-
-
Screenshot of using Akash Console Network (For Deployment)
-
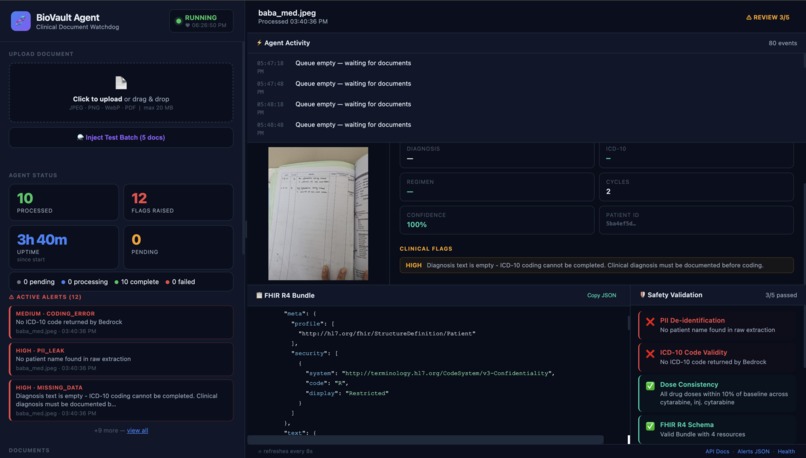
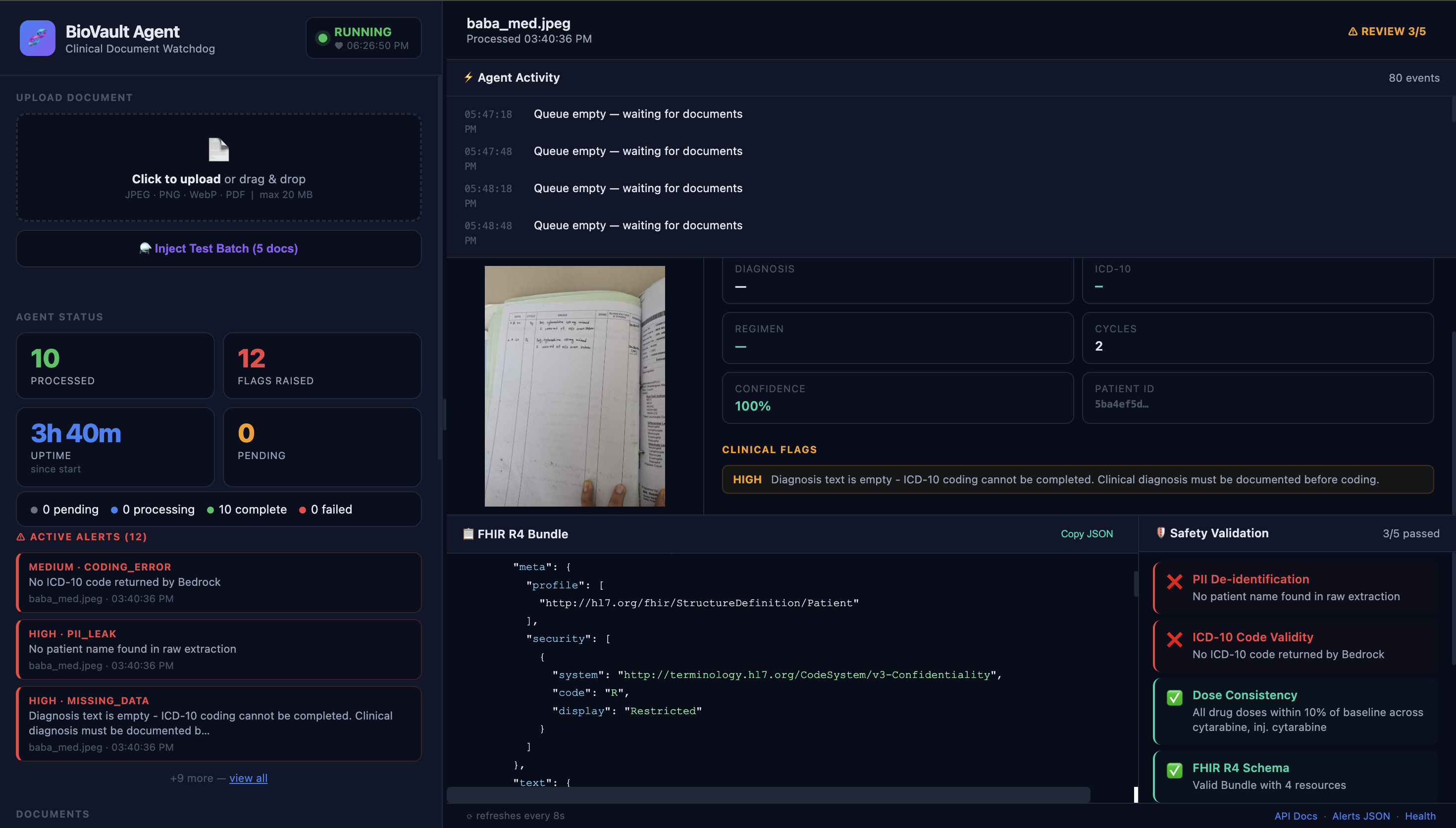
Using real world hand scripted doctor medicine delivery note
Inspiration
My father was diagnosed with blood cancer in 2024 and soon after he started his chemo, he passed away from radiation poisoning and not his cancer. It was a treatment error in Bangladesh and treatment errors globally is one of the top prominent cause of death (even in the united states), hidden away under heavy hospital bureaucracy. Coming from a Computational Biology background, I really wanted to leverage technology to solve clinical errors at a global scale especially for developing countries. Therefore, the inspiration or necessity for this project was more of a personal story for me. I wanted to build to a system that should have existed when my father needed it.
What it does
BioVault Agent is an autonomous AI watchdog that continuously monitors clinical documents, handwritten chemotherapy charts, treatment records, prescription sheets, and detects critical errors before they reach patients. It runs 24/7 without human intervention. Every 30 seconds it polls for new documents. When one arrives, it runs it through a 4-stage pipeline: MiniMax Vision extracts structured data from the handwritten image; AkashML (MiniMax M2.5) standardizes and enriches it; a FHIR R4 builder converts it to the international healthcare standard; and a safety validator checks for dose variances, unknown drug names, protocol deviations, and missing required fields. When it detects a critical issue (for example, a Daunorubicin dose drop of more than 10%, an unrecognized drug name, a missing cycle count, it raises a structured alert), logs the autonomous action with full observability, and fires a webhook to any external system listening. All results are visible on a live dashboard that updates in real time as the agent works. It is designed to catch what humans may miss.
How we built it
Backend: FastAPI with a daemon thread running the autonomous agent loop inside the same process Database: SQLite for fully persistent state: documents, pipeline results, safety flags, agent heartbeat, and an activity log survive container restarts.
Vision extraction: MiniMax Vision API reads handwritten clinical charts and returns structured JSON AI inference: AkashML API (MiniMax M2.5) handles standardization, ICD-10 coding, and clinical flag detection FHIR R4: A custom builder converts extracted data into standards-compliant healthcare bundles Safety validation: 5 deterministic checks such as dose consistency, drug name validation, cycle count verification, required field presence, and ICD-10 format compliance.
Dashboard: A single-page live UI with tabbed panels, real-time activity feed, and drag-resizable layout, no page reloads, pure fetch polling.
Deployment: Docker container on Akash Network, built automatically via GitHub Actions and pushed to GitHub Container Registry, deployed via Akash Console SDL for under $3/month. This matters for LMIC hospitals who can't afford or trust centralized cloud infrastructure with patient data.
Challenges we ran into
The hardest challenge was making the agent feel truly autonomous rather than a triggered script. Getting the daemon thread lifecycle right inside FastAPI's async context, ensuring fault recovery on startup for mid-processing documents, and building a dashboard that communicates real-time progress without websockets. I also spent time finding the correct AkashML API endpoint. The documented URL redirected and the model response structure differed from standard OpenAI-compatible APIs. I had to probe endpoints, inspect redirect chains, and validate that JSON was landing in the right response field before the pipeline worked end to end.
Accomplishments that we're proud of
That it works. You can visit the live Akash URL right now, inject a real world handwritten chart/clinical script and click Process Now. You will observe the agent monitor dose prescribed and administered, noting everything digitally, replacing a scribe, in real time. It raises alert as needed, loggs every stage, and renders the full FHIR R4 bundle and safety report.
The entire system, inference, storage, alerting, dashboard, runs in a single container on decentralized infrastructure for less than $3 a month. No cloud lock-in. No managed database. No external dependencies beyond the AI APIs.
What we learned
Fault tolerance, state recovery, and observable logging matter more than any individual feature. A system that fails silently is worse than no system at all, which is the problem I wanted to solve here. We also learned that decentralized infrastructure is genuinely production-ready. Akash Network handled our deployment cleanly, the provider was stable, and the total cost makes this viable for small clinics and hospitals in low-resource settings who cannot afford enterprise medical software.
What's next for BioVault Agent
Escalation tiers: Differentiate between advisory alerts, urgent review flags, and hard-stop critical blocks that prevent a treatment from proceeding Multi-provider Akash deployment: Run redundant agent instances across multiple Akash providers for high availability in clinical environments Audit trail compliance: Generate tamper-evident logs suitable for HIPAA and NHS Digital audit requirements And hopefully, get it into the hands of a real clinical team, so no other family goes through what mine did.

Log in or sign up for Devpost to join the conversation.