Inspiration
Patient and surgeon dissatisfaction with all currently available voice restoration techniques for patients with vocal cord paralysis.
How it works
Vocal fold (vocal cord) paralysis can be devastating, resulting in an inability to verbally communicate (loss of voice, hoarseness), swallowing difficulty (dysphagia, weight loss), and life threatening occurrences of aspiration pneumonia (from inability of their vocal cords to close and protect their airway during feeding/swallowing). True incidence is unknown, but there appears to be several hundred thousand cases per year, with approximately thirty to forty-thousand new cases of permanent vocal cord paralysis per year.
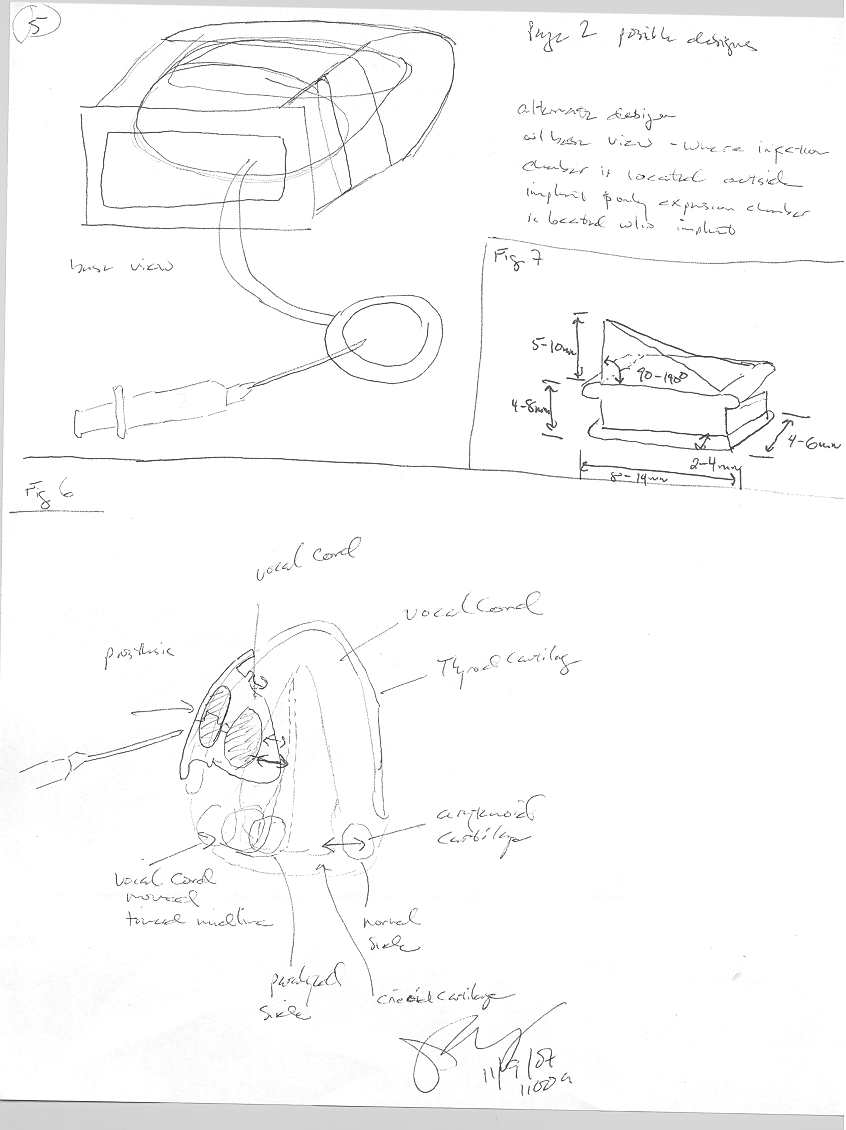
Vocal fold paralysis is caused by many things, including congenital (at birth), infection (viral), inflammatory and other systemic diseases, pharmacologic (chemotherapy), radiation therapy, neoplasms (tumors), trauma, iatrogenic (due to a surgical procedure ), and idiopathic (unknown cause ). In cases where there is little chance of recovery in vocal cord function, a procedure called medialization thyroplasty may be performed. In this procedure, an implant is placed within the paralyzed vocal cord. The implant gives the weakened vocal cord more bulk and moves it toward the normal functioning vocal cord on the opposite side. By doing this, the patient's vocal cords can come into full contact again, similar to a normally functioning larynx (voice box).
Current thyroplasty implants come in several sizes, but are not adjustable. Once a size is chosen in the operating room, it cannot be changed without a repeat surgical procedure. This lack of flexibility brings about several challenges. If the implant chosen is too small and the patient’s voice remains breathy or weak, a revision procedure may be required. Secondly, in cases where the implant is too large and the patient is overcorrected, he or she may require an emergency revision or even a life-saving tracheotomy procedure. Currently, the implant size is chosen based on the patient's voice at the time of surgery. Unfortunately, the patient’s voice typically changes during the weeks after the primary surgery (due to vocal fold and generalized swelling from the surgery subsiding). In some cases, these changes may transform an initially voice result into a suboptimal voice.
Our goal is to dramatically advance current thyroplasty implant technique by developing a simple, cost-effective, and safe adjustable implant. In doing so, surgical results could be individualized and improved. Mortality and morbidity could be decreased, patient satisfaction could be improved and the need for further procedures minimized.
Challenges I ran into
Determining the optimal injection material. Needs to be biodegradable, have adequate viscosity for optimal vocal cord vibration while being thin enough for easy withdrawal/removal if needed. The implant design must be able to control the direction of implant expansion with injection of the medium. A simplified comparison would be modifying the size and shape of a breast implant, tissue expander, or balloon.
Accomplishments that I'm proud of
This project has fostered a collegial attitude within the Otolaryngology department. Additionally, it has been a great opportunity to learn more about the unique challenges found in product design and development within the medical field.
What I learned
This projected has taught me how important it is to leverage the skill and knowledge base of those around you to optimize project results and fill competency gaps. This project also helped me realize my interest in healthcare development and I look forward to pursuing other ideas I have in the future.
What's next for Adjustable Thyroplasty Implant
The estimated time to market is 1-2 years. Our prototype implant designs will need to be tested either using computation models or through and animal/cadaver study to gather more data and refine the design prior to production. Once patenting and proof of concept is completed, it will need to pass all necessary safety parameters as a synthetic implant designed for use in humans. The current design uses already well accepted materials, and we do not expect this process to be a significant burden. The product will most likely be marketed and licensed to a medical device company for production and sales. Sales would likely be pursued initially at larger academic centers with robust laryngology subspecialty practices. After which, expansion into any hospital system which retains an Otolaryngologist (ENT physician) whom performs surgical procedures would be possible. This procedure is performed throughout the world, and the market for the implant is expected to be international, following the same clientele requirements as described above.
Although a true production cost has not yet been identified, this implant is relatively simple in design and is not expected to require any high cost materials. Because of this, we would anticipate a very appealing profit margin once development and proof of concept has been completed.

Log in or sign up for Devpost to join the conversation.