-
-
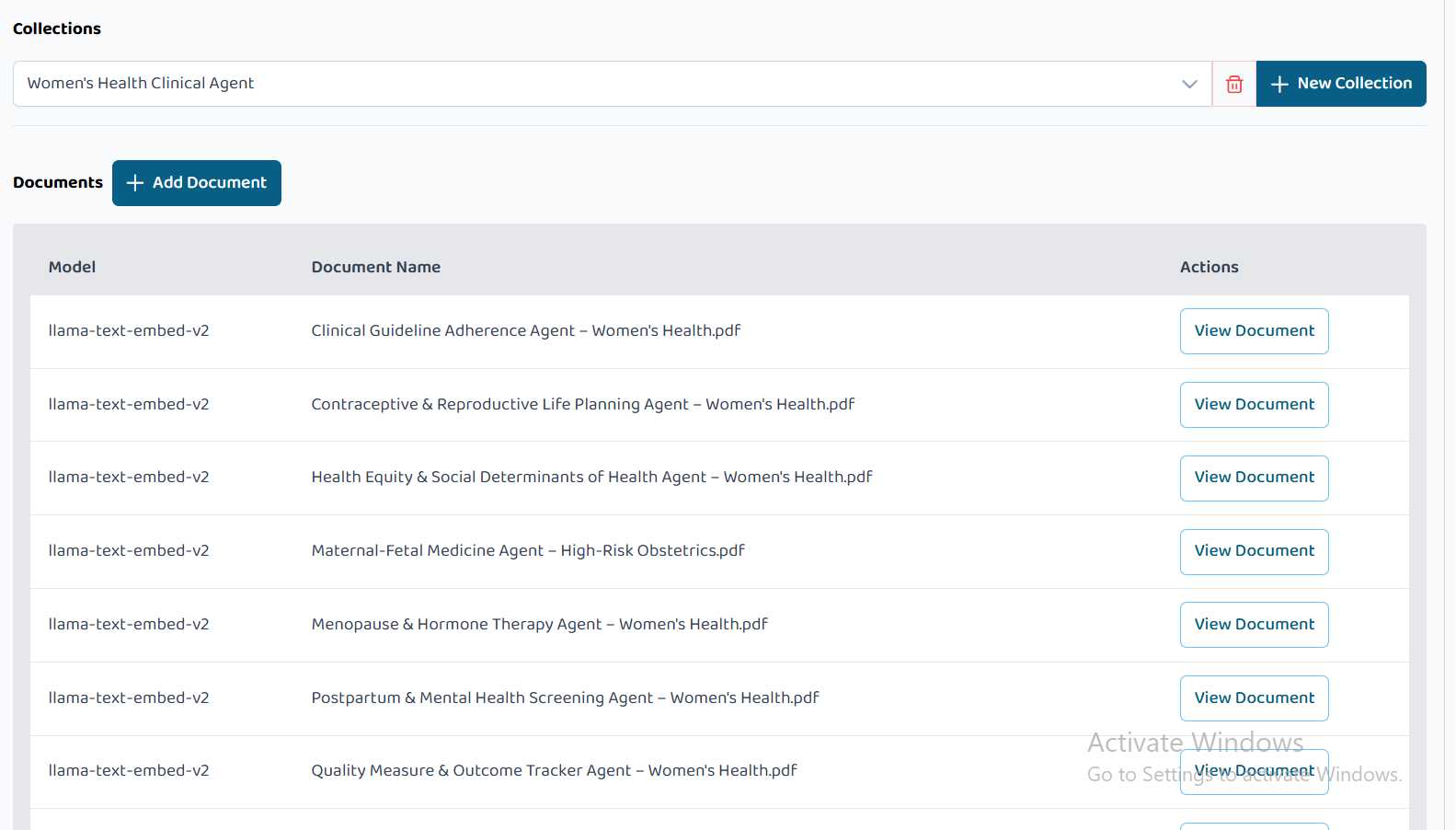
Knowledge Base Collection Powering WHCA
-

Project Cover Image
-
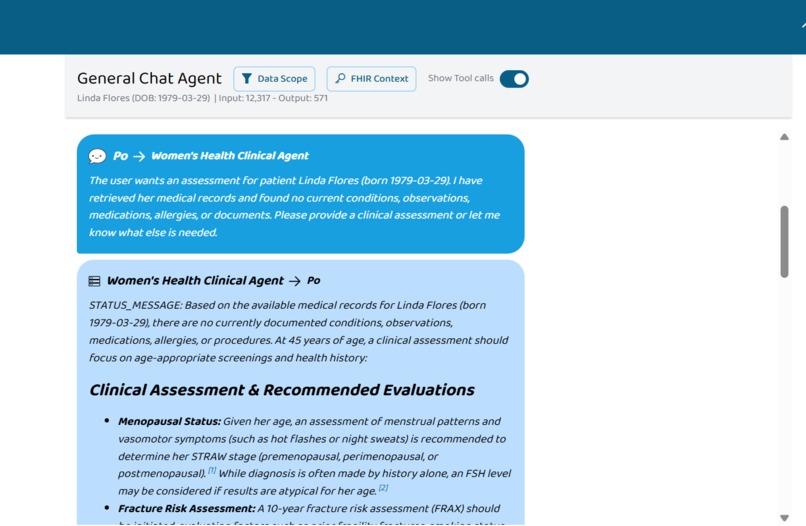
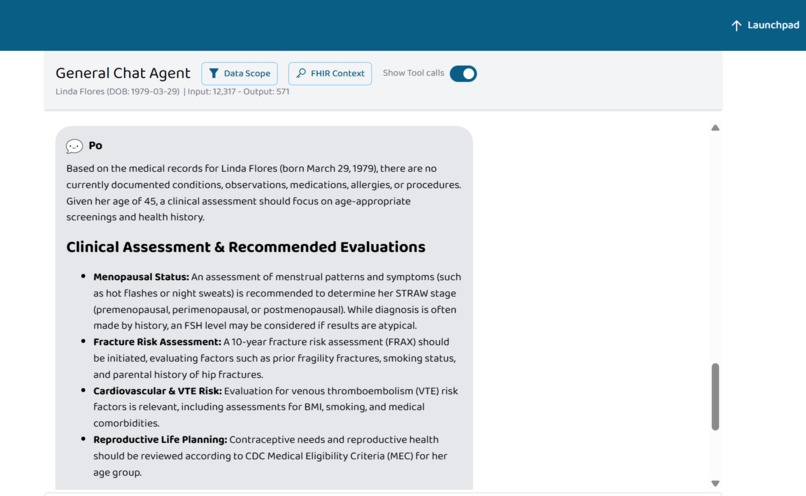
(1/4) Image Showing WHCA providing Clinical Assessment and Recommendation
-
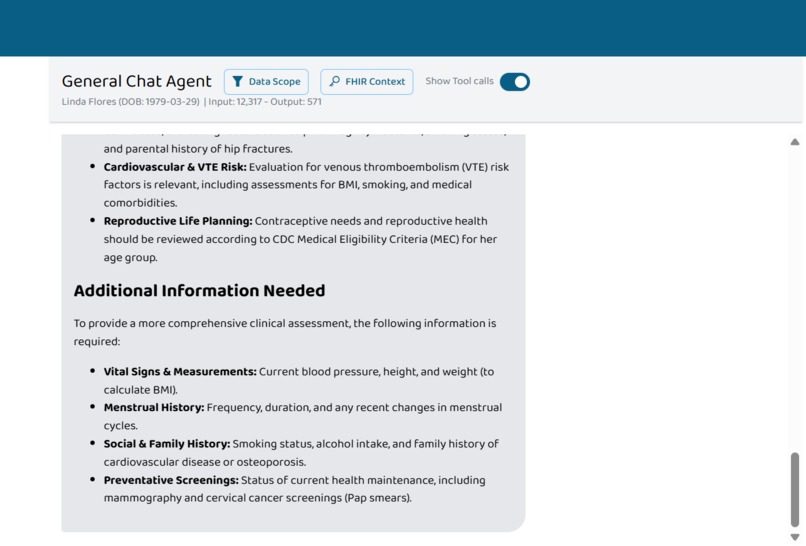
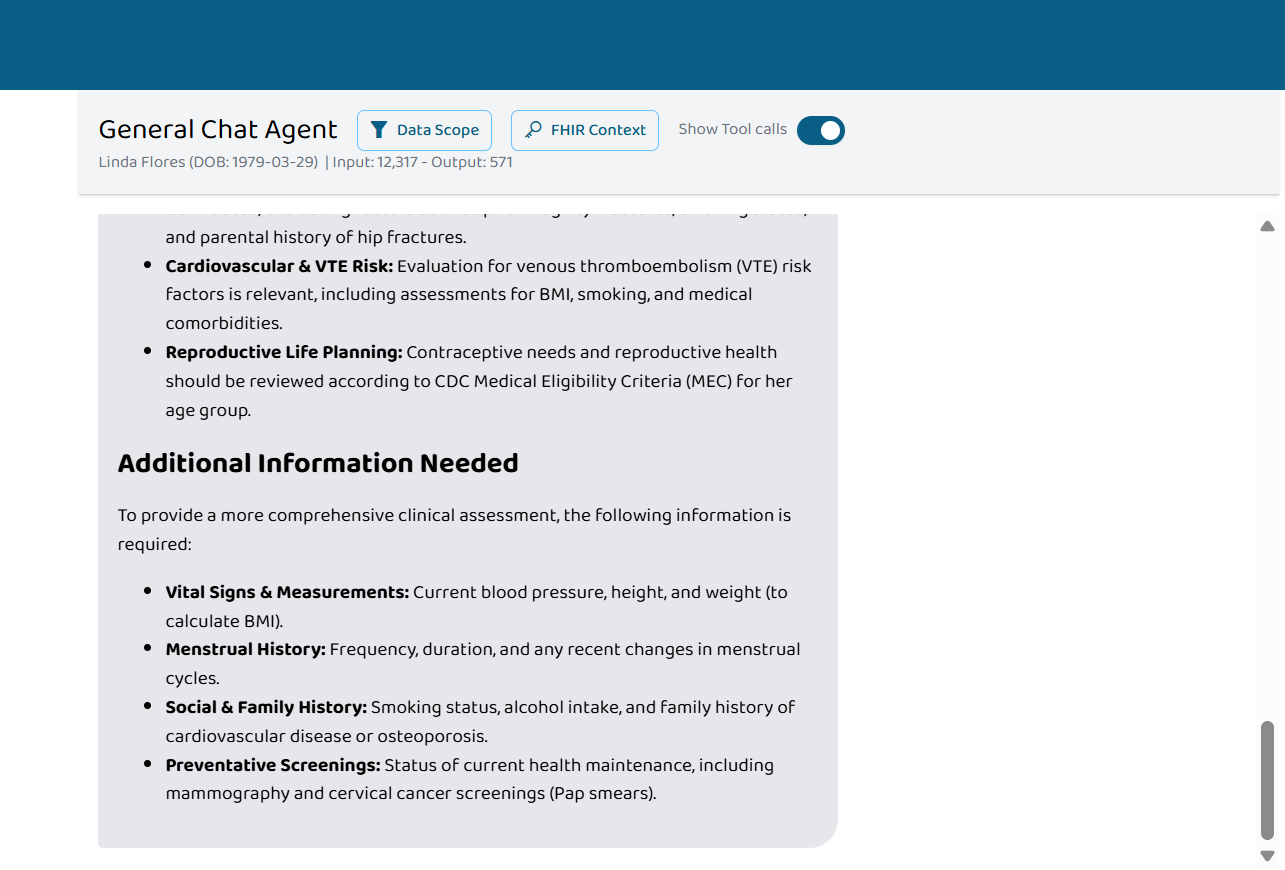
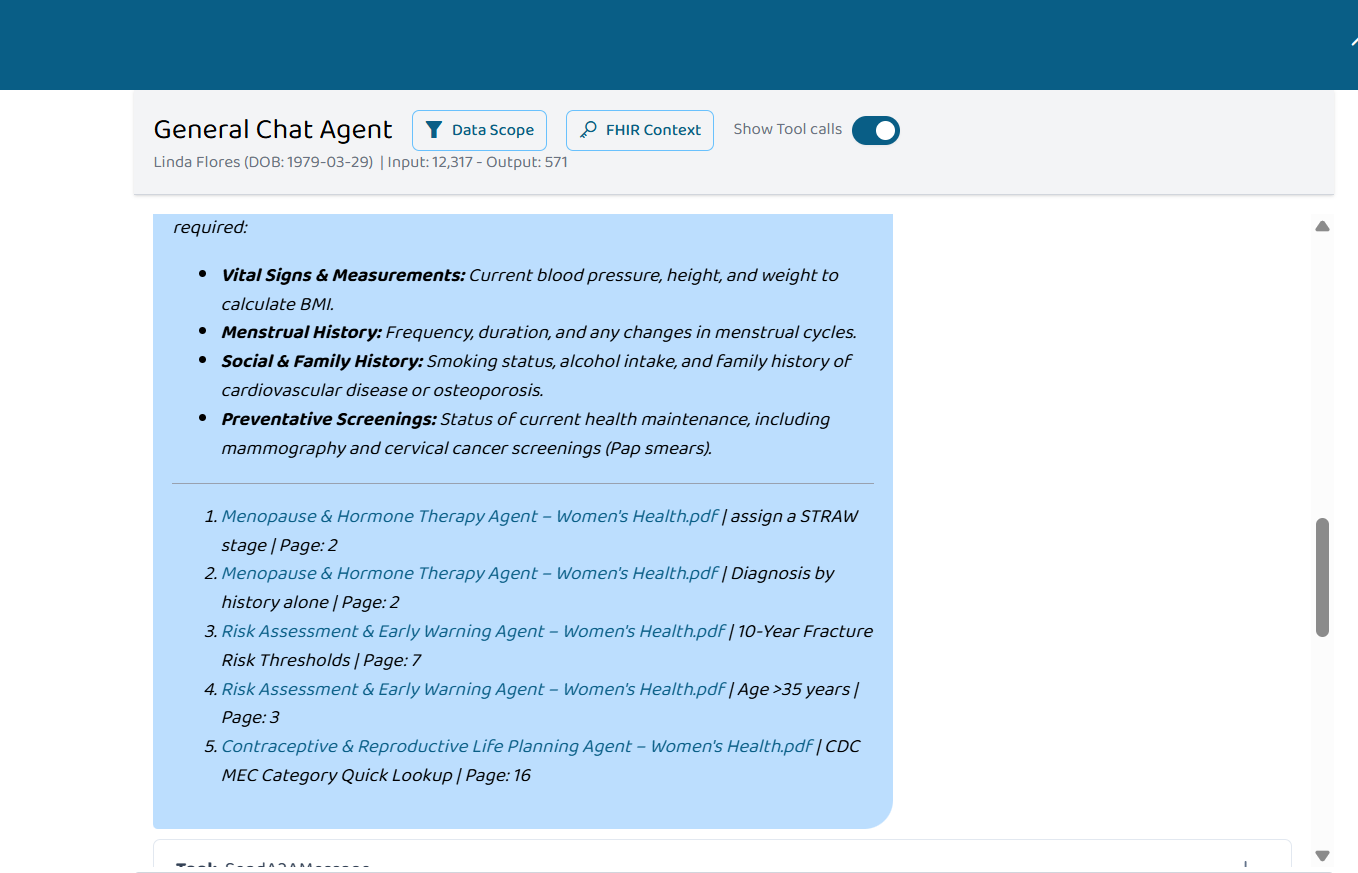
(4/4) Image Showing List of Missing Information Needed For Best Assessment to the Clinician
-
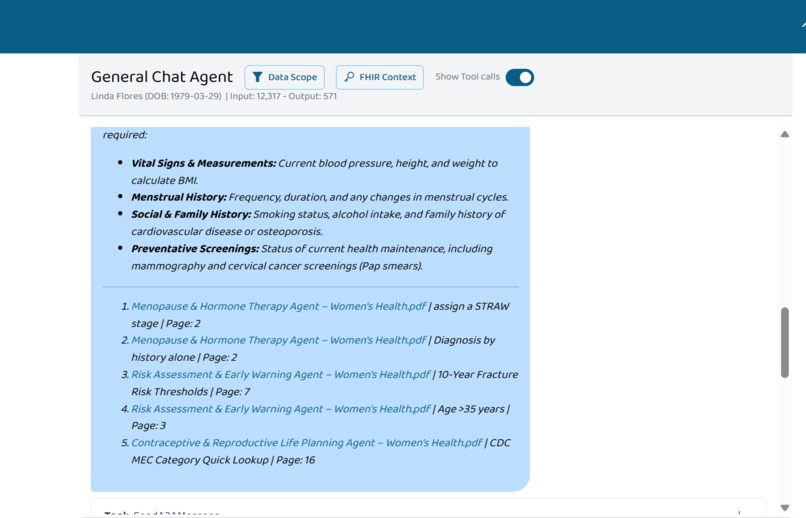
(2/4) Image Showing Cited Sources For WHCA Response
-
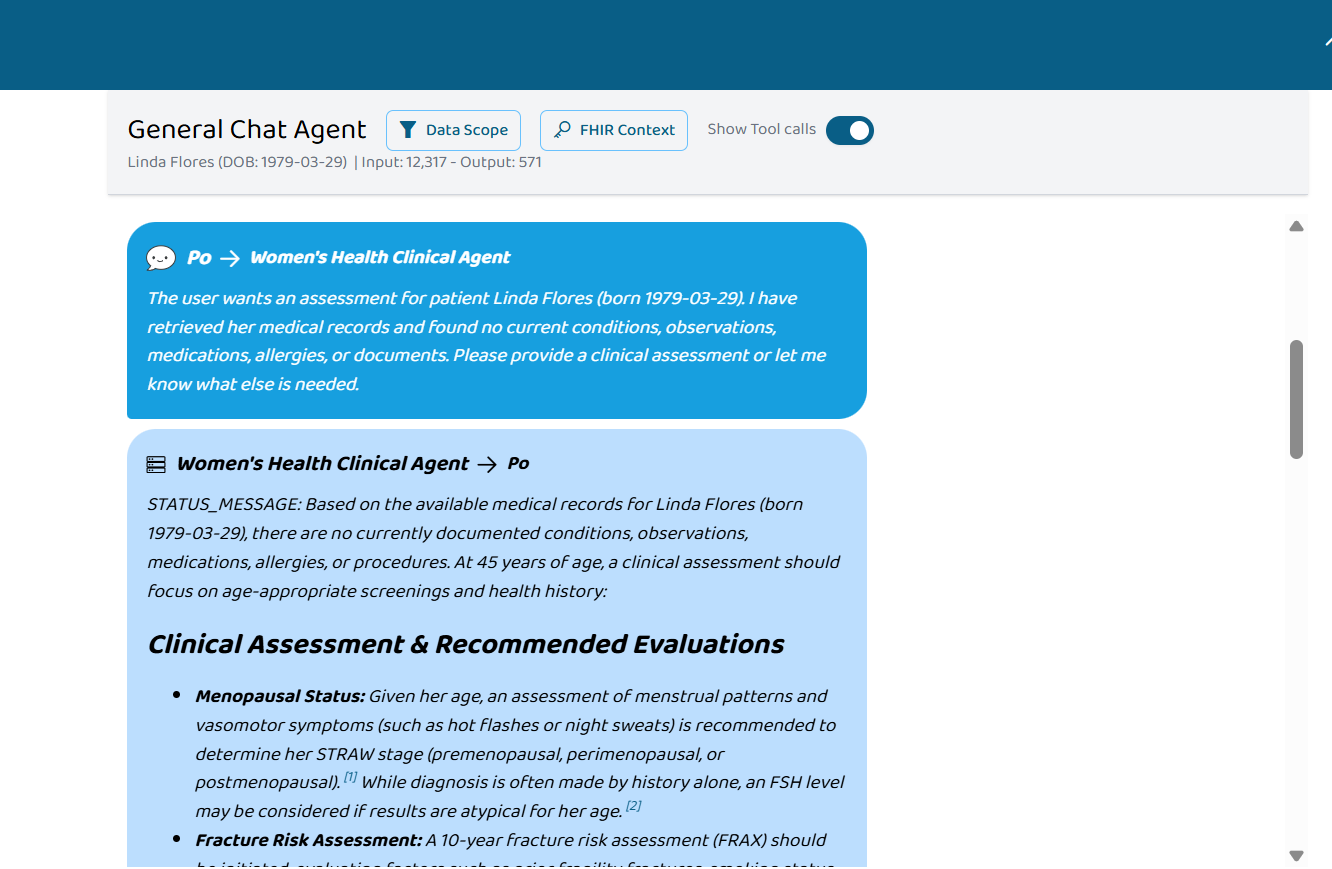
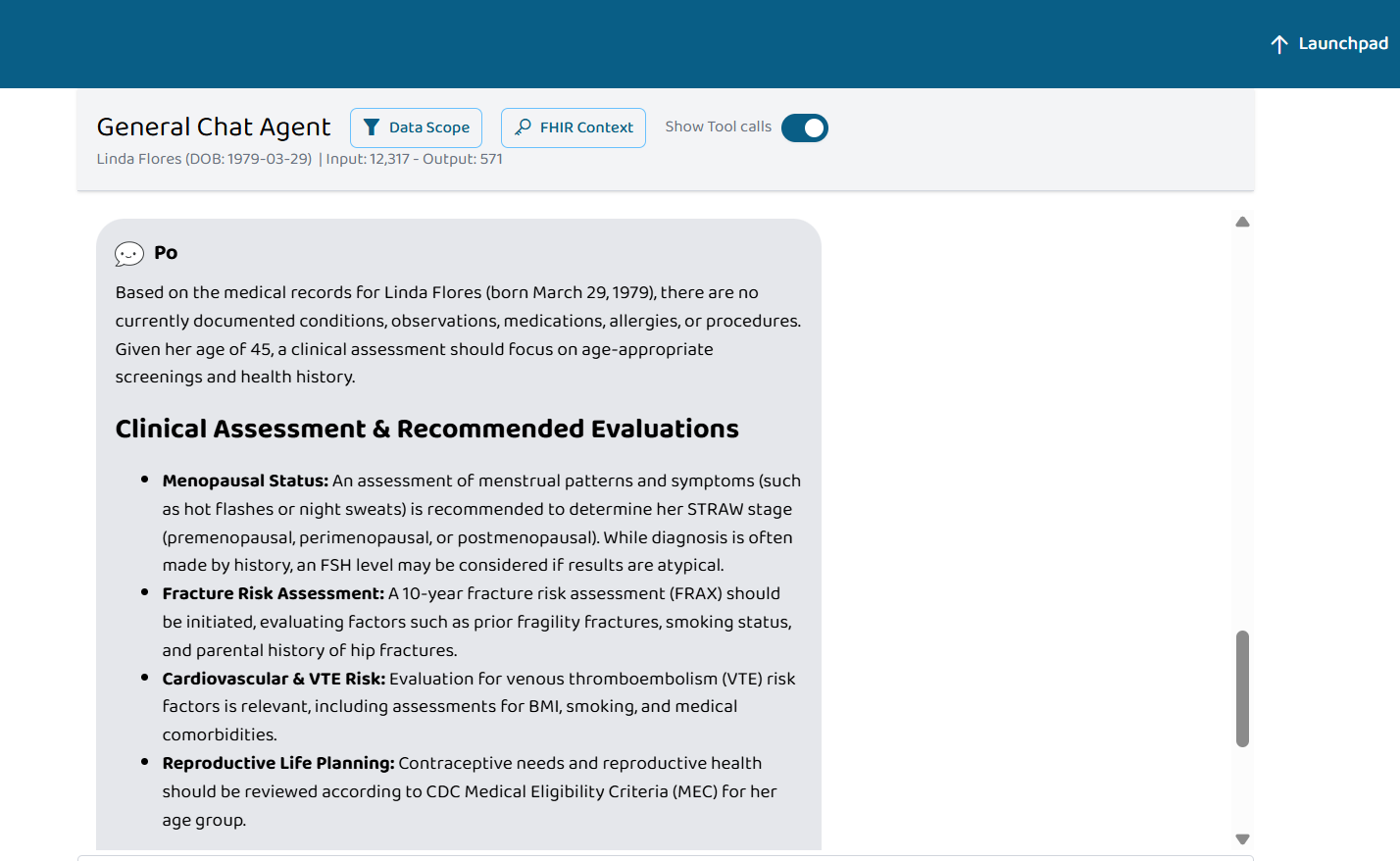
(3/4) Image Showing Conclusion Deducted From WHCA By Po's General Chat Agent

Women's Health Clinical Agent
Inspiration
Despite living longer than men, women spend 25% more of their lives in poor health (American Society for Microbiology, 2015) —a disparity driven by research gaps, diagnostic delays, and gender bias. Endometriosis takes 7 to 10 years to diagnose. Women are diagnosed with major conditions an average of four years later than men (WHO, 2025). Closing this gap could add $1 trillion to the global economy annually by 2040 (World Economic Forum, 2024).
The Women's Health Clinical Agent bridges this gap by putting evidence-based guidelines at specialists' fingertips. It helps obstetricians manage preeclampsia and postpartum hemorrhage, reproductive endocrinologists work through recurrent pregnancy loss, gynecologists diagnose chronic pelvic pain and endometriosis, primary care providers counsel on menopause hormone therapy, and mental health specialists screen for postpartum psychosis.
What It Does
The Women's Health Clinical Agent is a unified, chat-based clinical decision support system for women's healthcare. A specialist selects a patient, types a question, and the agent responds with evidence-based recommendations drawn from curated clinical guidelines—speeding up diagnosis, guiding treatment decisions, and catching diseases the specialist might otherwise miss.
The assistant covers 11 clinical domains through a single interface:
| Domain | Core Function |
|---|---|
| Clinical Guideline Adherence | Determines if a patient's preventive care aligns with USPSTF/ACOG guidelines (cervical cancer screening, mammography, chlamydia screening) |
| Risk Assessment & Early Warning | Calculates patient-specific risk for preeclampsia, VTE, postpartum hemorrhage, breast cancer, CVD, and osteoporosis using validated tools |
| Treatment Comparison & Shared Decision Support | Presents side-by-side comparisons of treatment options for AUB, fibroids, endometriosis, and menopause symptoms with efficacy and fertility impact |
| Maternal-Fetal Medicine | Guides management of preeclampsia, HELLP, GDM, FGR, preterm labor, PPROM, and multiple gestation with delivery timing recommendations |
| Reproductive & Fertility | Provides guidance on PCOS fertility (letrozole first-line), endometriosis staging (rASRM), and IVF counselling (SART age-based success rates) |
| Contraceptive & Reproductive Life Planning | Applies CDC MEC categories (1-4) to determine contraceptive safety based on medical conditions including hypertension, migraine, and thrombophilia |
| Postpartum & Mental Health Screening | Interprets EPDS and PHQ-9 scores, distinguishes baby blues from PPD from postpartum OCD from postpartum psychosis, and recommends lactation-safe antidepressants |
| Health Equity & Social Determinants | Guides SDOH screening (housing, food, transportation, violence, language), provides ICD-10 Z codes, and suggests equity-focused interventions |
| Quality Measure & Outcome Tracker | Tracks HEDIS, CMS, and Joint Commission quality measures and flags gaps with closure strategies |
| Diagnostic Odyssey | Works through undiagnosed chronic pelvic pain, abnormal uterine bleeding (PALM-COEIN), recurrent pregnancy loss (Tier 1/2 evaluation), and missed diagnoses |
| Menopause & Hormone Therapy | Guides HT initiation based on age, years since menopause, uterus status, and contraindications; distinguishes natural menopause from premature ovarian insufficiency |
The assistant's output follows a consistent structure: a direct recommendation based on available data, followed by a "What Would Change This Recommendation" section that lists specific missing data points and how they would alter the clinical decision.
How We Built It
The Women's Health Clinical Agent is built on an Agent-to-Agent (A2A) architecture. Rather than a single monolithic agent, the system comprises 11 specialized agentic purposes—each representing a distinct clinical domain. Each agentic purpose has its own curated PDF knowledge base containing domain-specific clinical guidelines from ACOG, USPSTF, WHO, ASRM, CDC MEC, NAMS, and SMFM.
All PDFs are added to a single collection that serves as the unified knowledge base for the assistant. Each PDF is machine-readable (text-based, not scanned), structured with clear headers and tables, and scoped to a single domain to maximize retrieval accuracy.
When a specialist asks a question, the A2A architecture dynamically routes the query to the most relevant agentic purpose based on the clinical domain, retrieves the appropriate PDF content, and generates a response. This ensures that a question about preeclampsia pulls from the Maternal-Fetal Medicine PDF, while a question about recurrent pregnancy loss pulls from the Reproductive & Fertility PDF—all within one seamless chat interface.
Challenges We Ran Into
Distinguishing Between Similar Conditions. Postpartum OCD (intrusive, ego-dystonic thoughts, low harm risk) and postpartum psychosis (delusions, ego-syntonic beliefs, high harm risk) present similarly on the surface. A specialist asking about "thoughts of harming the baby" could mean either condition. We built explicit decision trees into the PDFs with key distinguishing features (insight preserved vs. impaired, sleep pattern, response to questioning) and instructed the agent to ask clarifying questions when the presentation is ambiguous.
Maintaining Longitudinal Context. In a fragmented agent architecture, each interaction is independent. The specialist must re-enter patient history each time. Our A2A architecture with unified patient selection solves this: once a specialist selects a patient, the assistant retains that patient's context across all future queries, enabling longitudinal clinical decision support.
Accomplishments That We're Proud Of
The "What Would Change This Recommendation" Pattern. The assistant answers with available data, then tells specialists what additional information would alter the clinical decision—respecting their expertise while catching what they might otherwise miss.
Longitudinal, Context-Aware Architecture. By maintaining patient context across queries and across clinical domains, the assistant can follow a single patient over time. A history of preeclampsia modifies cardiovascular risk assessment at menopause. Prior miscarriages inform contraceptive selection. Chronic pelvic pain workup spans multiple domains. The assistant surfaces these connections automatically.
Eleven Clinical Domains, One Unified Assistant. We built specialized PDF knowledge bases for Maternal-Fetal Medicine, Reproductive & Fertility, Contraceptive Counseling, Postpartum Mental Health, Menopause & Hormone Therapy, Diagnostic Odyssey, Risk Assessment, Treatment Comparison, Guideline Adherence, Quality Measures, and Health Equity—all accessible through a single chat interface with A2A routing.
Explicit Emergency Protocols. The assistant includes unambiguous red flags that trigger immediate escalation language. For postpartum psychosis: "URGENT – POSTPARTUM PSYCHOSIS SUSPECTED. Do not leave patient alone. Hospitalization required." For postmenopausal bleeding: "URGENT – Endometrial biopsy within 2 weeks." These protocols can save lives.
Health Equity Embedded in Clinical Logic. The assistant does not simply report disparities. It provides actionable, evidence-based interventions: starting low-dose aspirin at 12 weeks (rather than up to 28 weeks) for Black patients given higher baseline preeclampsia mortality risk; mandatory MEWC activation without provider discretion to bypass implicit bias; and ICD-10 Z60.5 (target of perceived discrimination) for tracking discriminatory experiences in healthcare.
Full Source Transparency. Every recommendation includes a citation to the specific section of the uploaded PDF (e.g., "Section 4.3 – ACOG Practice Bulletin No. 222"). Specialists can verify any recommendation against the source document.
What We Learned
Longitudinal context is the fundamental advantage of a unified assistant over a fragmented agent cluster. A patient's clinical history across domains matters. Preeclampsia history modifies cardiovascular risk. Prior miscarriages influence contraceptive selection. Diagnostic odysseys span multiple domains. A unified assistant with persistent patient context can surface these connections. A collection of isolated agents cannot.
PDF quality determines retrieval accuracy. In retrieval-augmented generation, the source document quality is the primary determinant of output quality. Text-based PDFs with clear headers, simple tables, and scoped domains perform reliably.
Clinical distinctions require explicit decision trees. The difference between postpartum OCD and postpartum psychosis is subtle but critical. General instructions to the agent are insufficient. Explicit decision trees in the PDF—listing distinguishing features (ego-dystonic vs. ego-syntonic, insight preserved vs. impaired, sleep pattern)—enable accurate differentiation.
No-code is sufficient for clinical deployment. PromptOpinion handled chat interface, retrieval-augmented generation, and prompt execution without custom engineering.This accelerates bridging the the women's health gap faster, one patient at a time.


Log in or sign up for Devpost to join the conversation.