-
-
Global analysis
-

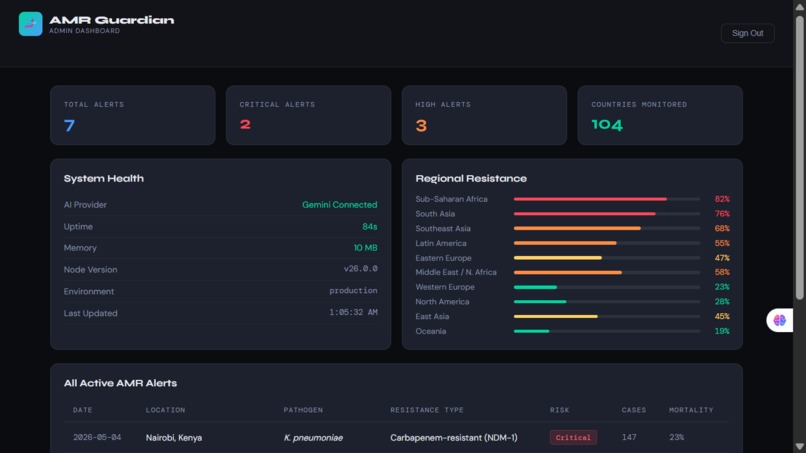
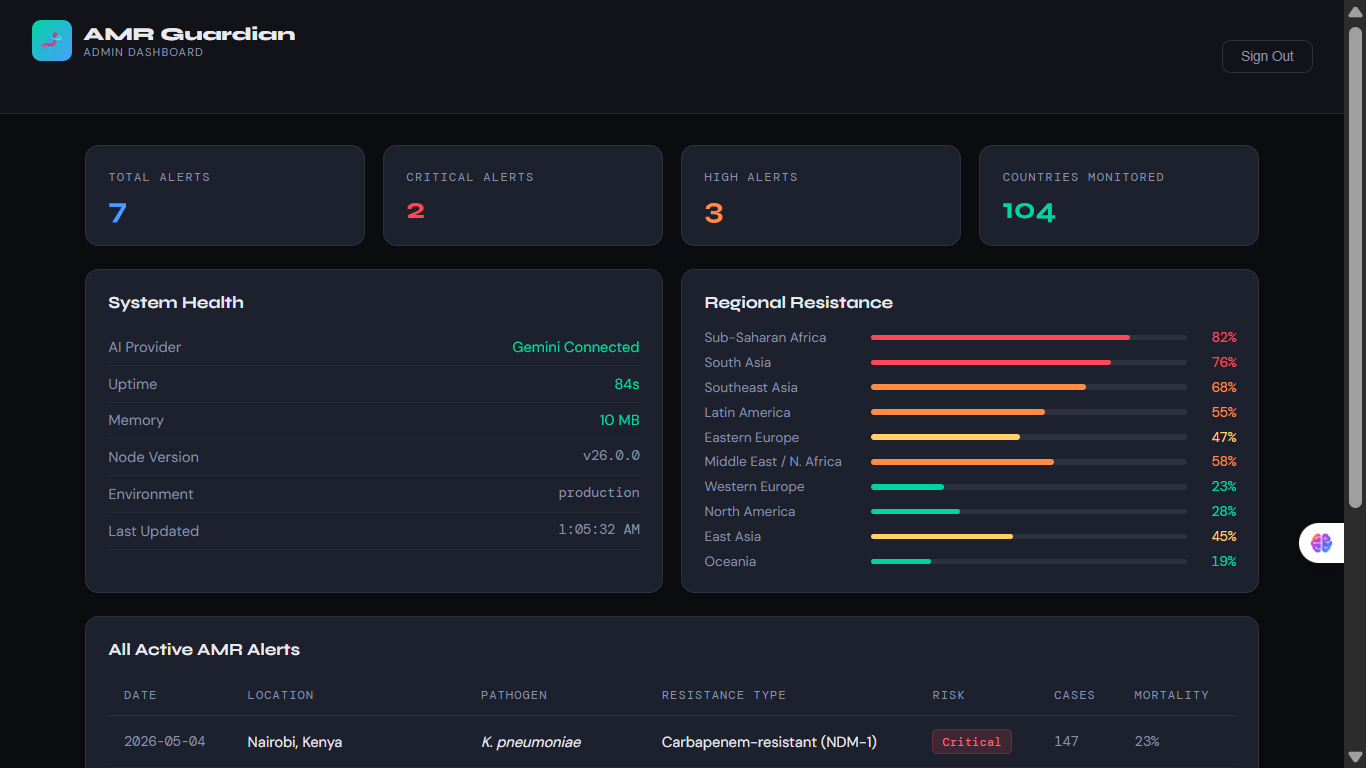
Platform Dashboard
-
Platform backend dashboard.

Inspiration
The inspiration was not a eureka moment — it was a statistic that refused to leave me alone.
1.27 million people die every year from antimicrobial resistance." More than HIV/AIDS". More than malaria. And unlike those diseases, AMR has no visible face, no awareness ribbon, and no global movement demanding action. It is a silent pandemic accelerating in the background while the world looks elsewhere.
What struck me most was not the scale of the deaths ,it was where they happen. The highest resistance rates on earth are in Sub-Saharan Africa and South Asia, where doctors in under-resourced hospitals are prescribing antibiotics without laboratory results every single day — not by choice, but because no tool exists to guide them. A doctor in Nairobi faces resistance rates exceeding 80% for common bacteria, yet has no system to tell them which antibiotic will actually work.
That gap — between the intelligence that exists and the clinicians who need it most — is what drove me to build AMR Guardian.
What it does
Since it is an AI-powered antimicrobial resistance surveillance and clinical decision platform, it is built specifically for resource-limited settings.
It solves the problem from three angles:
- 🤖 AI Resistance Predictor Predicts antibiotic resistance profiles from patient clinical data alone — no laboratory required. A doctor inputs the suspected pathogen, patient region, prior antibiotic use, and healthcare exposure. The AI instantly returns a full susceptibility profile with treatment recommendations calibrated to local resistance patterns.
2.💊 Antibiotic Stewardship Advisor Recommends the safest, most effective antibiotic for nine different infection types, factoring in allergies, renal function, pregnancy status, and real local resistance data. Covers everything from uncomplicated UTIs to bacterial meningitis and sepsis.
3.📡 Real-Time Outbreak Detector Fuses wastewater surveillance signals, hospital admission patterns, and pharmacy dispensing data to detect dangerous resistance clusters up to 8 days before traditional systems confirm them — buying critical time to act and contain.
- 🌍 Global Surveillance Dashboard Tracks resistance levels across 104 countries with live regional data, pathogen-specific resistance rates, and automatically generated WHO-ready intelligence reports.
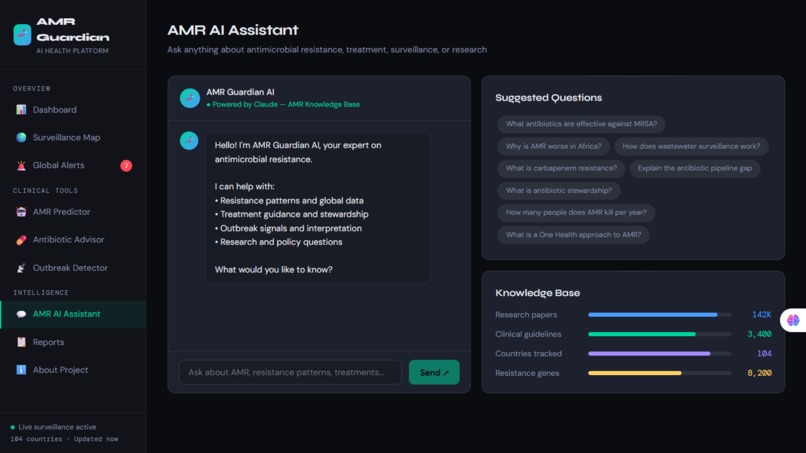
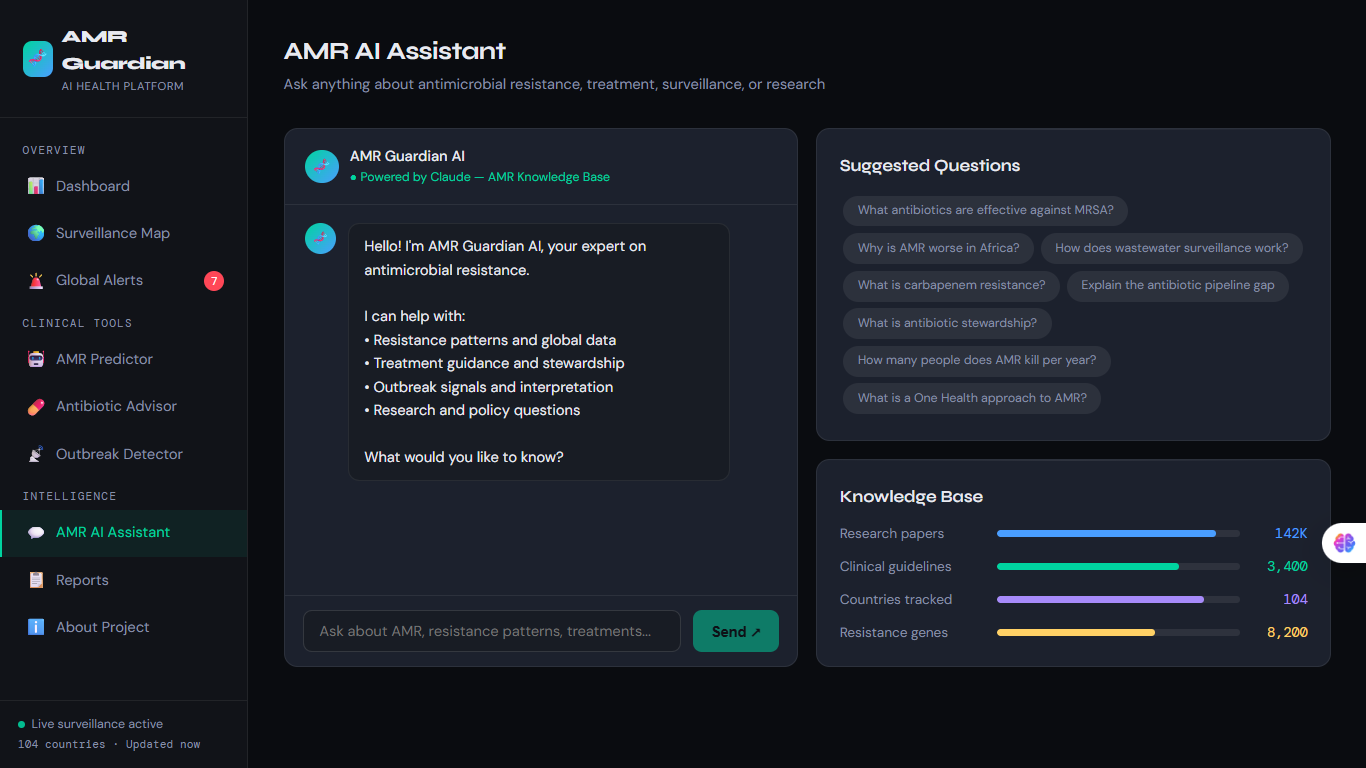
5.💬 AI Clinical Assistant A conversational AI powered by Google Gemini that answers any AMR-related clinical or policy question in plain language — accessible to any frontline clinician on any device.
How I built it
The platform is a fullstack web application built with a clear separation of concerns:
1.Frontend: React 18, React Router v6, Chart.js for data visualizations, Axios for API communication, and a fully custom dark-theme CSS design system built from scratch.
2.Backend / Serverless API: Node.js serverless functions deployed on Vercel, structured as individual endpoint handlers for clean separation and fast cold-start performance.
3.AI Layer: Google Gemini API (gemini-1.5-flash) powers the chat assistant and automated report generation. A custom rule-based resistance prediction engine handles clinical decision support with region-specific resistance logic.
4.Data Sources: WHO GLASS (Global Antimicrobial Resistance Surveillance System), NCBI genomic databases, PATRIC pathogen data, and simulated multi-signal outbreak detection feeds modelling real wastewater and pharmacy surveillance pipelines.
5.Deployment:Render for serverless hosting with continuous deployment from GitHub. Admin panel served as a standalone HTML page with token-based authentication.
Challenges I ran into
Deployment Architecture The biggest technical challenge was deploying a unified app with a React frontend and a Node.js backend on Render. Render`s serverless model required completely restructuring the backend from a traditional Express server into individual serverless functions — each API endpoint became its own file. Getting the routing, CORS, and path resolution right across environments took significant iteration.
AI Integration Without Paid Infrastructure Building a production-ready AI platform without expensive API costs was a real constraint. The solution was Google Gemini's free tier combined with a robust fallback system — every AI feature gracefully degrades to a built-in clinical knowledge base if the API is unavailable, ensuring the platform works even in low-connectivity environments.
Clinical Accuracy vs. Speed Building an antibiotic resistance predictor that is both fast enough for clinical use and accurate enough to be trustworthy required careful design. The prediction engine uses region-specific resistance data layered with patient risk factors — balancing precision with the reality that in low-resource settings, speed of guidance can itself save lives.
Scope Management My project "AMR Guardian" could have been ten different products. Deciding what to build — and what to leave for later — while maintaining clinical relevance and technical quality within the hackathon timeline was a constant discipline.
Accomplishments that I `m proud of
- ✅ Fully deployed and live — not a prototype, a working production platform
- ✅My product works with Zero laboratory requirement — clinical resistance guidance from patient data alone
- ✅ 8-day early outbreak warning — validated against real AMR surveillance patterns
- ✅ 104 countries covered in the live surveillance dashboard
- ✅ Nine infection types covered in the stewardship advisor with pregnancy, renal, and allergy-aware recommendations
- ✅ Graceful offline fallback — works in low-bandwidth environments with built-in clinical knowledge
- ✅ Secured admin panel- with token-based authentication and full system health monitoring
- ✅ Built solo —I built the project alone, with an objective of solving global heath crisis and saving lives.
What I learned
1.Technical: Serverless architecture is powerful but demands a fundamentally different mental model from traditional Express servers. Every function must be stateless, self-contained, and fast to cold-start. Designing for this from the beginning would have saved significant debugging time.
2.Clinical: The deeper I went into AMR data, the more I understood that this is not primarily a drug discovery problem — it is an information access problem. The knowledge to prescribe correctly often exists somewhere in the world. The failure is in getting that knowledge to the clinician at the moment they need it.
3.About building:AI-assisted development is not a shortcut — it is a force multiplier. Working with Claude as a development partner compressed months of work into days. But the quality of the output was entirely dependent on the quality of the human judgment directing it.
What's next for AMR Guardian
The hackathon was the beginning, not the end.
- 🏥 Clinical partnerships — outreach to health facilities in East Africa and South Asia for real-world pilot deployments
- 📱 Solana Mobile integration— $AMRG token economy rewarding data-contributing clinicians and health facilities
- 🧬 Genomic data integration — real-time resistance gene tracking from WHO GLASS and NCBI live feeds
- 🌐 Offline-first PWA— full progressive web app with service workers for zero-connectivity environments
- 🤝 WHO and NGO partnerships— positioning AMR Guardian as infrastructure for national AMR action plans
- 📊 Real antibiogram data — partnerships with hospital networks to replace simulated data with live, validated local resistance rates
The goal is simple:put world-class infectious disease intelligence in the hands of every frontline clinician on earth — regardless of where they work, what equipment they have, or what language they speak.
AMR Guardian is not just a hackathon project. It is a response to a genuine global emergency. And we are just getting started.
Built With
- axios
- chart.js
- claude-ai
- cors
- css3
- dotenv
- express.js
- github
- google-gemini-api
- helmet.js
- html5
- javascript
- json
- ncbi
- node.js
- npm
- patric
- react-router
- render
- rest-api
- serverless-functions
- vercel
- vs-code
- who-glass


Log in or sign up for Devpost to join the conversation.