-
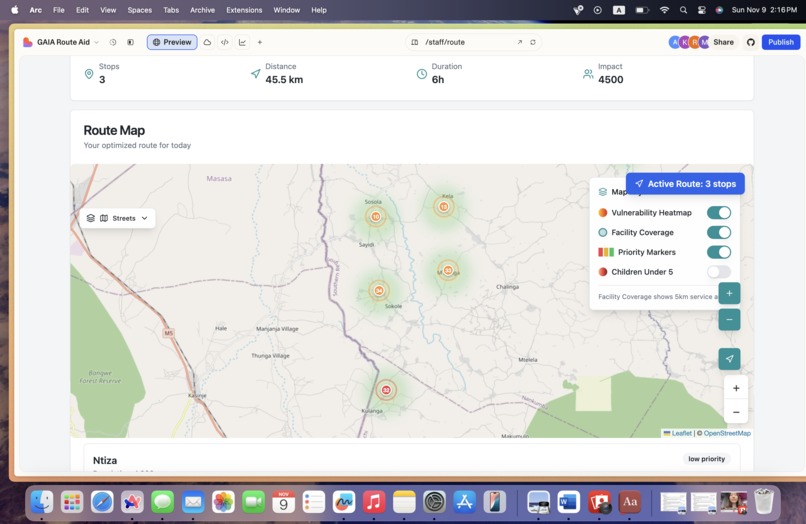
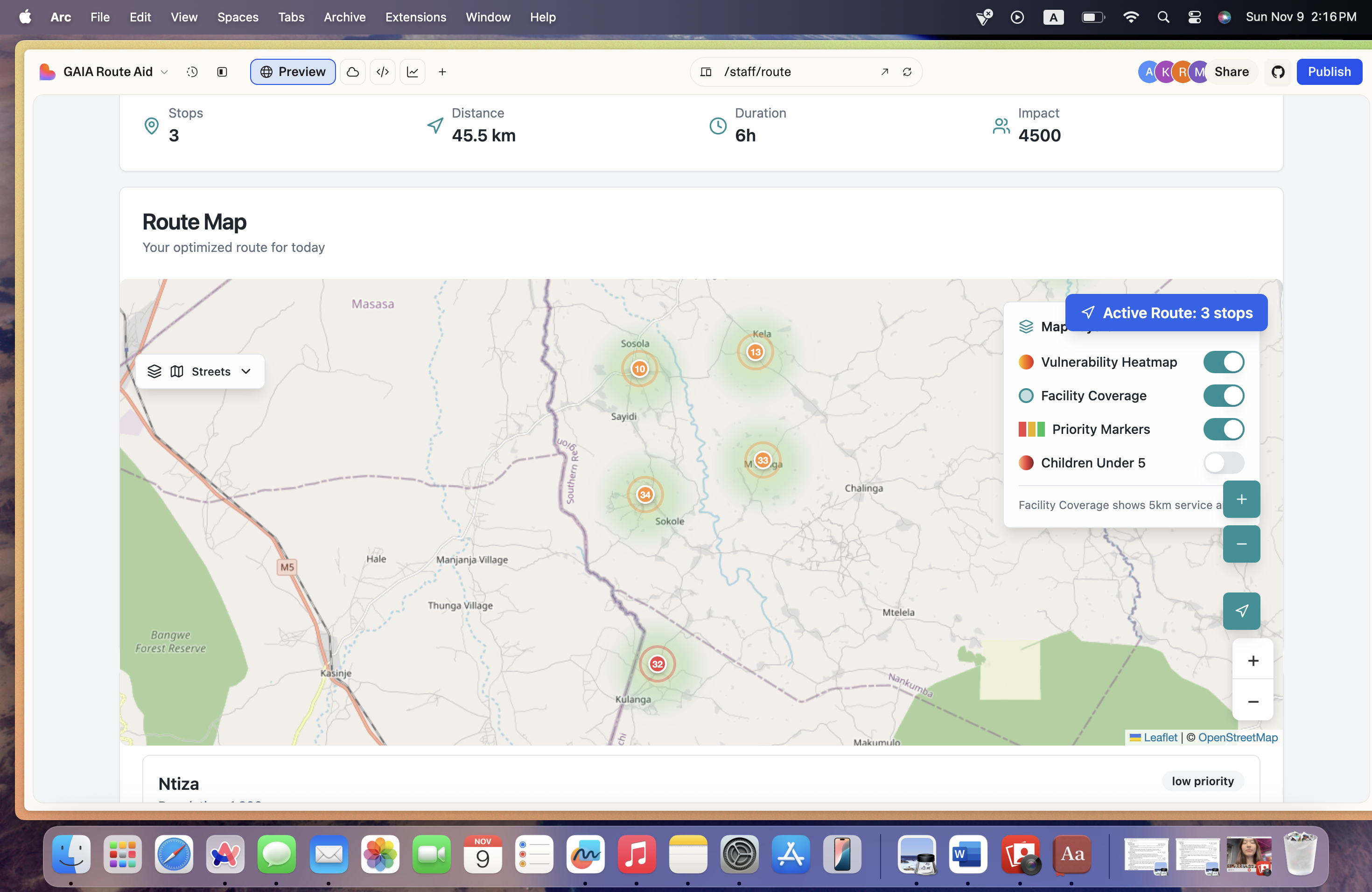
Screenshot of what our website interface looks like
Inspiration
In Malawi, millions of people live far from the nearest clinic, sometimes walking over three hours just to reach basic medical care. When we looked deeper, we found that the challenge isn’t only about distance, but about inefficient distribution: some areas get multiple mobile visits in a week, while others are left completely uncovered. Existing systems rely on outdated data, limited communication, and manual scheduling. We wanted to change that - to build a tool that makes healthcare outreach smarter, fairer, and faster. That’s how AidAtlas was born, a data-driven platform designed to help health organizations like GAIA coordinate their mobile clinics and ensure that no community is left behind.
What it does
AidAtlas is an intelligent mapping system that helps administrators and mobile health staff coordinate field operations in real time. Mobile staff log in with their credentials, register their vehicles, and check in with their location and working hours. Our system then calculates the walking time to the nearest clinic for every region, population density for each of the region, proportion of children under age of 5 and pregnant women, and assigns a priority score Green for less than 1 hour, Yellow for 1–2 hours, and Red for more than 3 hours away. Admins can view this interactive map, click on an uncovered area, and instantly assign a mobile staff vehicle to that location. Each vehicle receives its own unique route, preventing overlap and ensuring that every high-priority area is served first. Once an area is covered, it updates in real time so other teams can see that it’s already being taken care of. AidAtlas doesn’t just show where the clinics are, it shows where care is needed most.
How we built it
We started by analyzing GAIA’s real geographic data, clinic locations, outreach sites, and population clusters. We built a responsive web interface using Lovable’s framework that works seamlessly on mobile devices. On the backend, we integrated a cloud database to store vehicle, user, and area information, and designed a routing algorithm that generates optimal, non-overlapping paths for each staff member. A geospatial engine powers the live map, visualizing walking time, vulnerability level, and assignment status in real time.
Challenges we ran into
The biggest challenge was uploading datasets, because the files were too large We also had to design a priority algorithm that adapts to live updates, for example, if a clinic car suddenly covers an area, it should automatically change color and notify others to avoid duplicate visits. Lastly, ensuring secure authentication for both admins and staff required careful system design. Rural areas often lack stable internet, so we had to make the interface lightweight and able to function offline for short periods.
Accomplishments that we're proud of
We’re proud that AidAtlas can now assign vehicles dynamically, visualize real-time coverage, and make sure every route is unique. In pilot simulations, the system cut redundant travel by up to 40%, allowing the same number of vehicles to reach more patients. We also built a clean, intuitive interface that field staff can actually use without technical training.
What we learned
We learned that data equity is health equity. Even the best medical teams can’t make an impact if they don’t know where the needs are. By connecting geography, population, and logistics in one system, we realized how powerful real-time coordination can be for saving time, and lives.
What's next for AidAtlas
Next, we plan to integrate disease trend data and emergency response alerts so that mobile units can respond instantly to outbreaks or disasters. We’re also exploring machine learning optimization, allowing AidAtlas to predict future hotspots based on travel and treatment history. With GAIA’s support, our goal is to scale AidAtlas across Malawi, and eventually to other regions facing the same challenge of distance, isolation, and inequity. Because healthcare access should never depend on where you live.

Log in or sign up for Devpost to join the conversation.