiver automatically.
The entire frontend is built in Next.js 14 with TypeScript and Tailwind CSS — my first time using any of these technologies.
What I Learned
I learned that the hardest problems to solve are not always the most technically complex ones.
The hardest problem I solved was not the AI integration. It was asking: how do you design an app for someone who has never used a smartphone health app, cannot type, cannot read English, and is frightened?
The answer was: you make it speak to them.
I learned about the Web Speech API, text-to-speech in four languages, real-time transcription, and how to build a conversation that never asks someone to read anything. I learned about WebAuthn and why removing passwords matters more for rural users than anyone else.
I learned about the Haversine formula for calculating GPS distances to hospitals. For two points on Earth with coordinates \( (\phi_1, \lambda_1) \) and \( (\phi_2, \lambda_2) \), the great-circle distance is:
$$ d = 2r \arcsin\left(\sqrt{\sin^2!\left(\frac{\Delta\phi}{2}\right)
- \cos\phi_1 \cdot \cos\phi_2 \cdot \sin^2!\left(\frac{\Delta\lambda}{2}\right)}\right) $$
where \( r = 6{,}371 \text{ km} \) is the mean radius of the Earth, \( \Delta\phi \) is the difference in latitude, and \( \Delta\lambda \) is the difference in longitude.
I learned that quota errors and failed API calls at 2am are part of the process. I learned to keep going.
Most of all, I learned that technology is only as meaningful as the person it reaches.
The Challenges I Faced
This was my first hackathon. I come from a non-technical background.
Every single piece of this project required me to learn something I had never done before. There were moments I genuinely did not know if I could finish.
The biggest technical challenge was AI provider reliability. I went through four different AI providers — Gemini, Anthropic, HuggingFace, and finally Groq — because free tier quotas kept running out mid-build. Each time one failed, I had to understand why, find an alternative, and rewire the system. That is why BridgeHealth AI now has dual AI providers with automatic failover — not by design originally, but born from necessity.
The hardest design challenge was medical accuracy. An early version of the app returned HOME CARE for almost every symptom — because that was the statistically "safe" default. But for a rural patient with undiagnosed chest pain, HOME CARE is not safe. It could be fatal. I rewrote the entire triage logic from scratch:
- Chest pain → always EMERGENCY, no exceptions
- Any new symptom → minimum SEE DOCTOR
- HOME CARE → only when patient explicitly confirms prior prescription and stable symptoms
The emotional challenge was the hardest of all.
Every time I got frustrated, every time something broke, I thought about that grandmother who didn't know it was an emergency. And I kept building.
Why It Matters by 2030
The United Nations SDG 3.8 calls for universal health coverage by 2030. There are over 500 million people in rural South and Southeast Asia who currently have no reliable access to primary healthcare.
BridgeHealth AI cannot replace a doctor. But it can be the voice that says "this is serious, go now" — in Hindi, in Tagalog, in Bahasa — at 3am, in a village four hours from the nearest hospital.
That voice could save a life.
That is why I built this.
Built With
- agenticai
- deep-learning
- docker
- fast-api
- javascript
- llm
- machine-learning
- python



Log in or sign up for Devpost to join the conversation.