This project was inspired by patient and surgeon dissatisfaction with all currently available voice restoration techniques for patients with vocal fold (vocal cord) paralysis. Vocal fold (vocal cord) paralysis can be devastating, resulting in an inability to verbally communicate (loss of voice, hoarseness), swallowing difficulty (dysphagia, weight loss), and life threatening occurrences of aspiration pneumonia (from inability of their vocal cords to close and protect their airway during feeding/swallowing). True incidence is unknown, but there appears to be several hundred thousand cases per year, with approximately thirty to forty-thousand new cases of permanent vocal cord paralysis per year (in USA alone).
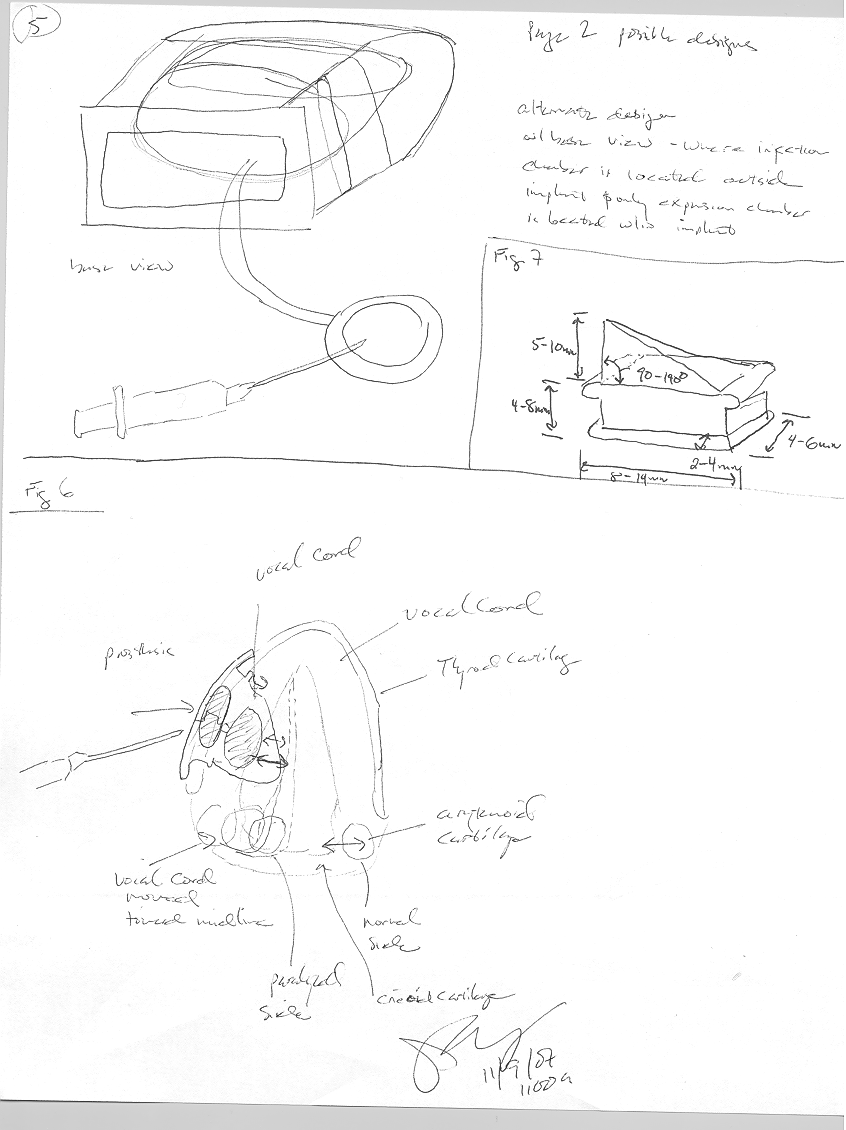
Vocal fold paralysis is caused by many things, including congenital (at birth), infection (viral), inflammatory and other systemic diseases, pharmacologic (chemotherapy), radiation therapy, neoplasms (tumors), trauma, iatrogenic (due to a surgical procedure ), and idiopathic (unknown cause ). In cases where there is little chance of recovery in vocal cord function, a procedure called medialization thyroplasty may be performed. In this procedure, an implant is placed within the paralyzed vocal cord. The implant gives the weakened vocal cord more bulk and moves it toward the normal functioning vocal cord on the opposite side of their larynx (voice box). By doing this, the patient's vocal cords can come into full contact again, similar to a normally functioning larynx (voice box).
Current thyroplasty implants come in several sizes, but are not adjustable. Once a size is chosen in the operating room, it cannot be changed without a repeat surgical procedure. This lack of flexibility brings about several challenges. If the implant chosen is too small and the patient’s voice remains breathy or weak, a revision procedure may be required. Secondly, in cases where the implant is too large and the patient is overcorrected, he or she may require an emergency revision or even a life-saving tracheotomy procedure. Currently, the implant size is chosen based on the patient's voice at the time of surgery. Unfortunately, the patient’s voice typically changes during the weeks after the primary surgery (due to vocal fold and generalized swelling from the surgery subsiding). In some cases, these changes may transform an initially voice result into a suboptimal voice.
Our goal is to dramatically advance current thyroplasty implant technique by developing a simple, cost-effective, and safe adjustable implant. In doing so, surgical results could be individualized and improved. Mortality and morbidity could be decreased, patient satisfaction could be improved and the need for further procedures minimized.
Built With
- 3d-printing
- poweroint
- silicone


Log in or sign up for Devpost to join the conversation.