-
-
Thumbnail
-
-

-
-

-
Inspiration
The numbers are not abstract and they are going the wrong way.
- 12.8 UK maternal deaths per 100,000 maternities in 2022 to 2024, around 20% higher than a decade earlier.
- 45% of those deaths were judged potentially preventable with better care.
- It is not random who dies. Black women are around three times more likely to die, women in the most deprived areas roughly twice, and 91% of the women who died had faced multiple overlapping challenges.
The dominant finding of the Birth Trauma Inquiry was the simplest and the hardest. Women raised a concern and were not listened to. Every pregnancy app on the store is built for the median user, well-served, English-speaking, low-risk, already heard, because the median user monetises. Artemis is built for the inverse. The high-risk, migrant, deprived, mental-health-complex, dismissed cohort everyone else designs past.
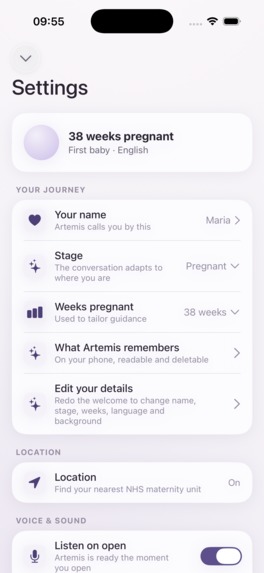
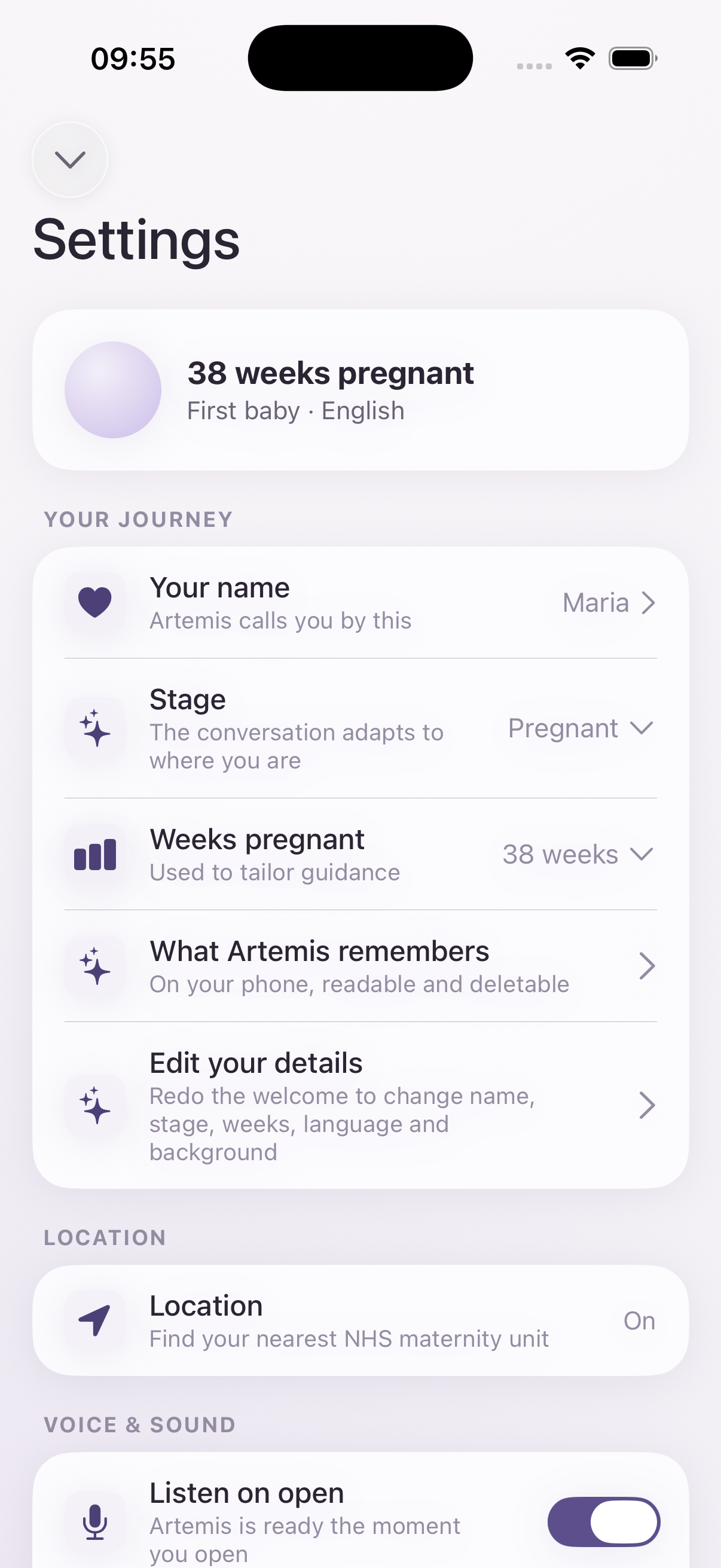
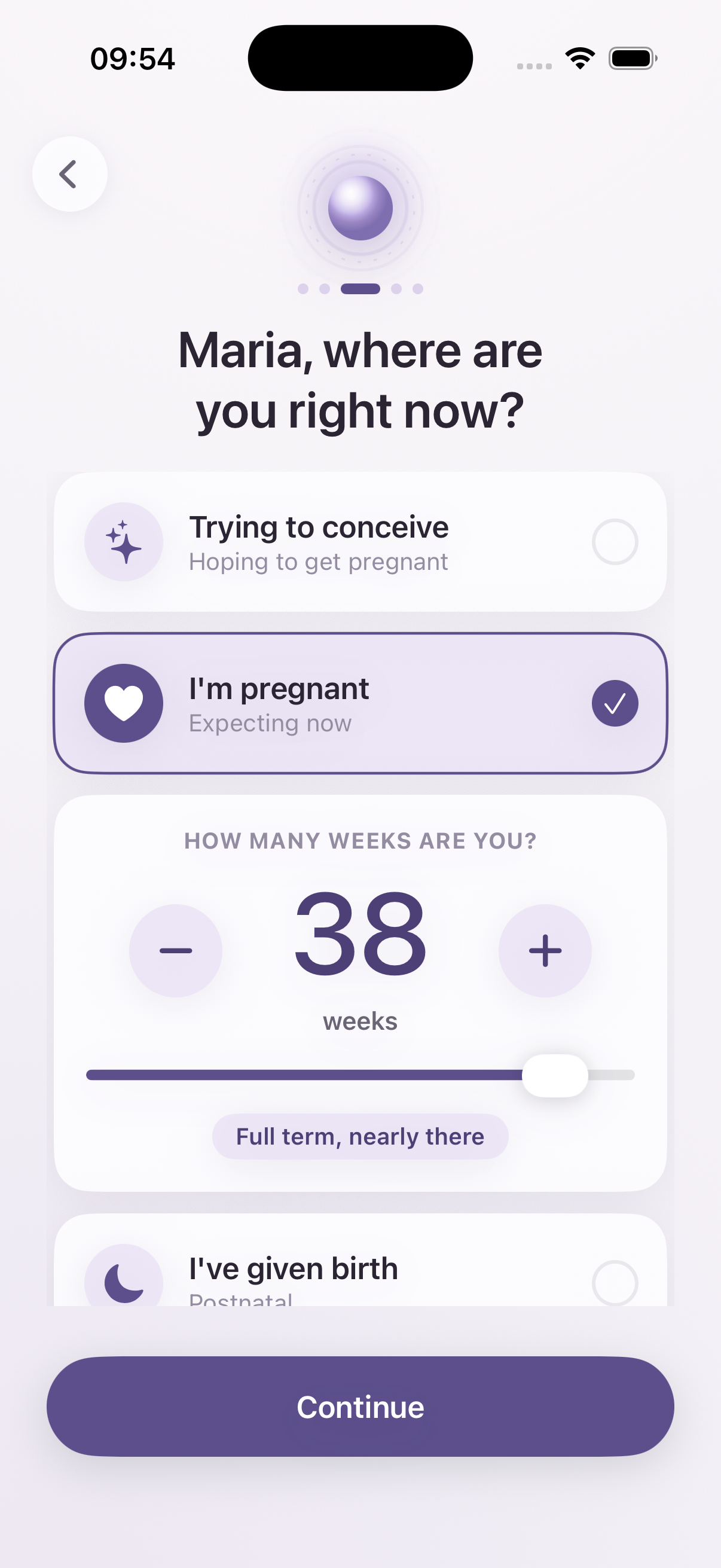
What it does
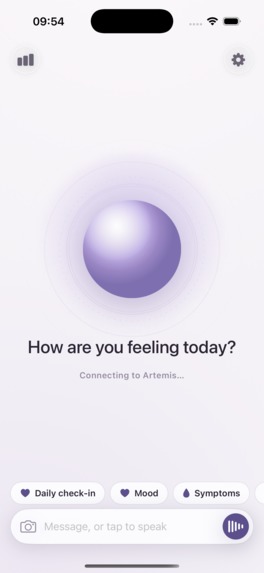
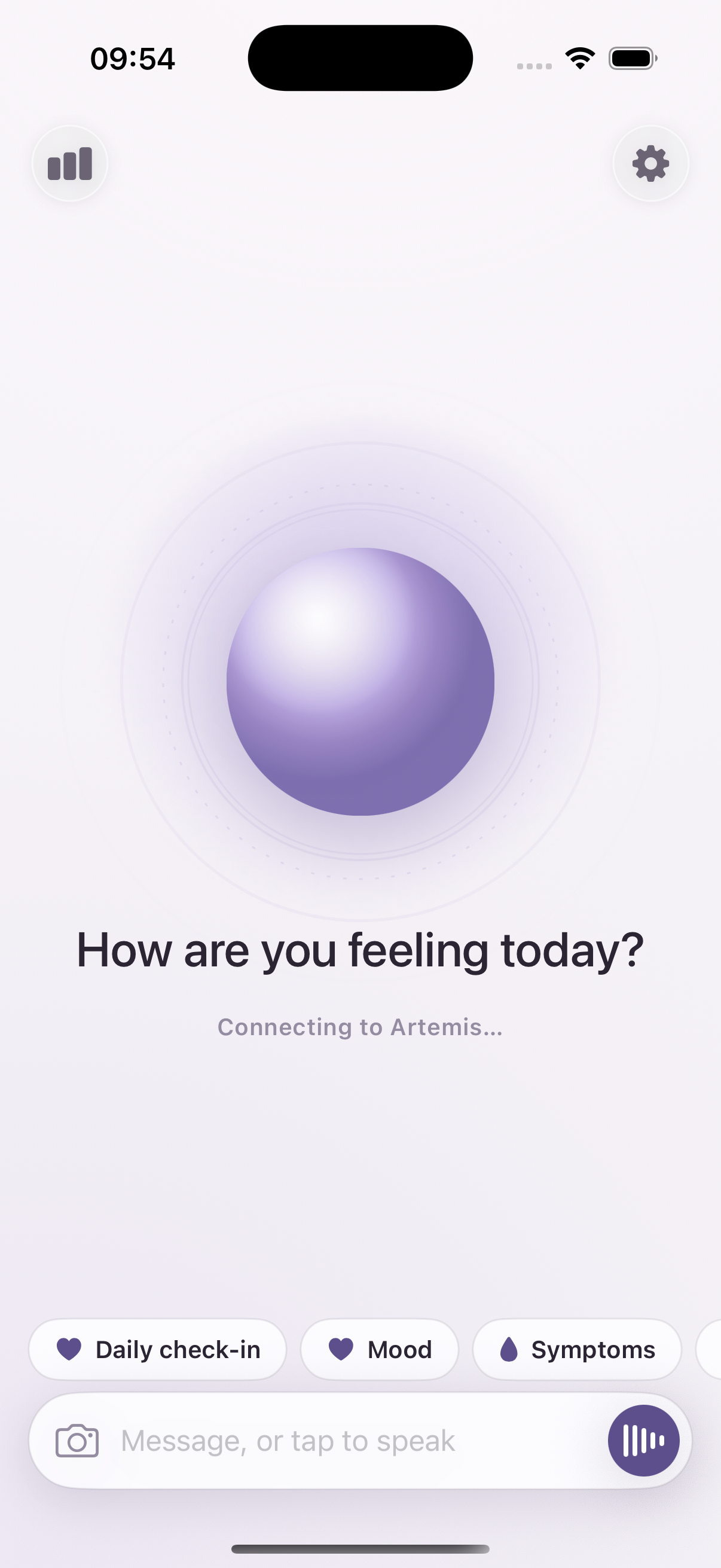
Artemis is a voice-first maternity safety companion for the women the system fails. She is named for the goddess invoked in childbirth. You open the app and she is already listening. A text box is always there for when you cannot speak.
Three mechanics no incumbent combines, shipped together.
- Listen. Voice-first triage. You describe a symptom, and the clinical answer is retrieved from NHS content and quoted on screen, not improvised.
- Route. Care navigation. On an urgent verdict, the nearest real maternity triage unit, one tap to call, not a generic see your GP.
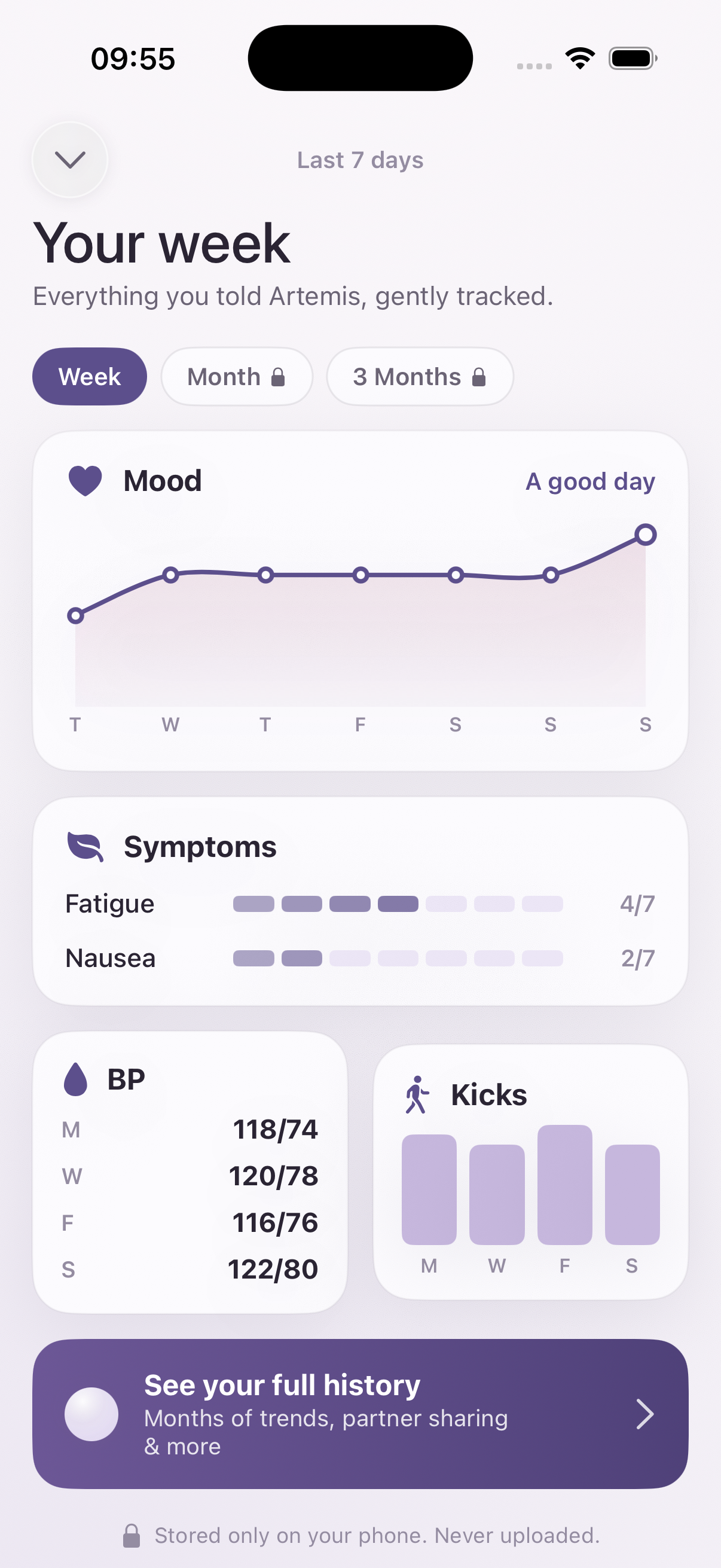
- Advocate. The handover. One tap turns weeks of her logged history into a clinical script she reads to a midwife, so a dismissed woman becomes impossible to ignore.
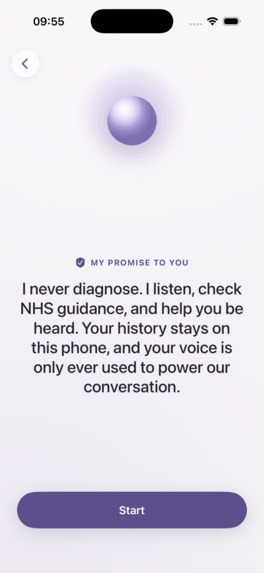
An equity layer designed in, not retrofitted. Multilingual voice, because interpreter gaps in maternity are a named safety failure. Surveillance-free by design, no NHS login and no immigration data, so migrant women are not deterred. And drift detection focused where the deaths actually are, perinatal mental health, pre-eclampsia, reduced fetal movements, and sepsis.
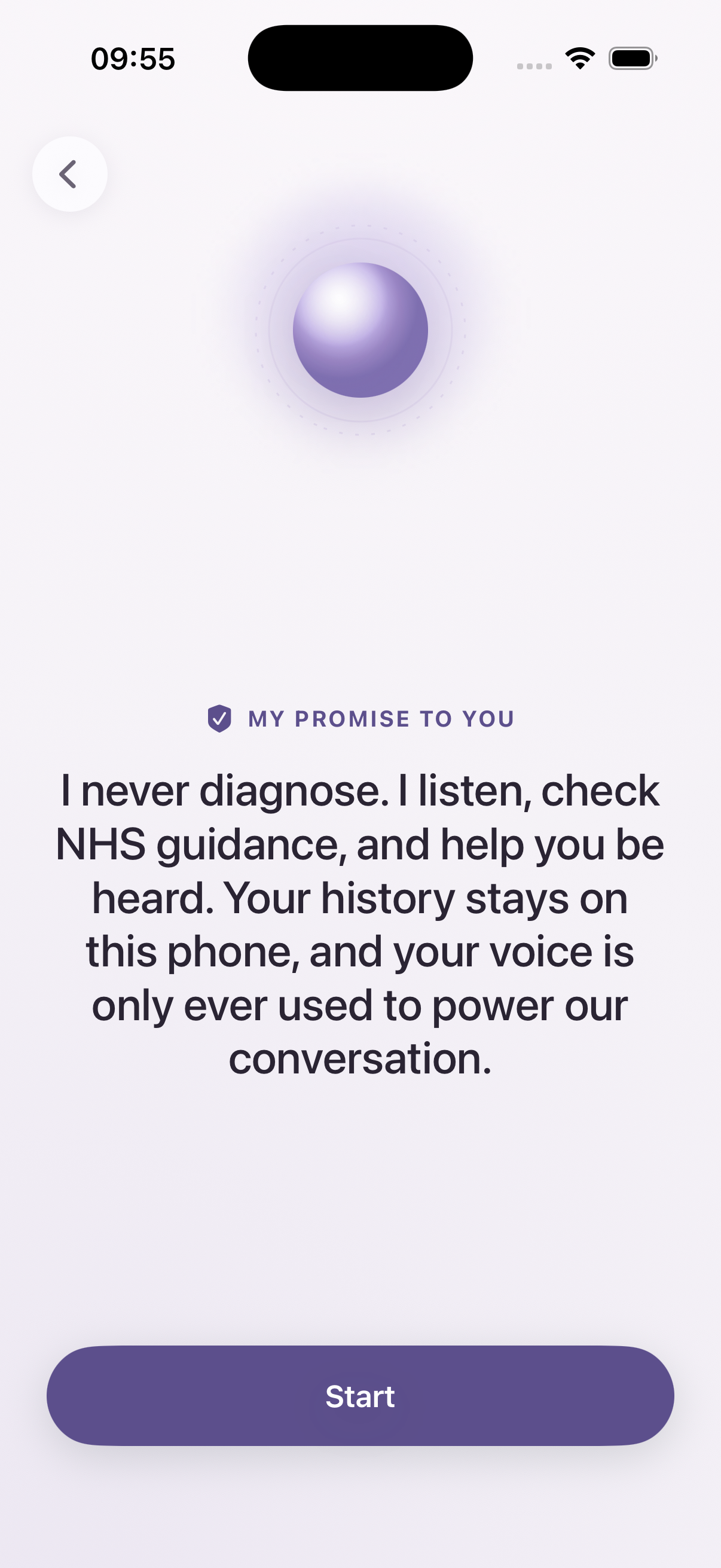
She does not diagnose. She supports communication and navigation, and she is escalation-first by design, so when something is uncertain she errs toward get checked.
How we built it
Solo, inside the hackathon.
- A native SwiftUI and SwiftData iOS app, voice at the centre.
- The OpenAI Realtime voice model over WebRTC, with a Cloudflare Worker minting short-lived ephemeral keys so no secret ever ships in the app.
- Retrieval-grounded answers from NHS content, with the citation rendered on screen, so the model cannot invent clinical advice. NHS routing is wired to the Directory of Services with a cached fallback for demo day.
- Built with Claude as the engineering pair throughout, and Fotor for the cinematic opener.
The grounding is the core safety decision. Retrieval is not a feature, it is the guardrail. The model is not free to answer clinical questions from its own head, it answers from NHS text and shows you where the words came from.
Challenges we ran into
- NHS API access is gated. The Content API sits behind an environment allowlist, so the demo runs on cached NHS content as a deliberate fallback while the live integration clears approval. I chose to be explicit about this rather than dress it up.
- Realtime voice doubling. Server voice activity detection and manual response triggers fought each other and produced double replies. Fixed by letting the server own a single response.
- Live transcription rendering. The model heard the user correctly long before her words appeared on screen. The fix was matching the transcription events back to the right message by id, and rebuilding capture so the locale was correct.
- Connection stability. A tunnel that died between sessions was the single biggest risk to the demo, so the backend moved to a deployed Worker on a stable URL.
Accomplishments that we're proud of
- A working voice triage that stays safe. Every clinical word is retrieved from NHS content and shown with its source, so the AI signposts and never diagnoses.
- The advocacy handover. Turning weeks of logged history into a script a woman reads to a midwife is the thing no incumbent does, and it speaks directly to the inquiry's finding of women not being heard.
- Built for the cohort, not retrofitted. Multilingual and surveillance-free were designed in from the start, for the women most likely to be failed.
- Shipped solo in the hackathon, a complete native iOS app with a live realtime voice stack, NHS-grounded answers, one-tap routing, and a cinematic opener.
What we learned
- The hard part is not building, it is restraint. One reliable user journey beats ten half-working features in a three-minute demo. I cut aggressively.
- Grounding changes what an AI is allowed to be. Forcing every clinical word through retrieval, with the source on screen, is what makes a voice model safe enough to point at maternity care at all.
- Equity has to be built in, not bolted on. Surveillance-free and multilingual are not nice-to-haves for this cohort, they are the difference between a woman using the app and never opening it.
- A live realtime voice stack is unforgiving. Audio routing, one-reply-one-voice, live transcription, and a connection that does not drop on venue wifi were where the real engineering time went.
What's next for Artemis
- Clinical validation with a midwife or obstetrician, and a proper safety case before any real-world use.
- A small real-world pilot with a community group serving the cohort Artemis is built for.
A quick note on limitations, stated plainly. Artemis is not a medical device, it is decision support and signposting only. The dangerous failure mode is a false negative, telling a woman she is fine when she is not, so every uncertain verdict is biased upward to manage exactly that. It ships as Health and Fitness, not Medical, with explicit non-diagnostic and crisis disclaimers.
A companion for the women the system fails.
Built With
- api
- claude
- cloudflare
- content
- cursor
- directory
- fotor
- ios
- nhs
- of
- openai
- realtime
- services
- swift
- swiftdata
- swiftui
- webrtc
- website
- workers


Log in or sign up for Devpost to join the conversation.