-
-
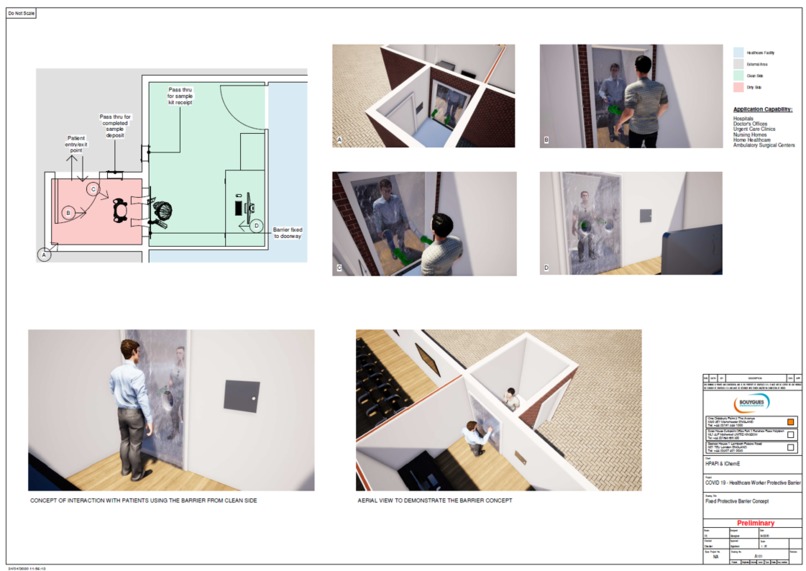
Figure 1
-

Figure 2
-
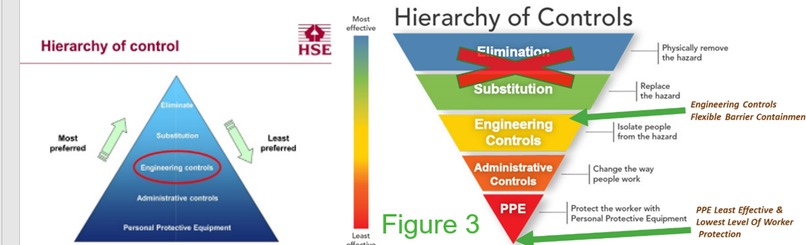
Figure 3
-
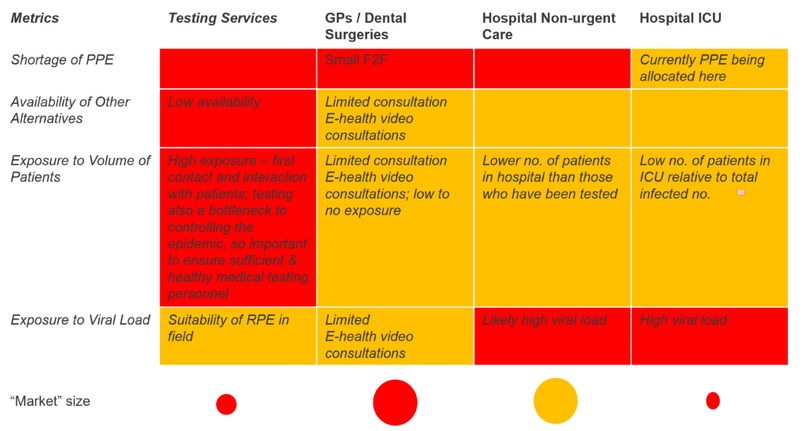
Figure 4
-
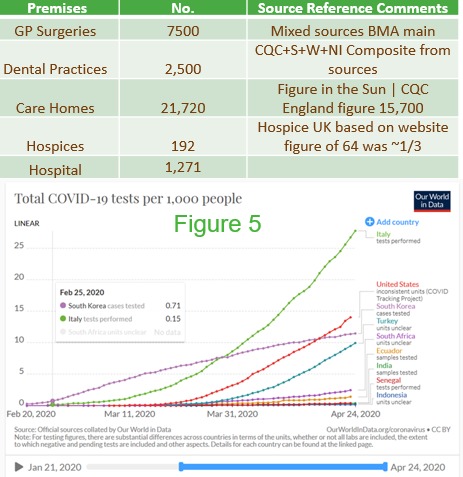
Figure 5
-

Figure 6
-

Figure 7
-
Figure 8
-
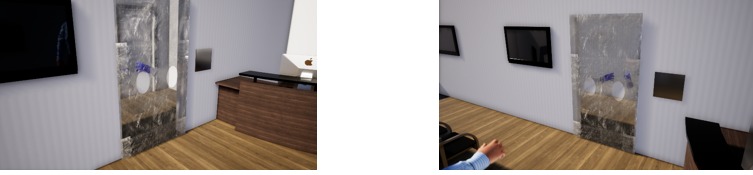
Figure 9
-

Figure 10
-
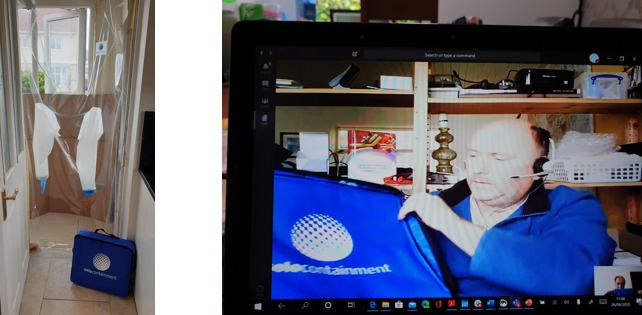
Figure 11
-
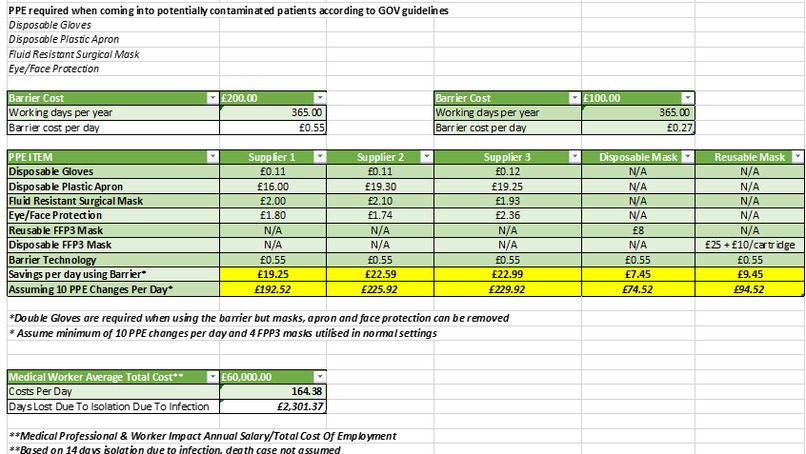
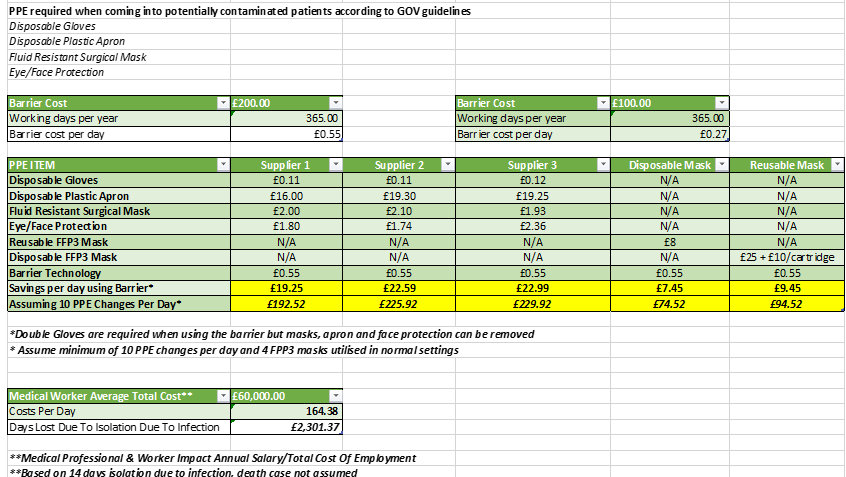
Figure 12 Cost Model





Problem the Project Solves
Problem 1: Use of PPE is the lowest level, least effective and least preferred means of protection for worker protection from exposure to hazardous substances (Principles of Control of Substances Hazardous to Health (COSHH) Regulation 7)
Problem 2: Even where PPE is used, current PPE and respiratory equipment (RPE) falls far short of the FFP3-standard masks required in accordance with EN149
Problem 3: Due to material shortages and limited PPE, non-rated surgical masks are commonly being deployed which provide inadequate protection; as only 2% as effective FFP3 masks (HSE 2008 Evaluation of Airborne Influenza)
Problem 4: PPE is the last line of defence with regards to worker protection and if engineering controls are available, they should be utilized
Background Context to problem
EN 149: Respiratory face masks are classified as FFP1, FFP2 and FFP3 dependent on filtration efficiency and EN 529 protection ratings; FFP3 most appropriate Covid 19
Due to both material shortages and current limited availability of suitable PPE, such as FFP3 rated, non-rated surgical masks are commonly being deployed which offer significantly lower respiratory protection, offering a mean reduction of 2 compared to FFP masks offering 100 times higher protection for medical workers. (HSE 2008 Evaluation of Airborne Influenza) (See Figure 2)
Based on EN 149 standards respiratory face masks are classified as FFP1, FFP2 and FFP3 dependent on filtration efficiency and EN 529 protection ratings. PPE measures are the least preferred worker protection measure and a last line of protection.
There are many other types of respirator that would be more suitable, especially powered air purifying respirator’s (PAPR) or supplied air respirator’s (SAR), however once again, these are in limited supply. The recent HSE Rapid Evidence review April 2020 https://www.hse.gov.uk/news/face-mask-equivalence-aprons-gowns-eye-protection-coronavirus.htm however permits as an acceptable comprise, use of FFP2 where circumstances permit and FFP3 are not available.
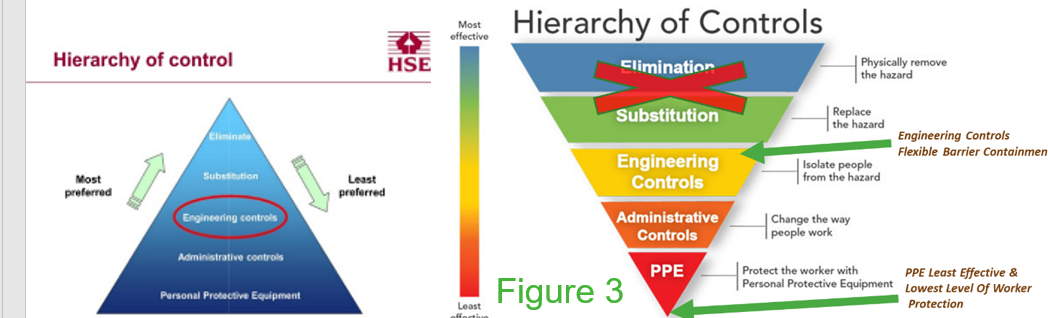
In accordance with the UK law (Control Of Substances Hazardous To Health (COSHH) Regulation 7 (3)), the use of PPE is at the bottom of the “hierarchy of control” - the lowest level, least effective and least preferred means of protection and the last line of defence for worker protection from exposure to hazardous substances. Most other countries have the same hierarchy of control (See Figure 3)
To mitigate this problem, the BarrierTech/HPAPI concept is based on the internationally accepted Hierarchy of Controls, which in a COVID-19 situation has Engineering Controls at the top of the hierarchy of control. (Elimination and Substitution are not possible).
Engineering controls offer substantially higher protection levels in comparison to “PPE”. “PPE” is the last line of defence and if breached, a worker is exposed.
Our Solution
The BarrierTech team have performed a needs analysis to establish and generate our final multi-faceted solutions which our project innovation brings.
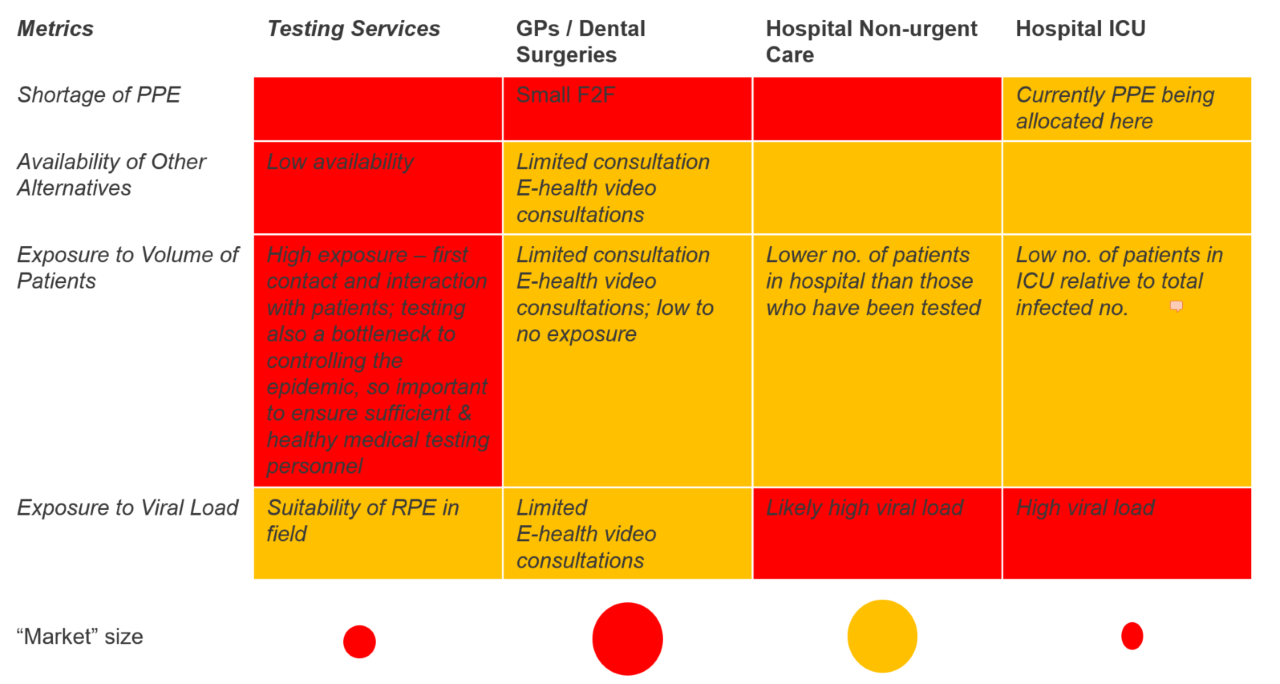
Needs Analysis: The pandemic response requires “Protection of the Medical Worker from the Patient” at an unprecedented scale. We have looked at the shortage of PPE, availability of other services, exposure to volume of patients and exposure to viral load to determine which settings barrier tech should be implemented as a first priority. Conclusion – testing services most in need of barrier tech due to high exposure and low availability of other alternatives. (See Figure 4)
Background Context to Solution
In addition to saving patient’s lives, the pandemic response unusually and untypically required “Protection of the Medical Worker from the Patient” as an additional complexity not previously encountered at this scale with communicable contagious diseases.
Global patient live saving responses have seen intense, unprecedented momentum and hyperactivity for meeting today’s current emergency situational needs within acute hospital treatment Intensive Care Settings, with additional patient capacity provided in “Rapidly Built Hospitals” throughout China, Italy and UK, never experienced or witnessed before.
Within and out with acute intensive care settings, general Healthcare, settings such as Doctor Surgeries, Dental Practices, Care Homes and Hospices for example have experienced an unprecedented level of disruption, abandonment of public service and unnecessary patient/public trauma and deaths due to inadequate health protection of key healthcare workers. The sole technique brought to bear has been so called “Personal “Protective
Equipment” or “PPE” and does not provide protection of the inhalation pathway. The BarrierTech/HPAPI Medical Professional and Healthcare Worker Protection Barrier (MPHPB) containment concept addresses and provides high-level at-risk worker protection solutions to both the Day 1 emergency treatment response and testing priorities for Covid 19 and any similar future communicable contagious disease outbreak and also provides the necessary Day 2 priority provisions and engineering barrier containment controls to maintain continuity of service and testing capabilities in general healthcare settings.
Healthcare worker interaction with patients in settings where a COVID-19 exposure risk will be present, are likely to persist for some time. The BarrierTech/HPAPI concept provides a straightforward, proven, rapidly manufactured, rapidly scalable and rapidly deployable low-cost solution to protecting both the Public, Medical Workers ultimately saving lives, for around as low as 27p to 55p a day lasting for 12 months, compared to several hundred per day for daily disposable PPE, with ultra-fast solutions manufactured in less than 8 hours and installed under 10 minutes in any fixed door setting.
Lessons learnt from the pandemic will demonstrate the critical and essential role of barrier protection strategies for now and for future pandemics, with regards in particular providing higher levels of worker protection, in addition to reduction in the overall requirements for PPE , for example where up to 4 FFP3 respirators per day may be required and up to 10 changes of PPE garments (disposable gowns etc.) in a normal setting without barrier controls compared to 1 with barrier, with the exception of gloves which will remain consistent with barrier due to double gloving protection between patient interactions.
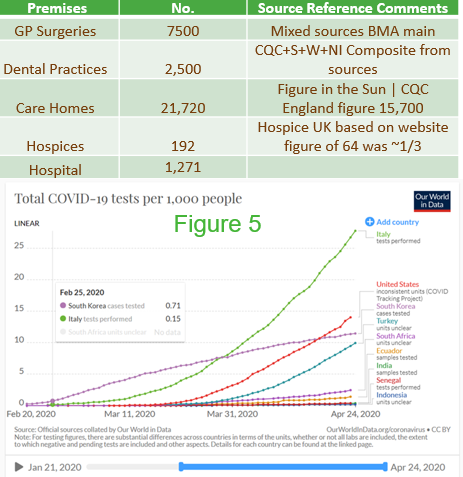
The BarrierTech HPAPI containment solution can be applied to a broad range of Acute and General Healthcare settings on an international scale, for both Day 1 and Day 2 post pandemic priorities. The magnitude of the opportunity, for UK only is illustrated below as an example of demand for a selective number of settings only, but not limited to these. (See Figure 5)
Based on recent world data published as referenced below, indicates the requirement for 19 Covid tests per 1,000 of population, in UK with a population of circa 60 Million this would equate to 1.8Million tests, therefore our initial priority is focused on fixed testing stations deployed rapidly on a mass scale, rather than acute emergency hospital settings requiring mobile devices where less patients are encountered.
The HPAPI flexible barrier solution offers a robust worker protection solution, at the top of the Hierarchy of Control, based upon the application of proven existing barrier isolator technologies for protecting workers from High Hazard Substances from the Pharmaceutical, High Containment Industries and Barrier Nursing to General Healthcare Settings. (See Figure 6)
The highly flexible and innovative BarrierTech solution based on the HPAPI design invention has been used for protecting workers in manufacturing settings and has been “Proof of Concept” prototype tested in medical healthcare settings. The team is working towards the next stage of Technology Adoption, immediately deployable within a broad range of settings from GP Surgeries, Dental Practices, Care Homes, Hospitals and Pharmaceutical Corporates for the highest impact potential. The team are currently installing the device in real medical settings in the USA and Ireland, and within a Mental Healthcare Setting.
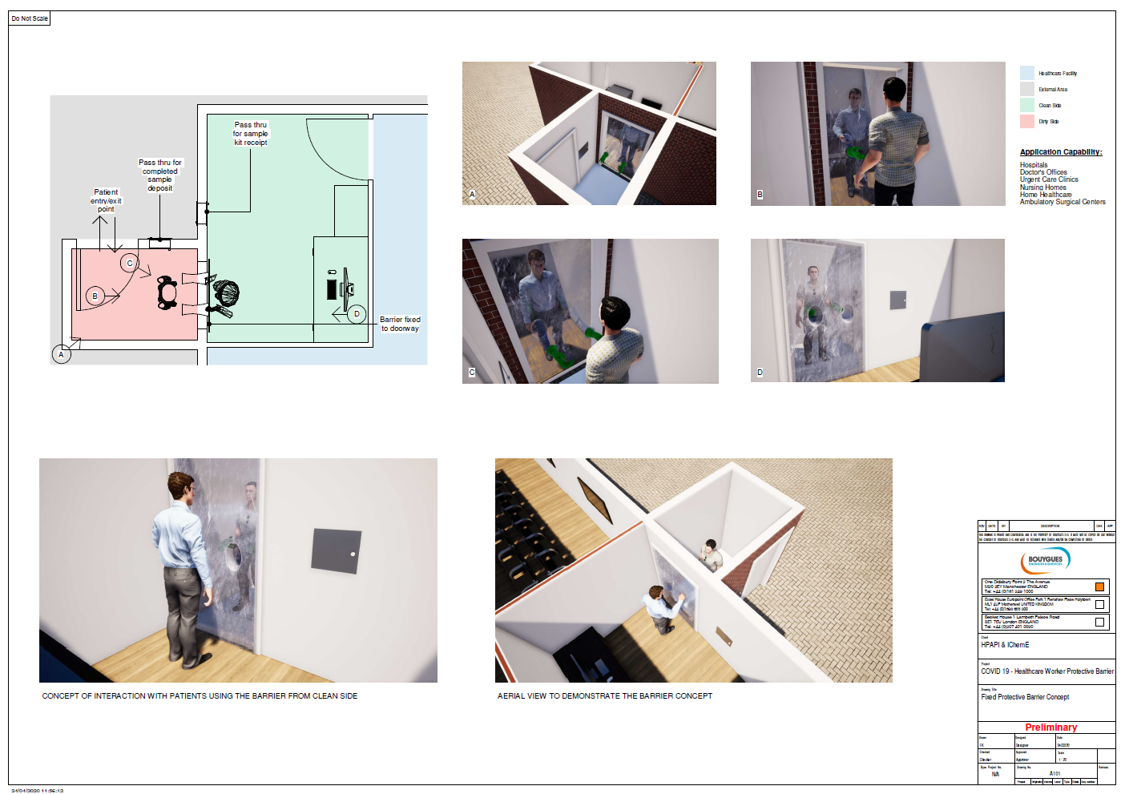
The flexible barrier solution is available and most effective in static settings where a ‘patient’ can be presented to the barrier, such as doctor’s surgeries, healthcare centre’s, care homes, nursing homes, dentists, drive-through centre’s and similar. Deployment can be in doorways, corridors and similar locations, in any size or shape. Gloveport numbers and locations can be changed easily. A mobile derivative has application in settings such as hospital wards and locations where patient mobility is limited. (See Figure 7)
The flexible barrier solution also offers the highest level of comfort and ergonomics for performing a range of critical medical procedures, previously demonstrated, performed and proven in the proof of concept prototype setting including cleaning, bio decontamination for subsequent patient protection and medical sample transfer. (blood, swab, etc.)
The flexible barrier solution compared to normal healthcare settings due to the reduction in PPE and the lesser frequent number of PPE changes daily by the healthcare worker, provides at least a doubling of the potential of patient who could potentially be tested (See Figure 8)
The HPAPI flexible barrier is an ultra-fast, ready to roll out solution, based on proven rapidly scalable prototype solution, utilizing the latest start-of-the-art CNC programming and RF polymer welding advanced manufacturing techniques. Concept to drawing to design and manufacture has been completed in less than 8 hours and can be installed in operational settings in less than 10 minutes using low skill tradesman. (See Figure 9)
Horizontal, vertical supply chains and Advanced Manufacturing partners onboarded and in place with manufacturing fabrication drawings available reputable global network, target minimum of 1,000 barriers per week (See Figure 10) The flexible barrier solution is constructed from readily available PVC, Polyurethane and Polymeric materials, which are different raw materials and material supply chains to those currently engaged and saturated to capacity in the current Covid response and relief efforts, which underpins the resilience and short, mid and long term sustainability of the HPAPI Professional and Healthcare Worker Protective Barrier Systems
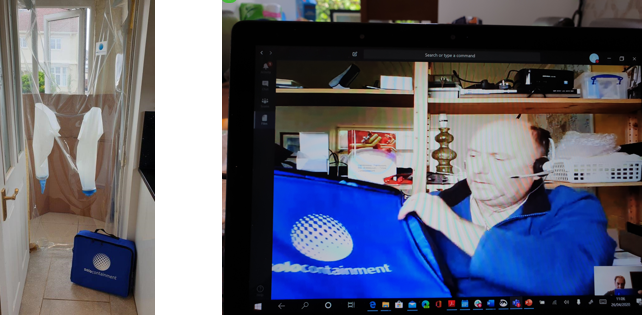
Due to the extremely compact and lightweight nature of the HPAPI flexible barrier, the solution can be transported with ease, in a very convenient foldaway bag (See Figure 11)
The HPAPI barrier solution will reduce the requirements for and the volume of PPE utilised due to the nature of the barrier protection and more importantly provide a higher level of healthcare worker protection. For cost modelling purposes, PPE assumptions are taken from harmonized UK/WHO sources for recommended levels of PPE protection. It is worthy of note that a properly installed barrier may last up to 12 months. (See Figure 12)
Progress Over the Weekend
With the help of our mentor, Zera Ong we achieved the following successful outcomes during the weekend Hackathon:
• Ability to frame the problem more succinctly • Prioritise and focus our offering to fixed testing stations due to demand • Development of cost model to support the ROI with this solution • Production of an animated visualisation and video to better promote our solution in layman’s terms • Prepare 2-minute pitch utilising multiple iterations on Slack via Zoom • Continual refinement and optimisation of solution through checkpoints 1,2 and 3 as progress, planning and problem-solving gate stages
Impact of Solution
Impact 1: Available now based on existing proven technology to be deployed in new health care settings, no requirement for regulatory approvals as not PPE, therefore not classified as Medical Device and such CE marking also not required
Impact 2: Preserving quality of life and maintains continuity of healthcare service and critical infrastructure
Impact 3: Extensive proof of concept prototype testing completed with end point medical procedures demonstrated
Impact 4: Flexible barrier containment solution based on engineering controls effectively reducing medical worker risk and offers significantly higher levels of protection, saving lives with additional projected benefits of saving £13,000 per month on alternative PPE solutions
Impact 5: Highly flexible formats comprising of 2 product configurations; fixed and mobile testing stations which can be installed within a doorway setting using low skilled workers in under 10 minutes, ease of mounting and disassembly
Impact 6: Allows doubling of patient throughput, more patients can be tested and treated as decontamination not required on the clean side of the barrier and associated 10x lower requirement of PPE
Impact 7: Rapid response technique to current and future pandemics, compact, easily transportable, user friendly, adaptable and customisable to a range of settings and testing/procedure/treatment requirements in a foldaway format
Impact 8: Utilisation of ultrafast advanced manufacturing CNC technologies for rapid manufacturing and scale up with concept to completion less than 8 hours with a minimum target of 1000 barriers per week with supply chain partners onboarded for rollout
Impact 9: Sustainable solution reusable for up to a year and can be used as an alternative or in combination with PPE providing resilience against PPE shortfalls
Impact 10: Barrier solution can have far reaching impacts and can be deployed in any face to face medical setting including GP surgeries, dental surgeries, hospices, hospitals, veterinary, care homes, podiatry and many other medical settings
Next Steps
- Investment will be spent on getting barriers designed, manufactured and into healthcare settings, FOC, ASAP.
- Support for distribution of barriers to test within healthcare settings
- Strategic contact with national healthcare providers, governments, healthcare professional organisations etc to raise awareness and move away from the single, blinkered reliance on so called “PPE”
- Awareness raising that better alternative to PPE available now
- Persons to install barriers in healthcare settings. Competent tradesperson needed. Simplest barriers are taped to door, secured with batten. More complex medical environments = slightly more complex installation. Military personnel best to do installation if available.
- Writing installation procedures and operating procedures and training for use of barriers. We will do this for free, but logically and morally we should be paid to do this. Some of us currently have no income. We have access to many people who can support this via professional bodies and others.
- More cash to increase delivery
- Exported at scale already. Support for expansion into healthcare settings worldwide
- Review of legal support e.g. for purchase, indemnities, warranties
Value after Crisis
• Every healthcare setting in the world will need one in its emergency store cupboard for future pandemics
• Please refer to solution and impacts section previously described, not duplicated here




Log in or sign up for Devpost to join the conversation.