About the Project
What inspired us
Emergency departments are chaotic, but not because care is impossible. It is because information does not reach the right person at the right time. Doctors spend nearly half their shift on documentation, while patients wait on coordination gaps.
We were also frustrated with how opaque most AI systems feel. If a model makes a claim but cannot explain it, trust breaks. That led to our core idea: every output should be inspectable and correctable.
Finally, privacy pushed our architecture. Sensitive patient data should not leave the hospital, and personal records should stay with the patient. That principle shaped everything we built.
What we built
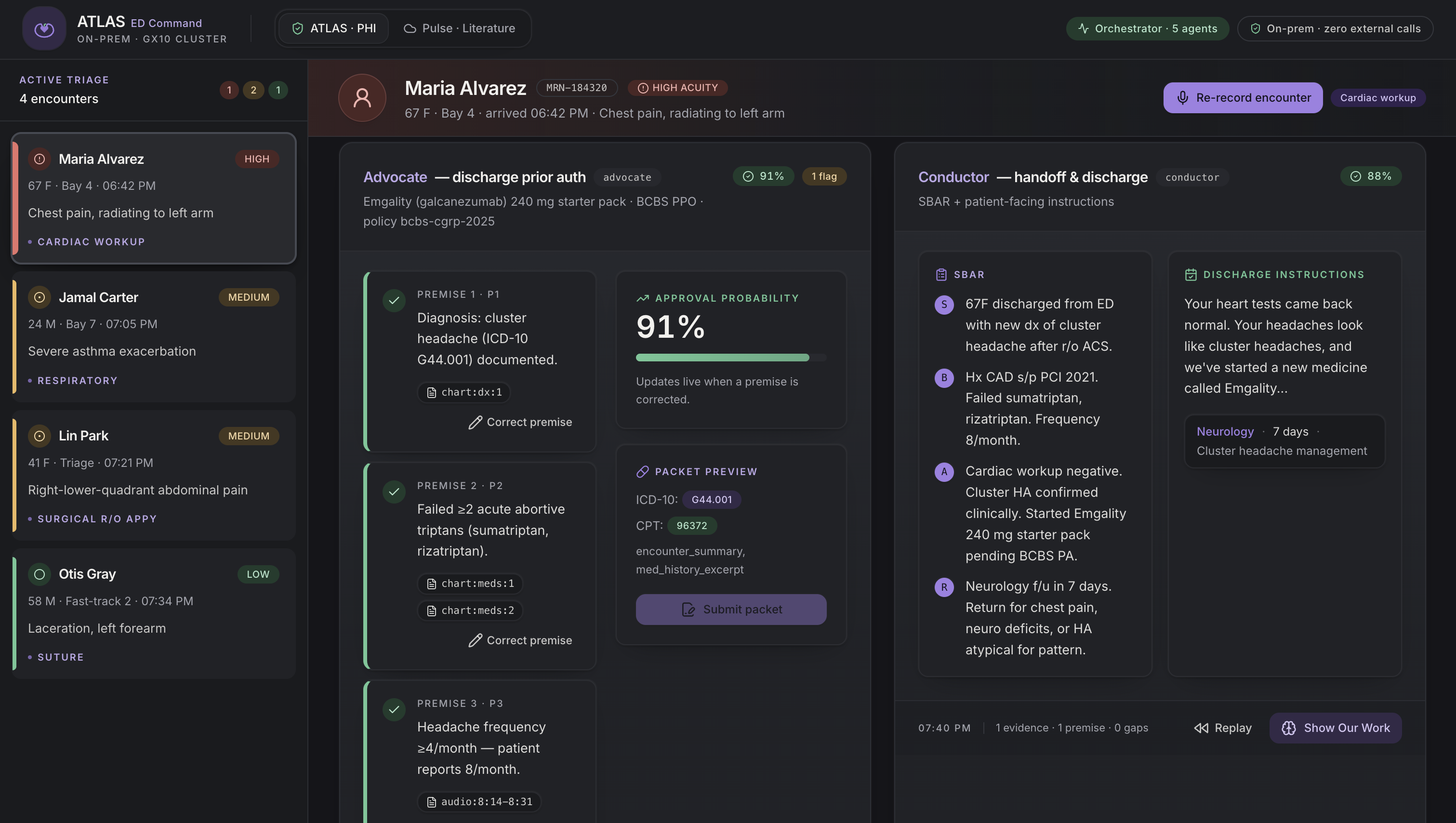
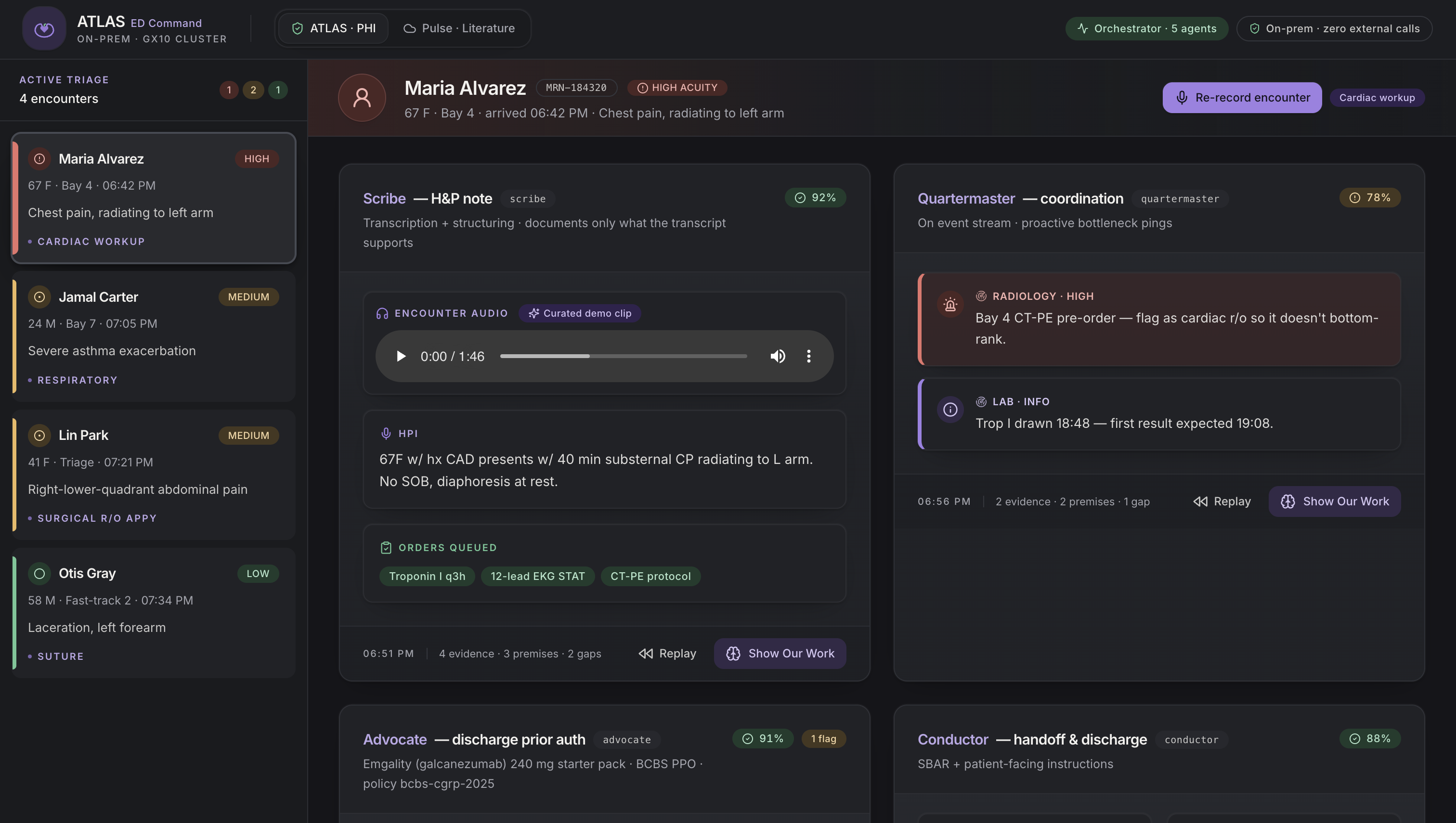
ATLAS is an on-prem, multi-agent system for emergency departments. It runs locally and coordinates five agents:
- Scribe writes clinical notes from encounter audio
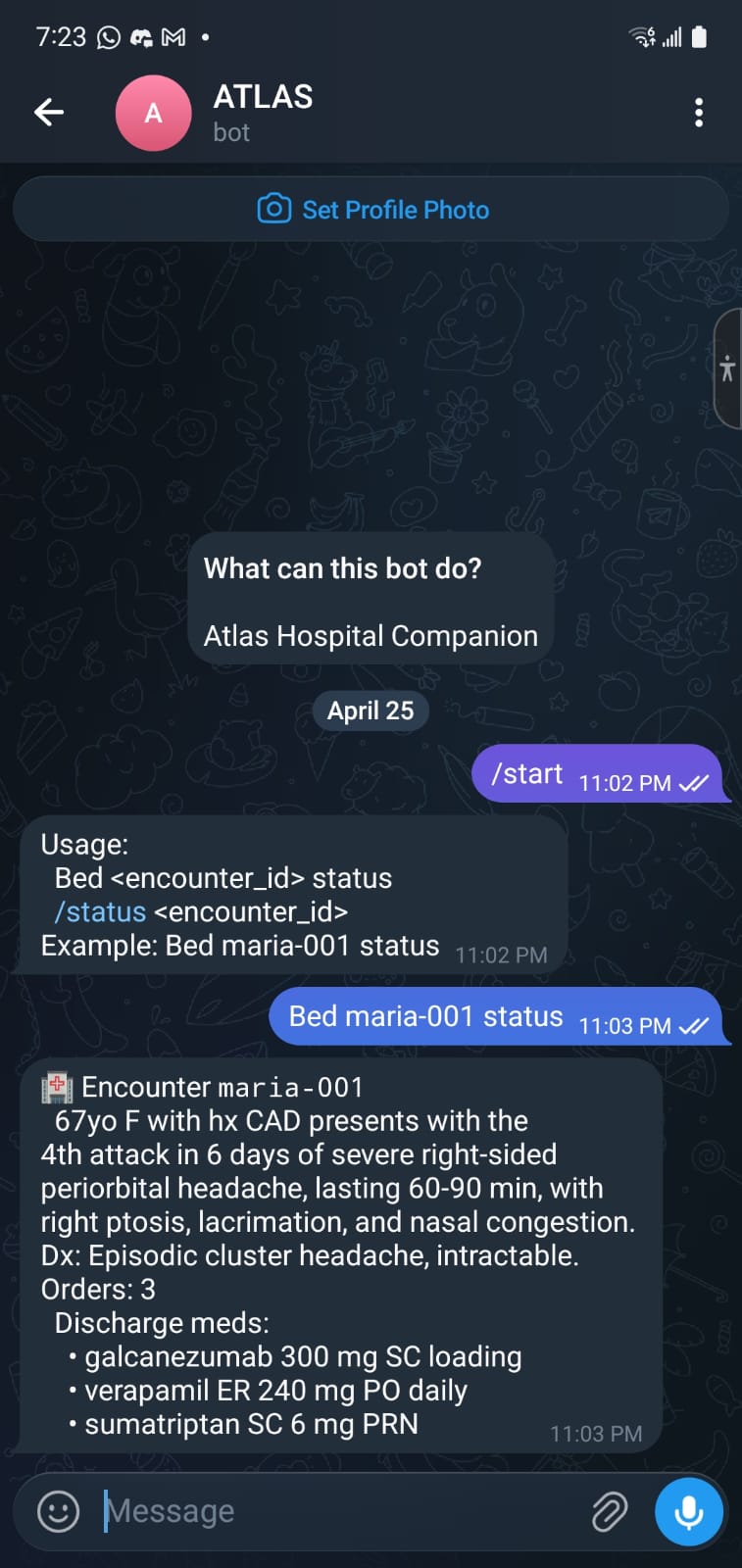
- Quartermaster manages coordination and predicts delays
- Advocate prepares prior authorizations during the visit
- Conductor generates handoffs and discharge plans
- Reality Check audits all outputs for errors
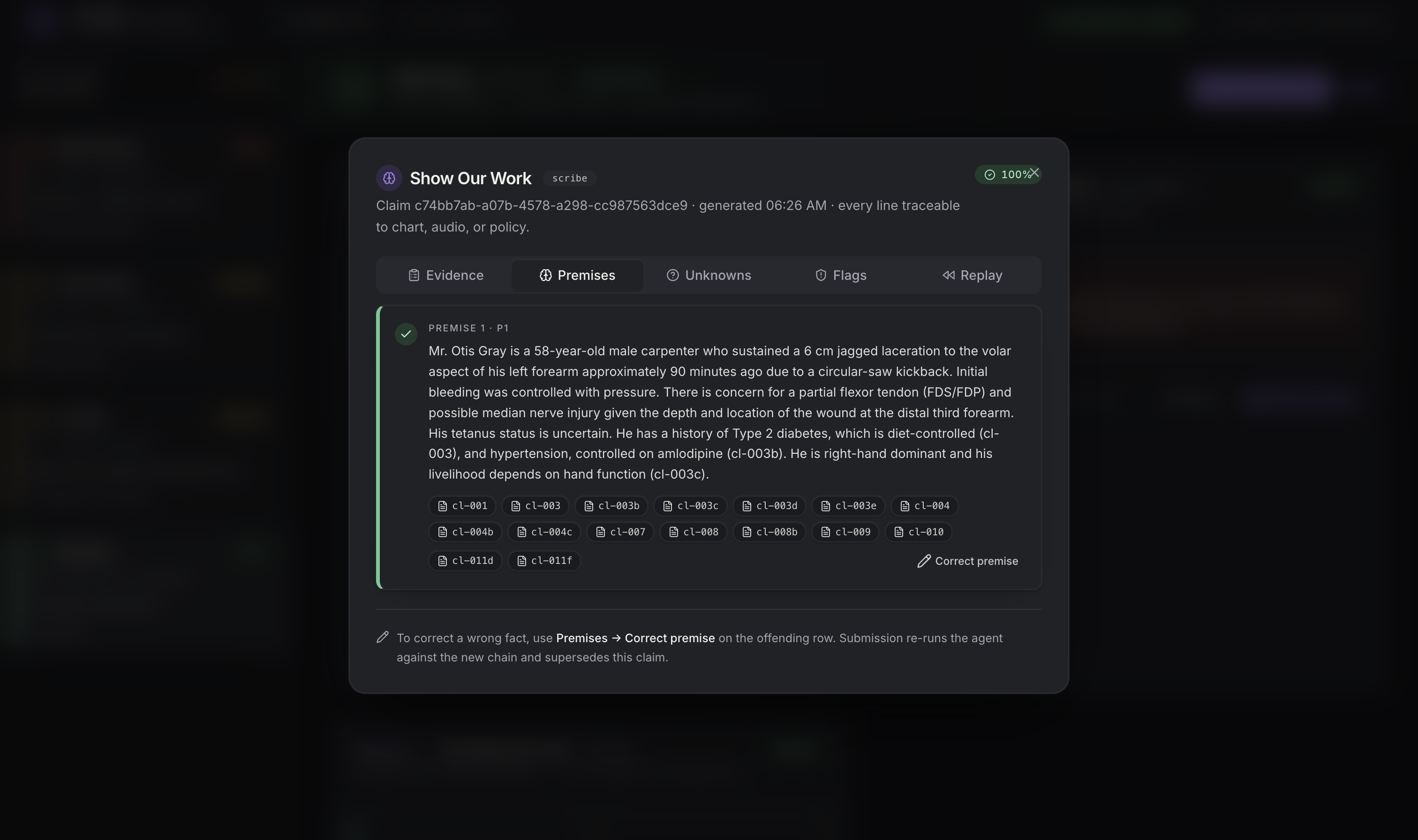
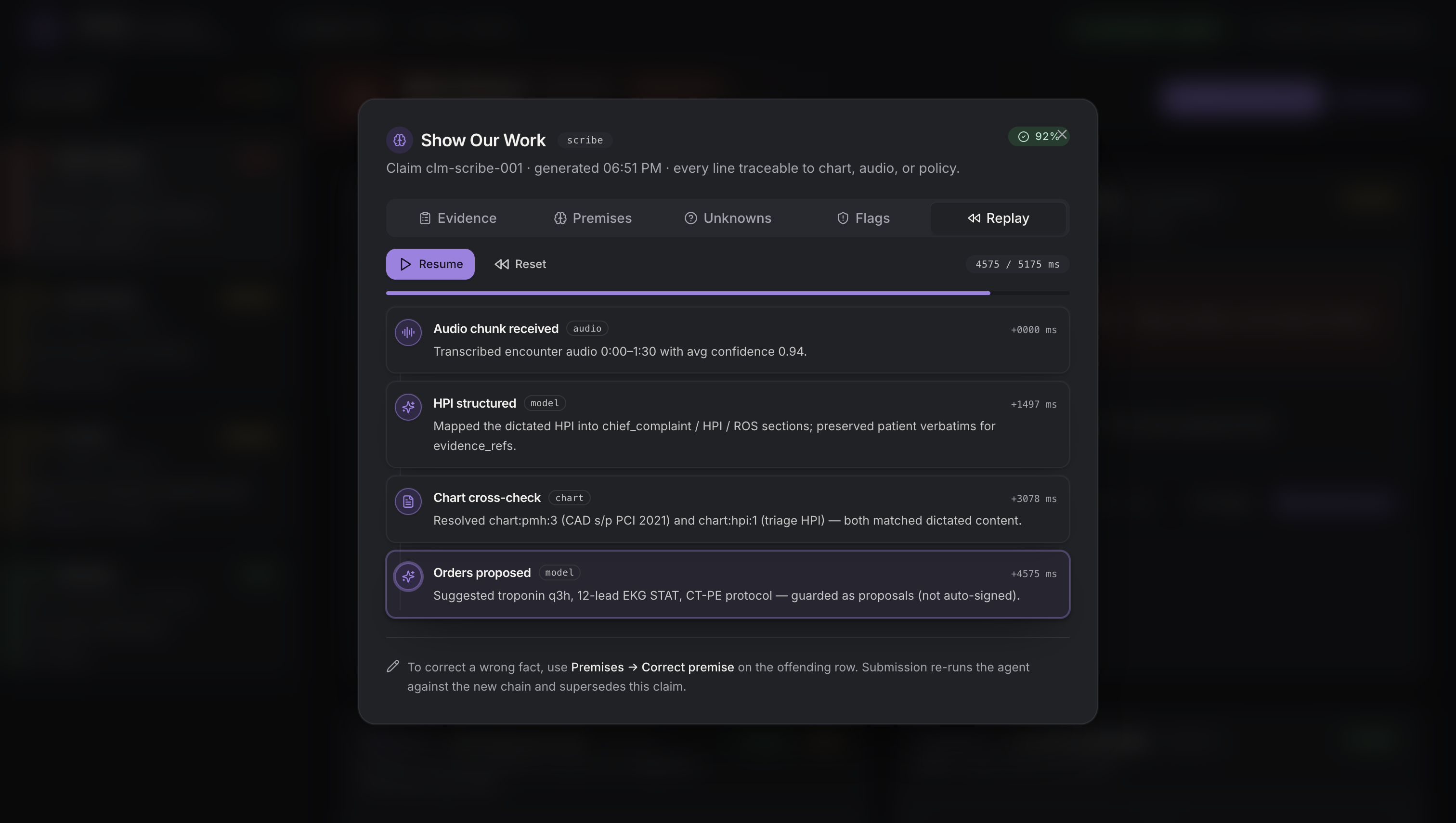
The key feature is “Show Our Work”. Every claim is backed by evidence and a reasoning chain that doctors can inspect and correct. If a premise is wrong, the system recomputes instantly.
We also built:
- Pulse: a cloud-based medical literature companion with zero patient data
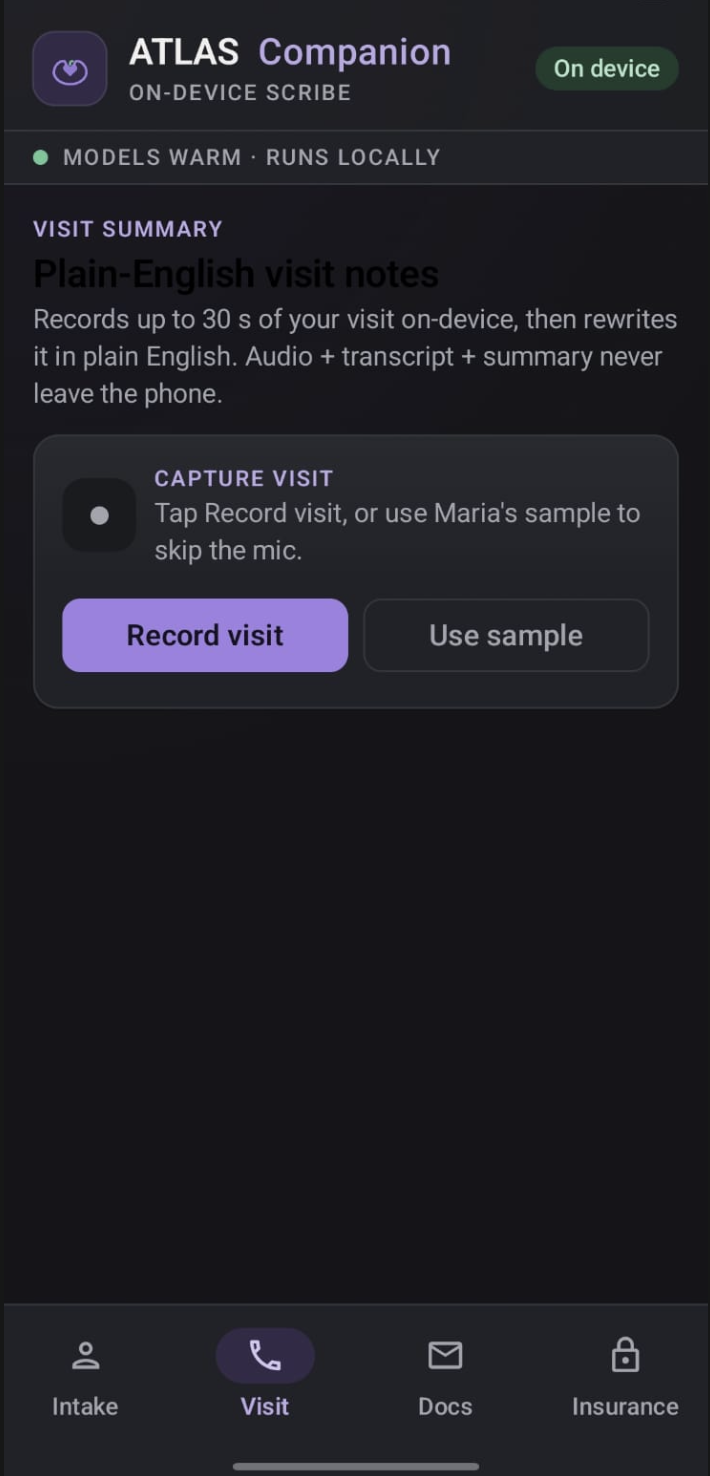
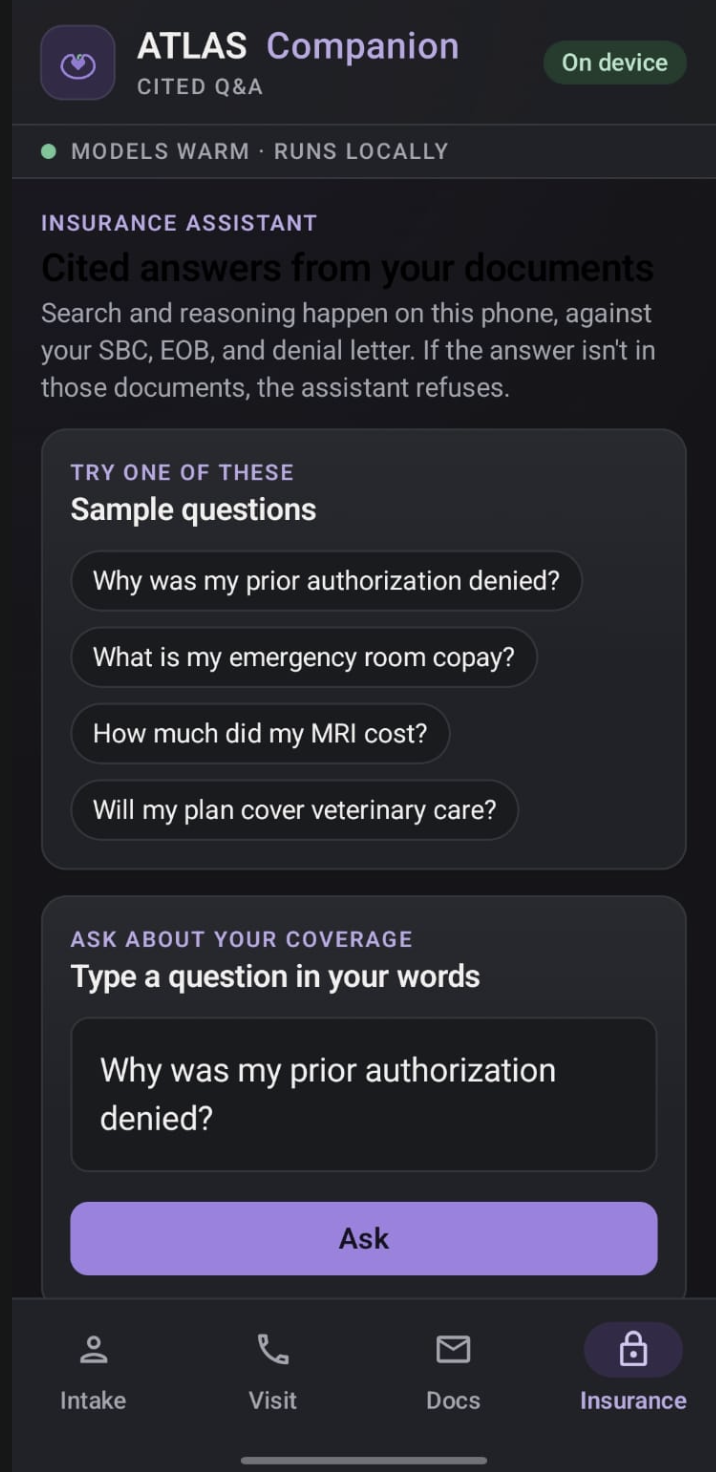
- Patient Companion app: an on-device app that summarizes visits and answers insurance questions using only the patient’s own documents
How we built it
We designed ATLAS as a local-first system running on a single machine with shared memory for multiple models.
- A central orchestrator routes events between agents
- Every output must include evidence and a reasoning chain
- If an agent fails to provide evidence, it is rejected and rerun
We used larger models for reasoning-heavy tasks and smaller ones for fast updates. Speech-to-text powers live documentation, while embeddings support retrieval.
On the mobile side, we built a Kotlin app with fully on-device models. For retrieval, we used lightweight cosine similarity over small vector sets instead of heavy infrastructure.
We also enforced a strict architectural boundary: [ \text{PHI (ATLAS)} \cap \text{Pulse} = \emptyset ] No patient data ever crosses into the cloud system.
What we learned
- Transparency matters more than raw model power
- Constraints like running on-device lead to better system design
- Multi-agent systems are only valuable if agents truly interact
- Good storytelling is as important as good engineering
Challenges we faced
- Scope: building multiple agents in limited time required strict prioritization
- Latency: responses needed to feel real-time, especially after corrections
- Speech input: live transcription is unreliable, so we built fallbacks
- Accuracy: enforcing evidence-backed outputs required system-level constraints
- On-device limits: mobile performance and memory required careful tradeoffs
Closing
ATLAS is not about replacing clinicians. It is about making AI a transparent teammate.
Instead of black-box outputs, we built a system where every decision can be traced, challenged, and improved.
Built With
- agentverse
- asi:one
- asus-ascent-gx10
- kotlin
- lmf2.5
- medgemma
- ollama
- postgresql
- python
- qwen
- react
- samsung-galaxy-s25
- telegram
- vllm
- whisper-large
- zetic

Log in or sign up for Devpost to join the conversation.