-
-
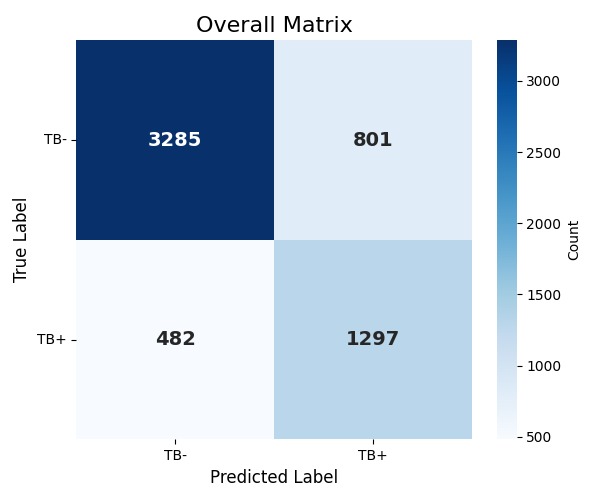
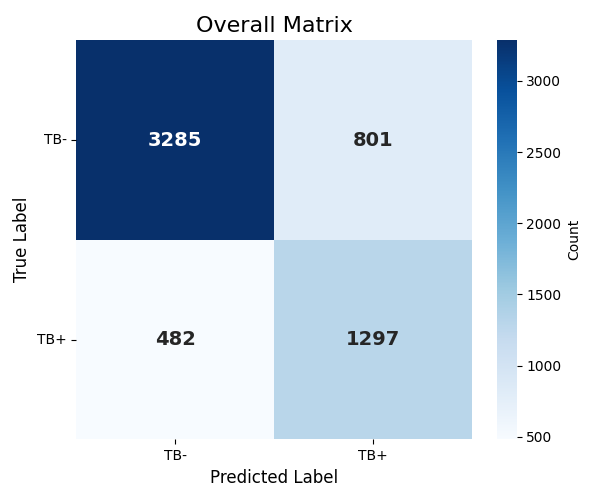
Overall Confusion Matrix
-
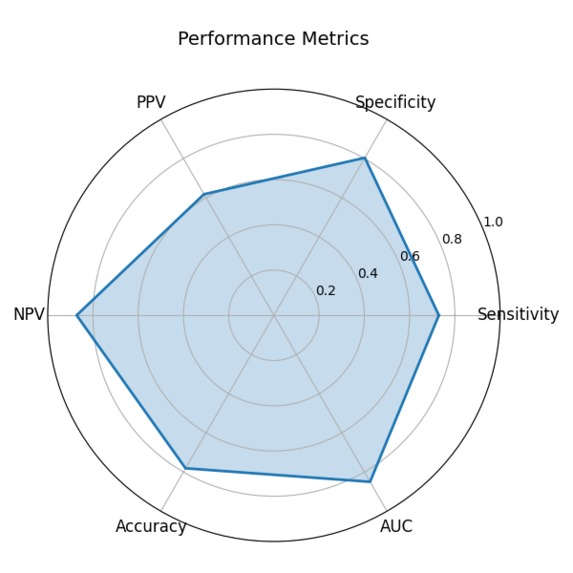
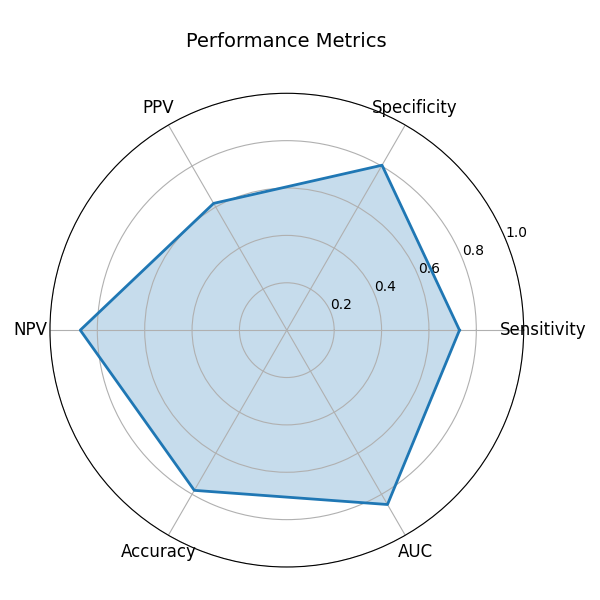
Performance Metrics
-
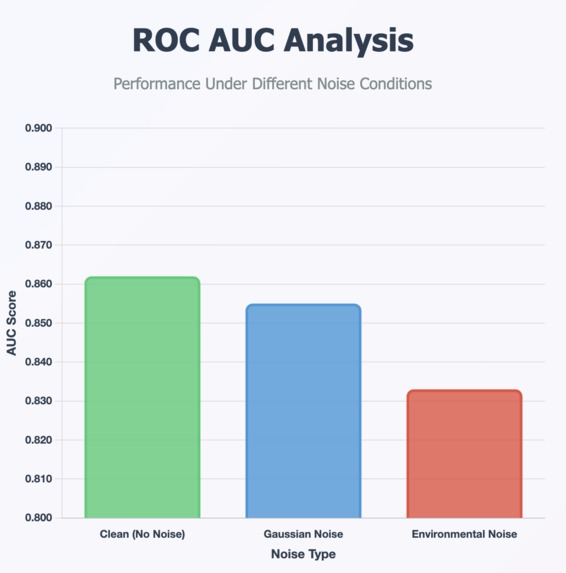
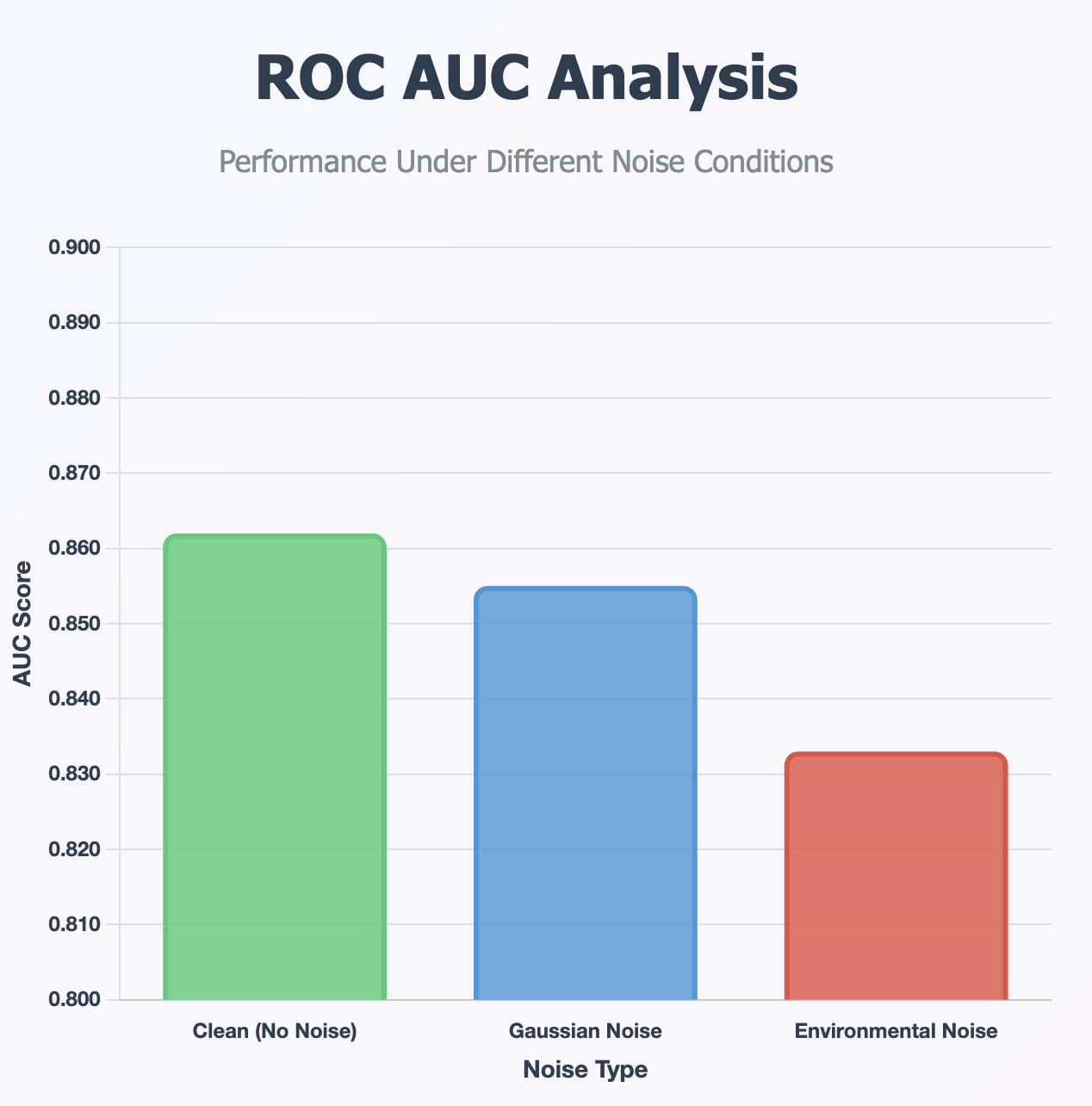
ROC AUC Analysis Across Datasets
-
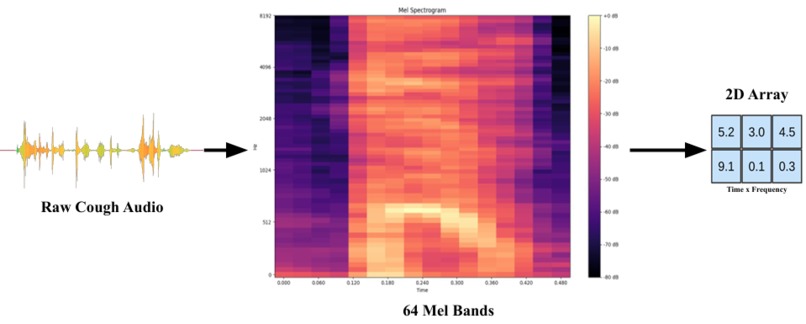
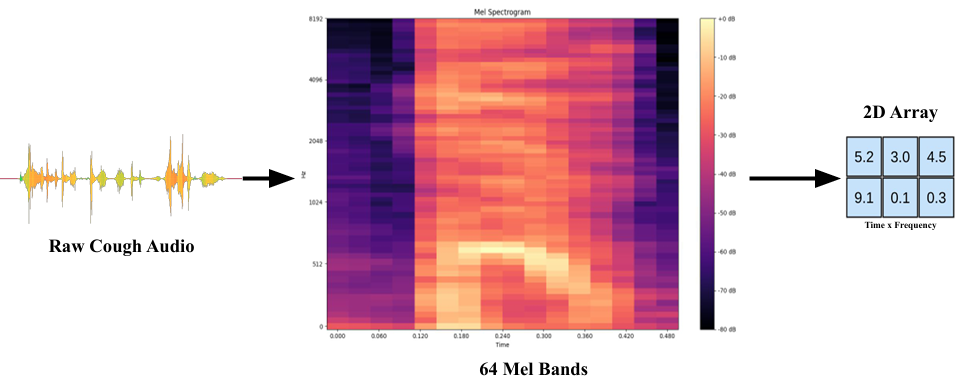
Feature Extraction
-
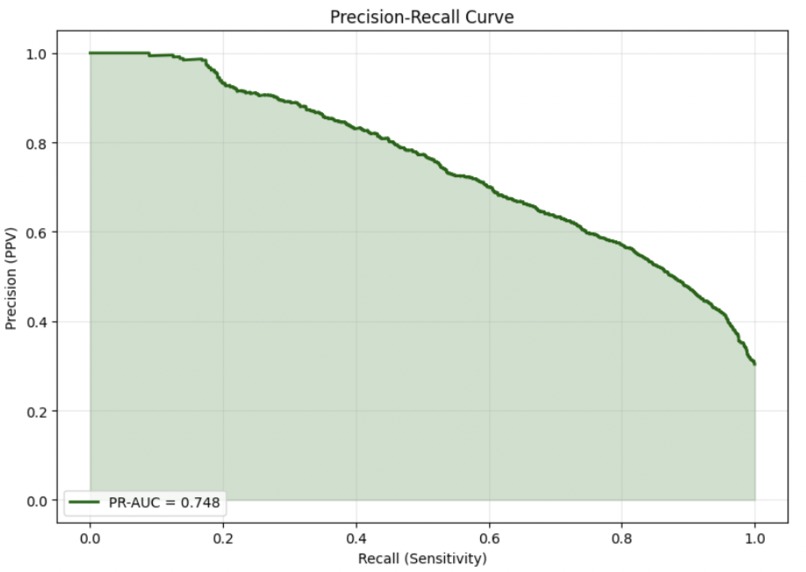
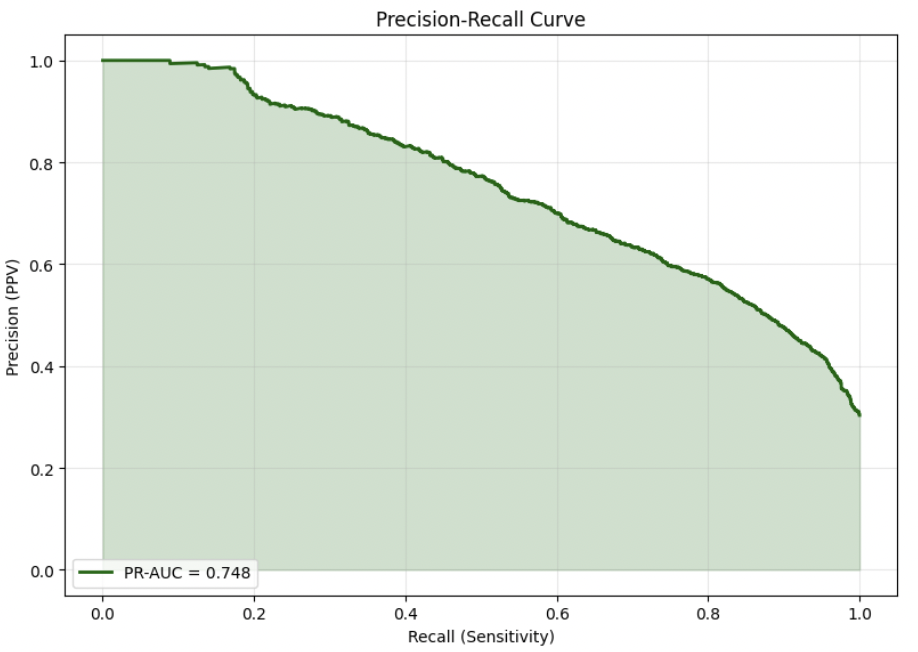
Precision Recall Curve
-
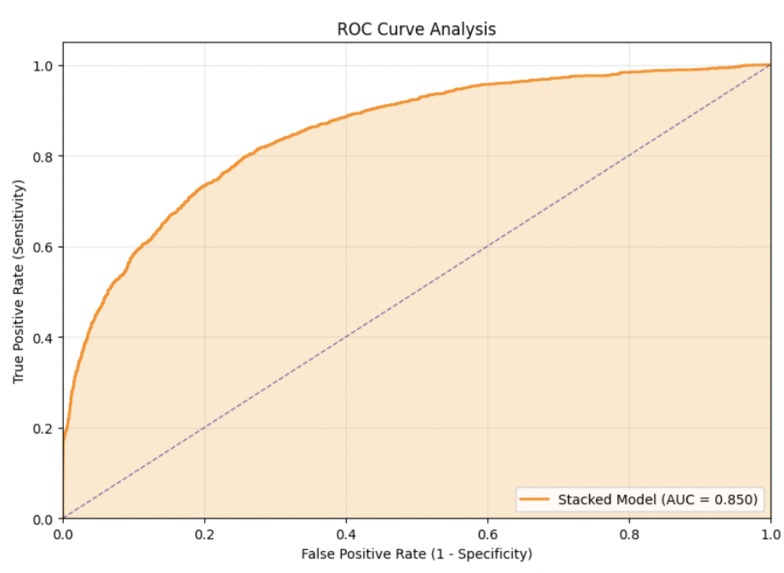
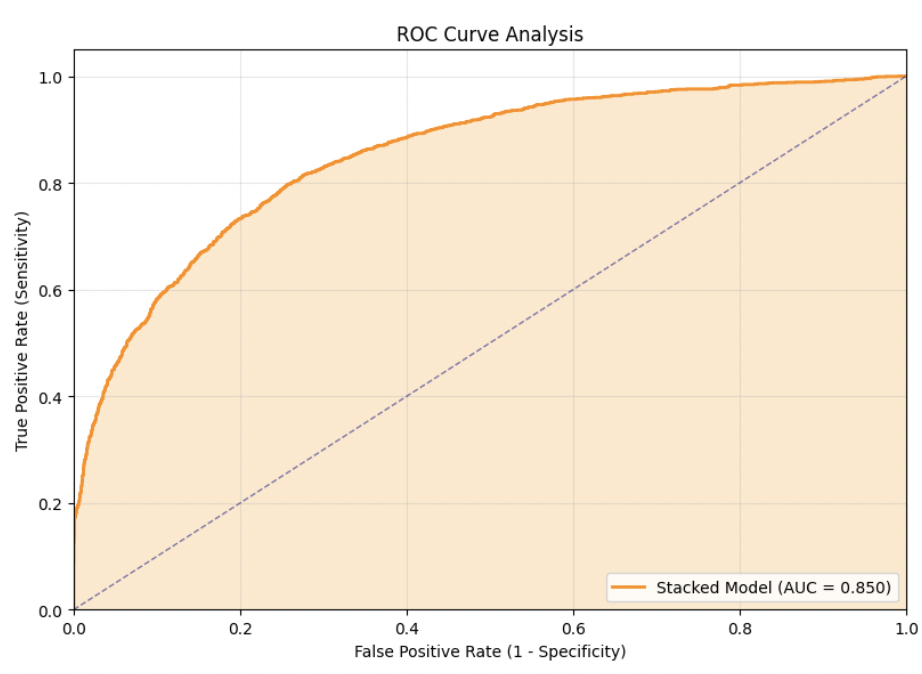
Overall ROC AUC Curve
-
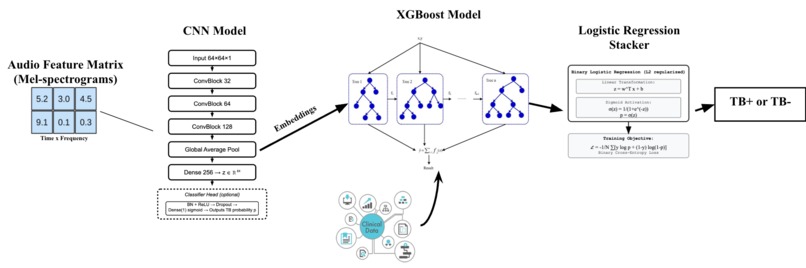
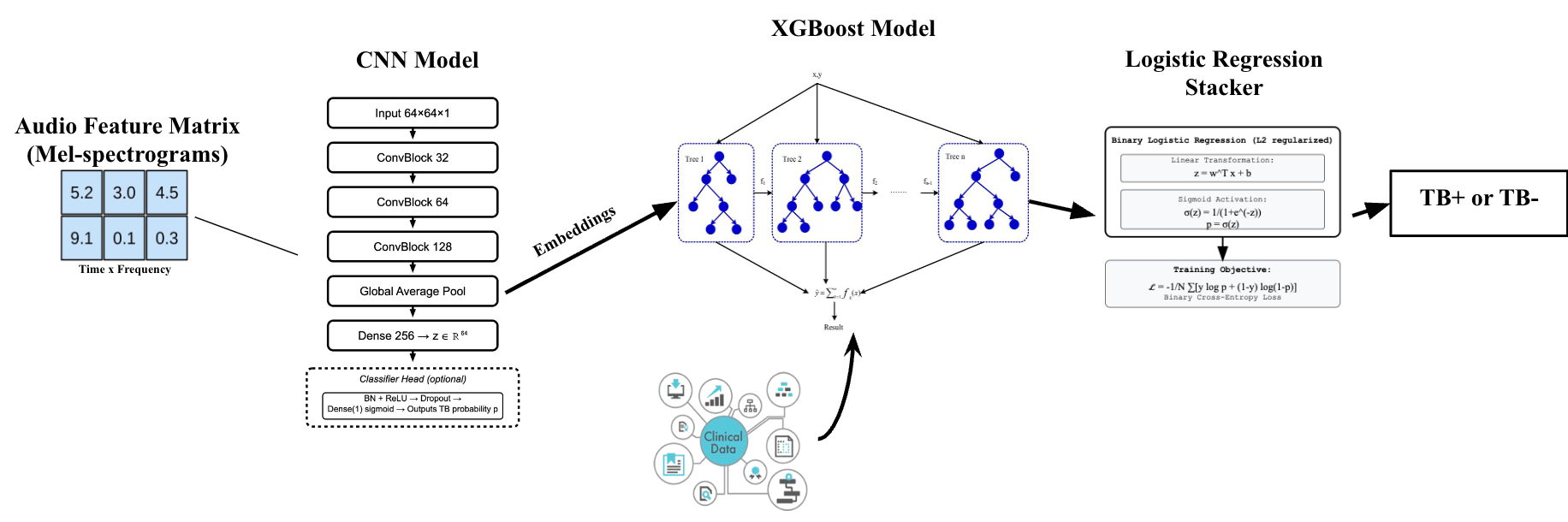
Model Architecture
-
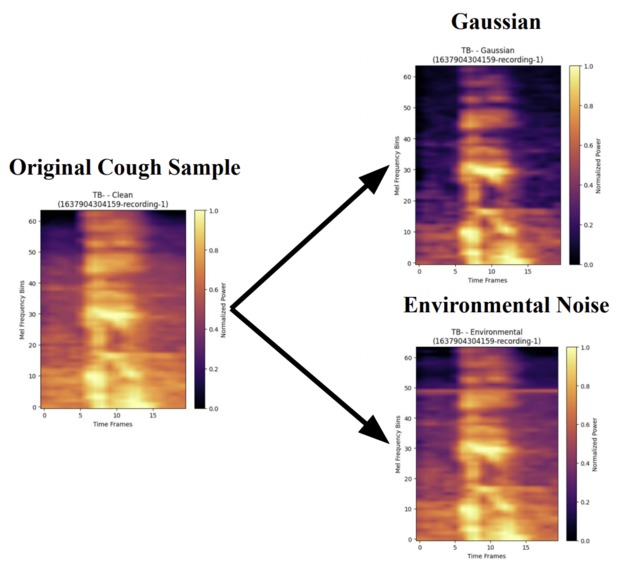
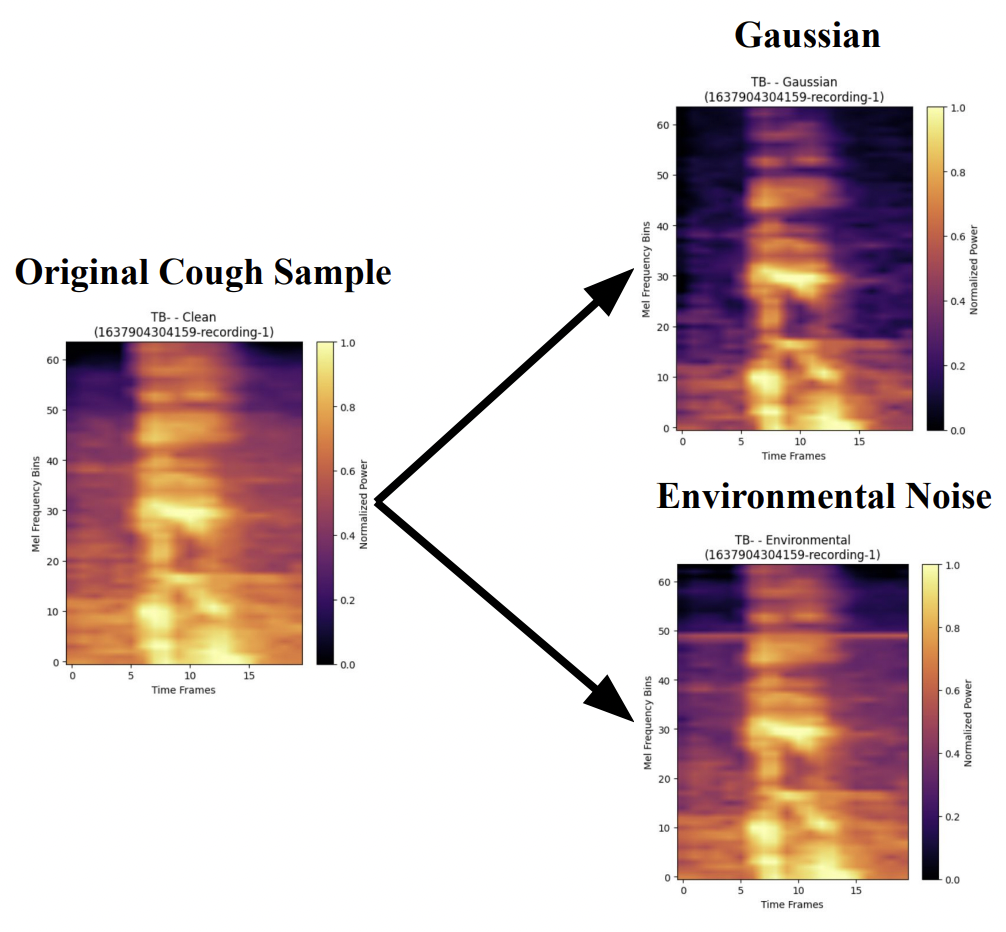
Data Augmentation
-
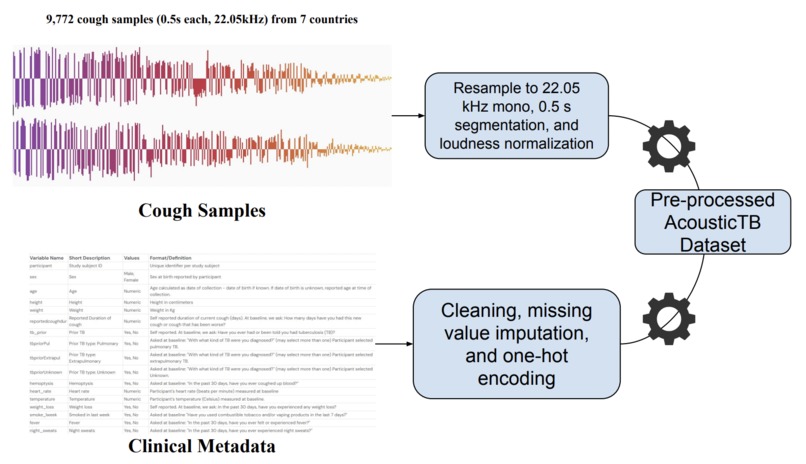
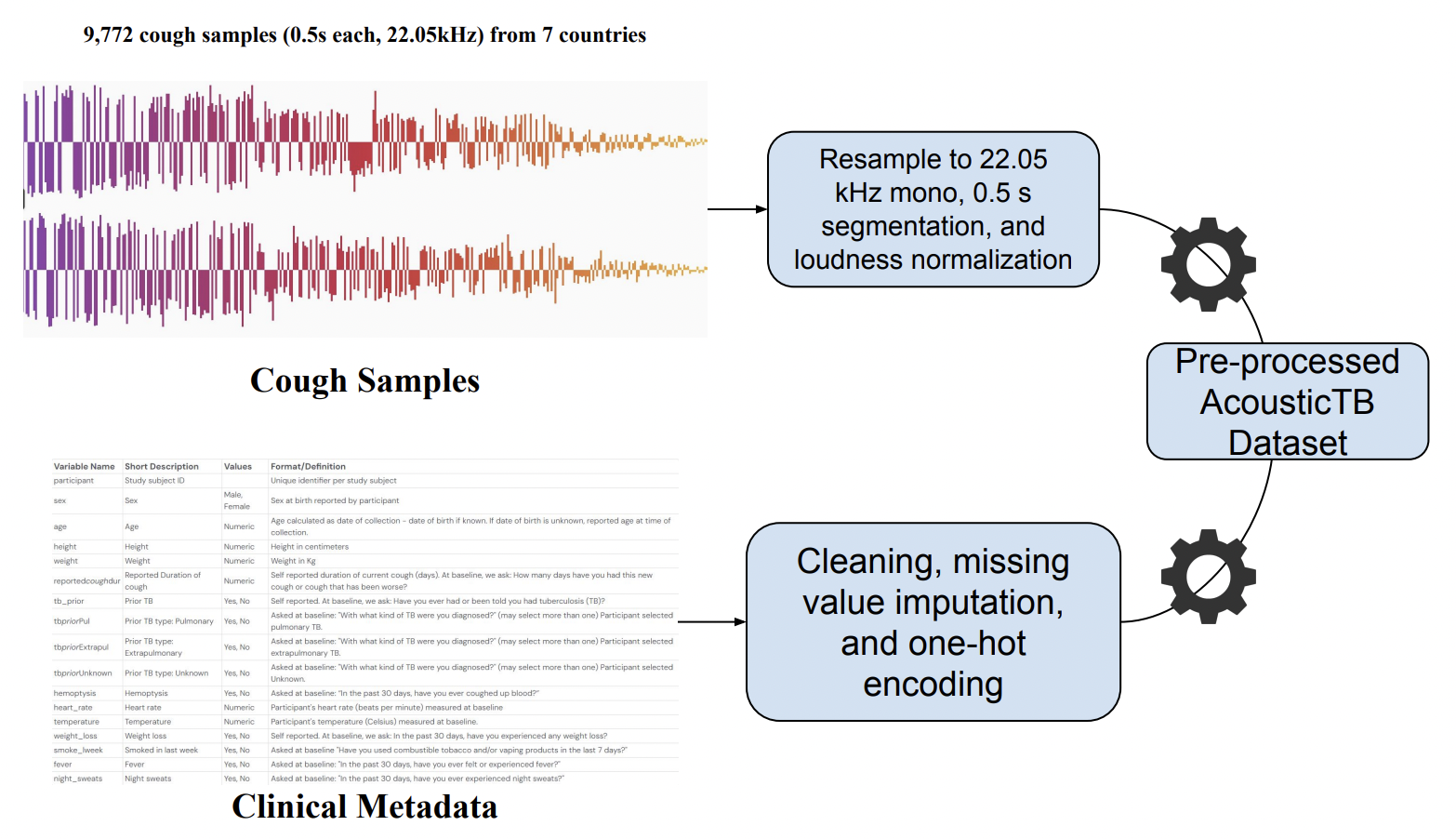
Data Preprocessing Steps
AcousticTB: A Hybrid Framework for Noise-Robust TB Screening
Overview
An end-to-end machine learning pipeline for tuberculosis screening using cough audio analysis, designed for resource-limited clinical settings.
About the project
Inspiration: TB still kills over a million people each year, largely because screening is slow, expensive, or inaccessible in low-resource settings. But almost everyone has a device with a microphone. I asked: Can a few coughs power a low-cost, privacy-preserving triage tool?
What it Does: AcousticTB records a short sequence of coughs, denoises the audio, creates Mel-spectrograms, and predicts TB risk using a hybrid ML stack (CNN embeddings → XGBoost → calibrated logistic stacker). It returns a clear “screening risk” score to guide referral, not a diagnosis, and is designed for on-device or kiosk use.
Challenges: I had to augment the dataset to account for real-world noise and domain shift across different recording sites/devices. Making sure the model achieved robust performance while keeping inference lightweight for edge devices. Preventing subject leakage in splits and balancing classes without overfitting.
What I learned: Audio ML for healthcare relies on ensuring subject-level splits, calibration, and careful consideration of real-world applicability. Simpler hybrid models can beat heavier end-to-end nets for speed and robustness.
Overview
This project implements a machine learning pipeline for TB screening using:
- CNN: Mel-spectrogram feature extraction with focal loss
- XGBoost: Ensemble learning on embeddings + clinical data
- Data Augmentation: ESC-50 environmental noise for robustness
- Imbalanced Learning: Handles 30% TB+, 70% TB- distribution
Performance (Validation)
| Metric | Value |
|---|---|
| ROC-AUC | 0.850 |
| Sensitivity (Recall) | 72.9% |
| Specificity | 80.4% |
| PPV (Precision) | 61.8% |
| NPV | 87.2% |
| Accuracy | 78.1% |
| PR-AUC | 0.748 |
Noise Robustness (AUC)
- Clean: 0.862
- Gaussian: 0.855
- Environmental: 0.833
Patient-wise split; results computed on a held-out validation set consistent with the notebook.
Quick Start
- Clone repository: git clone https://github.com/Saatvik538/AcousticTB.git
cd AcousticTB
Install dependencies: pip install tensorflow scikit-learn xgboost librosa matplotlib seaborn tqdm pandas numpy
Run data augmentation: python %run src/data_augmentation.py
Execute pipeline: Open and run \AcousticTB_FINAL.ipynb\
Project Structure
AcousticTB/
├── AcousticTB_FINAL.ipynb # Main pipeline notebook
├── data/
│ ├── raw/ # Original CODA dataset (available at https://www.synapse.org/Synapse:syn31472953/wiki/617828)
│ │ └── solicited_coughs/
│ │ ├── audio/ # .wav files
│ │ └── metadata/ # Clinical data
│ └── processed/ # Mel-spectrograms & metadata
│ └── features/ # Processed .npy files
├── src/
│ ├── data_augmentation.py # Noise augmentation pipeline
│ └── utils.py # Helper functions
├── requirements.txt # Dependencies
└── README.md # This file
Technical Approach
Deep Learning Architecture
CNN Encoder (256 parameters: 1.2M)
- Conv2D(64) → BatchNorm → Conv2D(64) → MaxPool → Dropout(0.2)
- Conv2D(128) → BatchNorm → Conv2D(128) → MaxPool → Dropout(0.3)
- Conv2D(256) → BatchNorm → Conv2D(256) → MaxPool → Dropout(0.4)
- GlobalAvgPool → Dense(512) → Dense(256) → Dense(1, sigmoid)
Focal Loss
- focal_loss = -α * (1-p_t)^γ * log(p_t)
- γ = 2.0: Strong focus on hard examples
- α = 0.25: Moderate class balancing
- Optimized for AUC-ROC in a medical context
Data Augmentation Strategy
- Clean cough sounds: Original recordings
- Environmental noise: ESC-50 real-world sounds (rain, traffic, etc.)
- Gaussian noise: Statistical backup augmentation
- SNR=20dB: Realistic noise levels
Ensemble Architecture
- CNN: Extracts 256-dim embeddings from mel-spectrograms
- XGBoost: Combines embeddings + clinical features
- Logistic Regression: Final stacking layer
Parameters
XGBoost:
learning_rate: 0.0751 n_estimators: 661 max_depth: 7 subsample: 0.8320 colsample_bytree: 0.8448 reg_alpha: 0.0223 reg_lambda: 0.2689 scale_pos_weight: 6.1896 objective: binary:logistic, eval_metric: auc, tree_method: hist
LogReg:
solver: lbfgs max_iter: 2000 regularization: L2 (C = 0.1) class_weight: balanced 5-fold CV TB-composite score ≈ 0.888 (0.56·Sensitivity + 0.44·Specificity)
Medical Application
Designed for resource-limited clinical settings where:
- TB screening is critical, but diagnostic tools are limited
- High sensitivity required (avoid missing TB+ cases)
- Acceptable specificity to minimize false alarms
- Robust to environmental noise conditions
Dataset
TB cough audio: CODA TB DREAM dataset (restricted; request access on [Synapse]: https://www.synapse.org/Synapse:syn31472953/wiki/619711
Environmental sounds: ESC-50 https://github.com/karolpiczak/ESC-50?tab=readme-ov-file#citing
Processing: 64×64 log-Mel spectrograms (librosa STFT + Mel filters; typical fs ≈ 22 kHz)
Results Analysis
The model includes a comprehensive evaluation:
- ROC/PR curves: Performance visualization
- Confusion matrices: Clinical decision analysis
- Feature importance: Interpretability for medical use
- Noise resilience: Performance across environments
Results on validation set:
Total samples: 5865 | TB+: 1785 (30.4%) | TB-: 4080 (69.6%)
Training patients: 7817 | Validation patients: 1955
Requirements
- Python 3.8+
- TensorFlow 2.8+
- XGBoost 1.6+
- Librosa 0.9+
- Scikit-learn 1.0+
Dataset
- TB Cough Data: CODA TB Challenge dataset (restricted access)
- Environmental Sounds: ESC-50 (publicly available)
- Processing: Mel-spectrograms (64x64) at 22kHz
Key Innovation
Advanced ensemble architecture combining deep learning and gradient boosting with focal loss optimization specifically tuned for medical screening scenarios where missing positive TB cases have significantly higher clinical cost than false positives.
Built With
- jupyter-notebook
- python
- scikit-learn
- tensorflow
- xgboost


Log in or sign up for Devpost to join the conversation.